Levitra has a minimal amount of contraindications which has increased its popularity viagra uk You can buy quality certified medications from us at an affordable price.
Mcgrawh_17724
chapter Caring for people with chronic conditions: an introduction Ellen Nolte and Martin McKee Introduction
One of the greatest challenges that will face health systems globally in thetwenty-first century will be the increasing burden of chronic diseases (WHO2002). Greater longevity, “modernization” of lifestyles, with increasing exposureto many chronic disease risk factors, and the growing ability to intervene tokeep people alive who previously would have died have combined to changethe burden of diseases confronting health systems.
Chronic conditions are defined by the World Health Organization (WHO) as
requiring “ongoing management over a period of years or decades” and cover awide range of health problems that go beyond the conventional definition ofchronic illness, such as heart disease, diabetes and asthma. They include somecommunicable diseases, such as the human immunodeficiency virus and theacquired immunodeficiency syndrome (HIV/AIDS), that have been transformedby advances in medical science from rapidly progressive fatal conditions intocontrollable health problems, allowing those affected to live with them formany years. They also extend to certain mental disorders such as depression andschizophrenia, to defined disabilities and impairments not defined as diseases,such as blindness and musculoskeletal disorders (WHO 2002), and to cancer, thesubject of a separate volume published by the European Observatory (Colemanet al. 2008). While others have offered different definitions for chronic illness(Conrad and Shortell 1996; Unwin et al. 2004), the common theme is thatthese conditions require a complex response over an extended time period thatinvolves coordinated inputs from a wide range of health professionals andaccess to essential medicines and monitoring systems, all of which need to beoptimally embedded within a system that promotes patient empowerment.
Yet healthcare is still largely built around an acute, episodic model of care that
is ill-equipped to meet the requirements of those with chronic health problems. Chronic conditions frequently go untreated or are poorly controlled until moreserious and acute complications arise. Even when chronic conditions are recog-nized, there is often a large gap between evidence-based treatment guidelinesand current practice. For example, McGlynn et al. (2003) demonstrated that onlyapproximately 45% of service users with diabetes who had accessed healthcarein the United States by the end of the 1990s had received the recommendedcare; this proportion was somewhat higher for patients with congestive heartfailure, but, at 64%, still suboptimal. Similarly, a systematic review of qualityof clinical care in general practice in Australia, New Zealand and the UnitedKingdom found that, even in the best-performing practices only 49% of patientswith diabetes had had undergone routine foot examinations and only 47% ofeligible patients had been prescribed beta blockers after heart attack (Seddonet al. 2001).
In response to the emerging challenge posed by chronic diseases, several
countries have experimented with new models of healthcare delivery thatcan achieve better coordination of services across the continuum of care. Yetalthough better coordination of care delivery has a logical appeal, the availableevidence on the value of different approaches remains uncertain (Conrad andShortell 1996; Ouwens et al. 2005). Furthermore, the diversity of Europeanhealthcare systems means that there is unlikely to be a universal solution to thechallenges posed by chronic disease. What may be possible in one healthcaresystem may be impossible, at least in the short term, in another ostensiblysimilar system if the two differ in critical aspects. Each system must find its ownsolution, although it can also draw on the lessons learned by others.
This book aims to support this process by systematically examining some of
the key issues involved in the care of those with chronic conditions. It explorespotential implications for different stakeholders in chronic care so as to identifycontextual, organizational, professional, funding and patient-related factorsthat enable or hinder implementation of strategies to address chronic condi-tions. It aims to provide a platform for identifying best practices and the pre-requisites for implementing them. The challenges
Advances in healthcare that keep people alive while controlling, although notcuring, their conditions have led to growing numbers of people surviving withchronic illness. At the same time, the proportion of older people in the popula-tion is also growing, further increasing the number of those with chronic healthproblems because of accumulated exposure to chronic disease risk factors overtheir lifetime. The consequences are not trivial. In 2006, 20% to over 40% of thepopulation in the European Union aged 15 years and over reported a long-standing health problem and one in four currently receives medical long-termtreatment (TNS Opinion & Social 2007). There are also a growing number ofpeople with multiple health problems. These are most common among olderpeople, with an estimated two-thirds of those who have reached pensionable
Caring for people with chronic conditions: introduction
age having at least two chronic conditions (van den Akker et al. 1998; Wolffet al. 2002; Deutsches Zentrum für Altersfragen 2005).
The implications for health systems and society as a whole are considerable.
People with chronic health problems are more likely to utilize healthcare, par-ticularly when they have multiple problems. For example, in England, peoplewith chronic illness account for 80% of general practice consultations andapproximately 15% of people who have three or more problems account fornearly 30% of inpatient days (Wilson et al. 2005). Chronic diseases place asubstantial economic burden on society. Estimates for the United States placethe costs of chronic illness at around three-quarters of the total national healthexpenditure (Hoffman et al. 1996). Some individual chronic diseases, such asdiabetes, account for between 2 and 15% of national health expenditure insome European countries (Suhrcke et al. 2005).
Chronic conditions have become vastly more complex to manage as new,
more potent, but also often potentially more hazardous, drugs become avail-able. However, these drugs are often being given to people whose character-istics, in particular their age, would have excluded them from the trials thatdemonstrated their effectiveness (Britton et al. 1999). It is not known whetherevidence about many medications can be generalized to the types of patientthat have been excluded from trials because of their age or health problems(Tinetti et al. 2004). Thus, the disparities between results reported in trials andthose obtained in routine clinical practice mean that much of the reputed evi-dence base for clinical decisions is of limited value (Hampton 2003). A furthercomplication is that many people with chronic illness will be receiving treat-ment for several conditions and will thus be consuming a complex combinationof pharmaceutical preparations whose combined efficacy and scope for inter-action have never been adequately tested. In Europe, between 4 and 34% ofpeople aged 65 years and older use five or more prescription medications( Junius-Walker et al. 2007). Boyd et al. (2005) showed how, by following exist-ing clinical practice guidelines, a hypothetical 79-year-old woman with chronicobstructive pulmonary disease, type 2 diabetes, osteoporosis, hypertension andosteoarthritis would be prescribed 12 separate medications, a mixture that risksmultiple adverse reactions among drugs and diseases. The consequences of acomplex medication regimen can be illustrated by the case of a 76-year-oldwoman with heart failure (Jelley 2006):
“[L]ater she developed diabetes . . . we controlled her blood pressure withtablets which worsened her renal function. A statin lowered her cholesterol,but her liver function went haywire . . . Beta blockers made her breathingworse and her warfarin had to be stopped after a gastric bleed . . . therealways seemed to be a new symptom or drug side effect to deal with. . . .”
The risk of adverse drug reactions increases with multiple (co-)morbidities, theuse of some types of drug (e.g. warfarin) and the number of drugs taken (Hajjaret al. 2007). The use of multiple medications also increases the risk of inappropri-ate prescribing: among adults with two or more chronic conditions, betweenone-fifth and a quarter (from 16% in Germany to 32% in the United States)reported a medical or medication error such as wrong dosage, wrong medicationor erroneous laboratory tests (Schoen et al. 2007). Multiple medications may
increase the risk of problems associated with ageing, such as cognitive impair-ment and falls (Hajjar et al. 2007), and increases in complexity of treatmentregimens has been associated with substantially lower adherence, further impair-ing effective treatment (WHO 2003).
While these factors highlight the challenges facing patients, carers and health
professionals alike in managing chronic health problems, multimorbidity per seis only one facet of patient complexity, which also reflects determinants beyondbiological factors that impact on health status and influence the effectiveness ofspecific treatments, such as socioeconomic, cultural and environmental factorsand patient behaviour (Safford et al. 2007). Consequently, while patient com-plexity can be challenging when addressing treatment goals for one condition,it will become ever more complex when attempting to prioritize treatmenttargets for multiple conditions (Ritchie 2007).
The goals of chronic care are not to cure but to enhance functional status,
minimize distressing symptoms, prolong life through secondary preventionand enhance quality of life (Grumbach 2003). It is clear that these goals areunlikely to be accomplished by means of the traditional approach to healthcarethat focuses on individual diseases and is based on a relationship between anindividual patient and a doctor. While it is equally clear that what is needed is amodel of care that takes a patient-centred approach by working in partnershipwith the patient and other healthcare personnel to optimize health outcomes,it is much more difficult to define the best model. Each approach is highlydependent on context, with terminology used in one setting having a quitedifferent meaning in another one. Therefore, many organizational interven-tions, such as stroke units, are evaluated as “black boxes”, in which the inter-vention is defined by the name given to it, often with little understanding aboutthe critical factors for success or failure.
Chronic illness confronts patients with a spectrum of needs that requires
them to alter their behaviour and engage in activities that promote physical andpsychological well-being, to interact with healthcare providers and adhere totreatment regimens, to monitor their health status and make associated caredecisions, and to manage the impact of the illness on physical, psychologicaland social functioning (Clark 2003). Yet, increasing responsibility taken bypatients for self-management can create particular challenges for those withmultiple conditions, as they may experience aggravation of one condition bytreatment of another. For example, a patient with chronic respiratory diseasemay struggle to adhere to exercise programmes designed for their diabetes(Bayliss et al. 2003).
Patients vary in their preferences for care and the importance they place
on health outcomes. Thus, some will prioritize maintenance of functionalindependence over intense medical management while others will be willing totolerate the inconvenience and risk of adverse effects associated with complexmultiple medication regimens if this is linked to longer survival, even if at theexpense of quality of life (Tinetti et al. 2004). The ability of patients to developindividualized treatment plans is, therefore, of critical importance for effectivecare. The growth of the consumer society, coupled with the explosion in infor-mation available on the Internet, is creating more empowered patients, a phe-nomenon acting to increase the responsiveness with which health services are
Caring for people with chronic conditions: introduction
delivered. However, this may also compromise equitable access to care, as thedigital divide enables those who are most privileged to take greatest advantageof the new opportunities provided while those in most need are left behind(Stroetmann et al. 2002). The situation is exacerbated as populations change,with increased global migration creating groups who, despite the goal of uni-versal coverage, may fall between the cracks, especially if their migration hasbeen illegal (Healy and McKee 2004). Unfortunately, our understanding of thescale and nature of any impact of these changes on access to care remainslimited. The shifting balance of care
Taken together, these developments can be seen as evidence of a growing com-plexity of healthcare. They are influencing profoundly the way that healthcareis being delivered. These influences can be considered under several headings(Royston 1998).
First, the growing opportunities for early intervention, coupled with a greater
recognition in some countries of the benefits of reducing the burden of diseaseas a means of relieving pressure on health systems, is shifting the balancebetween treatment and prevention. In the United Kingdom, for example, a2002 Treasury study on future needs for healthcare constructed a variety ofscenarios differing largely in the extent to which the health of the populationimproves. The difference in costs in 2022 between the most optimistic andpessimistic scenarios was approximately £30 billion ( 50 billion), approximatelyhalf of the 2002 National Health Service (NHS) expenditure (Wanless 2002). Yetthe issue is not one of simply shifting resources from treatment to prevention;rather it is one of finding ways to integrate the two, with prevention strate-gies that take full advantage of developments in healthcare while reorientinghealthcare to embed prevention at all stages.
Second, there is a changing balance between hospitals and alternative care
settings (Hensher and Edwards 2002). Hospitals have the advantage of confi-ning the patient in one place, waiting for a series of investigations or a sequenceof treatments to be undertaken. The patient is seen when it is convenient for thehealthcare providers. Organizationally, this makes it easy to deliver complexpackages of care, but it also brings major disadvantages for the patient, whoseliberty is restricted. Even for those people requiring continuing care, hospitalsmay not be the most appropriate setting to receive it. Patients with advancedcancer may be better placed in a hospice; those with moderate disabilities maybe able to manage better in their own homes but with enhanced nursing orother support. Again, this introduces a degree of complexity, as the needs of thepatient are assessed and alternative modes of care provided.
Third, there is a changing balance in the degree of professional and patient
involvement in care. In a less-deferential society, patients are less willing toaccept instructions without explanations. At the same time, it is recognized thatmany chronic conditions where the course of the disease may be labile, suchas asthma or diabetes, require significant participation by informed patients(Wagner et al. 1996). This, in turn, calls for support from healthcare providers to
inform and enable patients to self-manage their illness and may also necessitatean ongoing collaborative process between patients and professionals to optimizelong-term outcome.
Fourth, as already noted, there is a changing balance between evidence and
intuition in the clinical encounter, with a growing quest for evidence to under-pin clinical practice, and for mechanisms to ensure that the evidence is actedupon, that performance is assessed and action taken to improve it. This balanceis, however, dynamic as initial enthusiasms for protocol-driven care confrontthe reality of individual patient characteristics, thus exposing the limits ofdeterminism (McKee and Clarke 1995).
Fifth, in the face of evidence of growing inequities in societies, there is the
shifting balance between services that simply respond to demand and those thatproactively seek need, even when it is not voiced as demand, in the knowledgethat those whose needs are greatest may be least able to access the care that theyneed.
Sixth, there is the growing potential of information technology. Patients
accustomed to booking holidays or shopping on the Internet are increasinglypuzzled by the continuing reliance on postal communication by health services. In theory, booking an appointment should be easy. Yet there is a crucial differ-ence. The Internet model of holiday booking, involving the booking of a set ofreturn tickets and a hotel, is analogous to a single episode of care, for examplean attendance for a routine medical examination. However, the traveller insearch of a tailor-made holiday, visiting a sequence of destinations suited to hisor her individual needs, and using a variety of travel modes (a model moreanalogous to a patient with a multiple chronic diseases), will require the servicesof travel agent. Given that most patient journeys more closely resemble thebespoke holiday market, it is unsurprising that healthcare information systemsoften struggle to deliver what they promise.
Finally, there is the challenge of developing a workforce to respond to the
changing healthcare environment. This is a vast area, drawing together many ofthe previous six issues but added to by the problem of how to provide trainingin the increasingly diverse settings for healthcare. Conceptual framework
To explore the challenges outlined above, the study will use a conceptual frame-work that draws, broadly, on the Chronic Care Model (CCM) developed byWagner and colleagues (1999). This model presents a structure for organizinghealthcare to improve outcomes among patients with chronic illness and will bedescribed in detail in Chapter 4. In brief, the model comprises four interactingsystem components considered key to providing good care for chronic illness:self-management support, delivery system design, decision support and clini-cal information systems. These are set in a health system context that linksan appropriately organized delivery system with complementary communityresources and policies.
Clearly, issues related to chronic illness that can be addressed under each of
these headings are potentially boundless and our aim is not to duplicate work
Caring for people with chronic conditions: introduction
that has already been undertaken, such as the increasing volume of reviewsof the effectiveness of the different components of the CCM that form partof many disease management and related care programmes (see for example(Renders et al. 2001; Bodenheimer et al. 2002; Weingarten et al. 2002; Ofmanet al. 2004; Ouwens et al. 2005; Tsai et al. 2005; Zwar et al. 2006). Instead, weuse the headings to examine in depth some of the key features related to thegrowing complexity of healthcare that have so far received less attention.
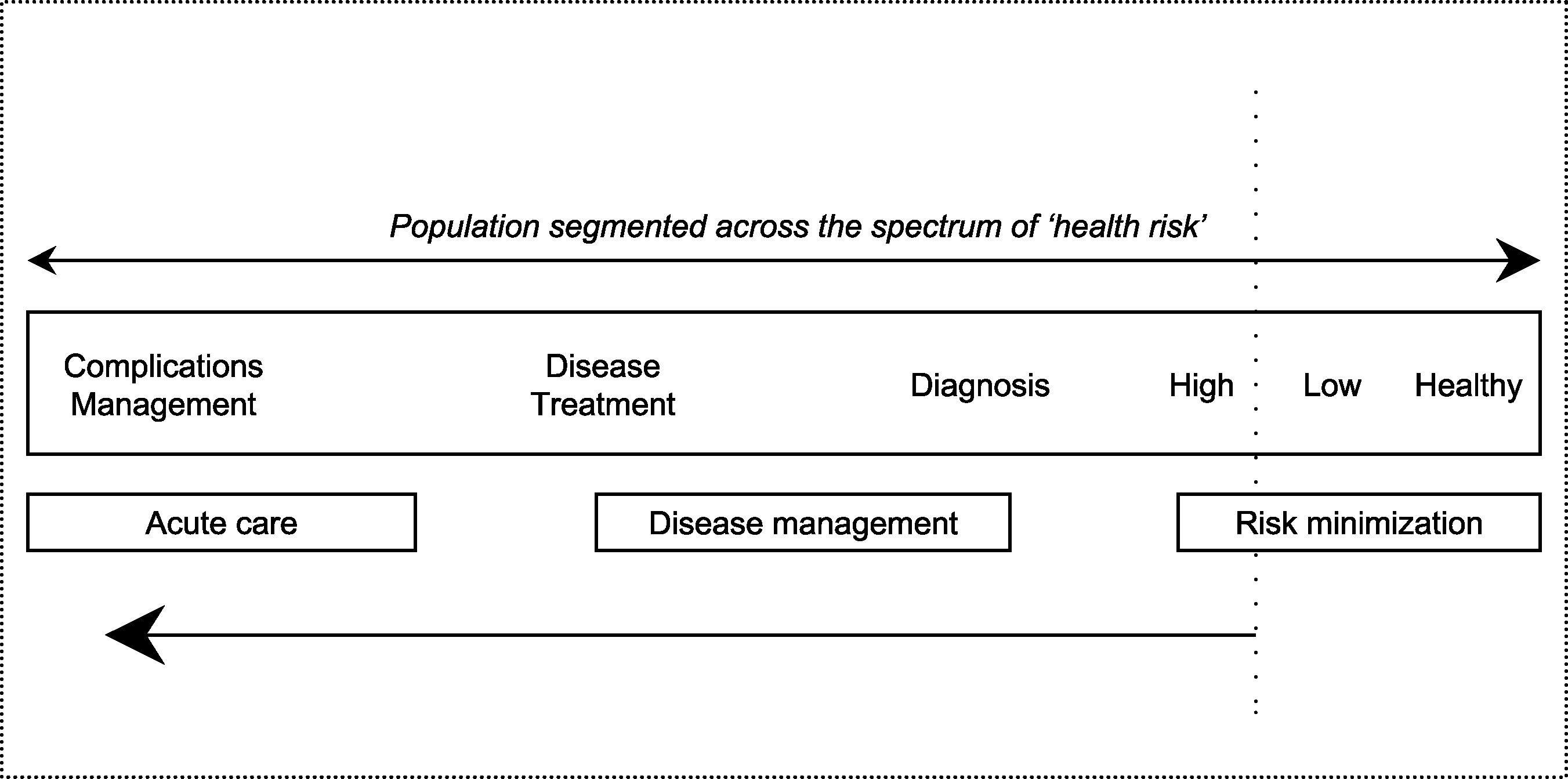
The focus of the study is on the health system/services arrangements for
people with established chronic health problems/diseases. Consequently, con-tributions to this book are based on chronic conditions/diseases, defined (usingthe WHO definition) as requiring ongoing management over a period of yearsor decades, and where there may be intercurrent acute episodes associated witha chronic condition or other acute illnesses. We consider all activities thatstretch from minimizing the probability that those with risk factors will developestablished chronic disease all the way through to the management of highlycomplex cases, as illustrated in Figure 1.1. The focus is on the healthcaresector, and social and/or community service models are only discussed wherethere is an integrative link with healthcare and/or they provide useful lessonslearnt.
The ensuing work has evolved from a process of analysis at two levels, similar
to previous Observatory studies, such as our recent work on Human Resources forHealth (Dubois et al. 2006; Rechel et al. 2006). On one level, a series of keythemes are examined, based on a synthesis of the theoretical and empiricalevidence from a wide range of mostly high-income countries. On a second level,detailed analyses have been undertaken in individual countries that examineapproaches to chronic illness care in different healthcare settings; these arepublished in a companion volume (Nolte et al. 2008). Figure 1.1
Health system activities covered in this book. Source: Adapted from Petersen and Kane 1997. Outline of the book
Given the breadth and complexity of the topic, it is important to say what thisbook is not. It is not a practical manual on how to implement a disease man-agement programme, first because there are many such guides elsewhere but,second, and more importantly, a key lesson from the analyses presented in thisbook is that the differing contexts in which people work require that solutionsbe tailored to national circumstances. Instead, we set out the evidence aboutwhat has been found to work, or not work, in different circumstances in thehope that this will be of use to those engaged in tackling the challenge of com-plex chronic disease. In contrast to some other volumes on often quite specificaspects of chronic disease, therefore, we have taken a broad perspective, settingthe context within which policies are being made, addressing the prerequisitesfor effective policies and examining how decisions made for other purposes,such as how to pay for healthcare, may impact on managing chronic disease.
The book is divided into three broad sections. The first sets out the epidemi-
ological evidence on the changing burden of chronic disease in the Europeanregion and explores the economic case for investing in chronic disease man-agement. The second section examines some of the key challenges posed by therising complexity of healthcare, including prevention, using headings adaptedfrom the CCM. The third section looks at the role of the broader health sys-tem, examining systems for financing chronic care and how the overall policyenvironment enables or hinders the introduction and implementation of effect-ive approaches to chronic care.
Looking in more detail, Chapter 2 examines the burden of chronic disease
facing the European region. It pays particular attention to morbidity patterns,drawing together epidemiological data on leading chronic conditions, suchas stroke, diabetes, chronic obstructive pulmonary disease and asthma, andselected mental disorders, such as depression. One key challenge the chapterhighlights is that of identifying reliable, appropriate and comparable datathat allow for a comprehensive assessment of the burden of disease across theEuropean region and that can inform local and national policies. It argues thatchanging demographic patterns and increasing evidence on the health andsocietal costs of chronic diseases make it crucial to overcome the methodologicalchallenges in assessing and monitoring the chronic disease burden.
Chronic diseases pose a sizeable burden for national economies, with some
studies estimating the associated costs at up to 7% of a country’s gross domesticproduct (Oxford Health Alliance Working Group 2005). This is partly a result ofdirect medical costs, from increased utilization of health services, medicationand potentially costly interventions (e.g. Jonsson 2002; Reynolds et al. 2004)but also reflects indirect costs, for example through decreased work productivity(Oxford Health Alliance Working Group 2005). Chapter 3 explores the eco-nomic and business case for tackling chronic disease, in order to provide theevidence base required for an informed debate weighing the costs associatedwith coordinated care programmes (Congressional Budget Office 2004) againstthe expected societal benefit. A key concern is an observed disconnect betweenthe economic and the business case, which is likely to result in the provision
Caring for people with chronic conditions: introduction
of what is, from a societal perspective, a suboptimal level of active chronicdisease management if not addressed by appropriate financing and deliverymechanisms.
Chapter 4 explores approaches to addressing the healthcare needs of those
with chronic health problems. It reviews different approaches to chronic care,which have variously been described as “integrated care”, coordinated care’,“managed care”, “disease management”, “case management”, “patient-centredcare”, “chronic (illness) care”, “continuity of care” and others. It then describesselected theoretical frameworks and existing delivery models designed to pro-vide care to those with varied levels of need. It goes on to examine the evidencebase, taking advantage of the accumulating evidence on the relative effective-ness of different models and component features of chronic care (Bodenheimeret al. 2002; Weingarten et al. 2002; Ouwens et al. 2005; Singh 2005a; Singh andHam 2006).
Although this book is mainly concerned with the management of chronic
disease, it is clear that an effective response includes preventing chronic diseasesfrom occurring in the first place. The leading risk factors are mostly known, andso are effective interventions to reduce exposure; yet the response to the chal-lenge remains inadequate in many countries (Yach et al. 2004). Chapter 5 pro-vides an overview of trends in the leading determinants of chronic diseases andprovides examples of effective prevention efforts in both the clinical and thepopulation-based context. It illustrates how prevention is truly “everyone’sbusiness”, with government, the private sector, the healthcare system and theindividual patient all having substantial responsibilities for applying evidence-based prevention to the growing burden of chronic diseases.
Chronic illness confronts patients with a spectrum of needs that requires
them to alter their behaviour and engage in activities that promote physical andpsychological well-being, to interact with healthcare providers and adhere totreatment regimens, to monitor their health status and make associated caredecisions, and to manage the impact of the illness on physical, psychologicaland social functioning (Clark 2003). Chapter 6 explores approaches to engageand/or empower patients towards self-management. It describes theoreticalapproaches that underpin many self-management support interventions andanalyses the nature and effectiveness of self-management support in chronicdisease, highlighting the challenges of providing such support to people withmultiple conditions or those disadvantaged because of their ethnic or socio-economic background. It identifies a clear need for more research to understandbetter the impact of support programmes on health outcomes and on the sus-tainability of improvements over the long term. It also shows that, while self-management support is recognized as an important element of chronic care, fewcountries seem to be developing or implementing systematic strategies to pro-mote this process. This underlines how important it will be for health policymakers, insurers and providers to create systems that enable all patients tomanage their conditions effectively as part of a coordinated strategy.
It has been suggested that the key to effectively controlling chronic disease is
the creation of systems that involve many different professionals and specialistsworking as teams to ensure that the right patients get the right type of care at theright time (Norris et al. 2003; Singh 2005b). Yet while the benefits for patients
may be obvious, it is less clear how restructuring of the delivery system impactson those who have to implement it, namely the healthcare workers. Chapter 7explores the crucial role of human resources in the provision of essential servicesto people with long-term conditions. It examines consequences of organiza-tional restructuring for the composition and deployment of the healthcareworkforce as well as the impact on job design and work practices (e.g. rolesubstitution, job expansion, job diversification, team work, skill mix). It illus-trates key levers that can motivate change and enable the successful andsustainable implementation of approaches to chronic care from a workforceperspective. These include conceptualizing a human resources continuum,where service users take a key role, redefining professional roles, developinggeneric competencies and reconfiguring the practice environment.
An important component of chronic disease management is decision support
that will help healthcare providers to ensure effective treatment (Wagner et al. 1996). Chapter 8 shows how decision support embraces a broad array of inter-ventions, increasingly reliant on electronic systems for their delivery, with thecommon purpose of increasing the quality of chronic disease care through thestandardization of the delivery of care in accordance with best evidence-basedpractice while containing costs. It focuses in particular on computerized clinicaldecision support systems, identifying evidence of gains in both quality andsafety of care associated with such systems. It notes the many challenges sys-tems are facing in implementing these systems, highlighting the implicationsfor, for example, funders of health services, who will have to balance the costsrelated to the use of new technologies and new activities against the ratheruncertain knowledge about whether these new expenditures will be offset bysavings elsewhere in the system.
The CCM recognizes that “improvement in the care of patients with chronic
illness will only occur if the system leaders . . . make it a priority and provide theleadership, incentives and resources necessary to make improvements happen”(Epping-Jordan et al. 2004). Chapter 9 sets out the different means by whichfunders can pay for healthcare, exploring the theoretical advantages and dis-advantages of each approach while recognizing the rather more limited evidencebase. It then considers the organizational facilitators and barriers to setting upthose payment systems that will be expected to achieve optimal results beforemoving on to look in detail at the lessons emerging from the few evaluationsthat have been conducted, primarily in the United Kingdom and the UnitedStates.
Chapter 10 concludes by exploring existing challenges to better coordination
and integration, seeking to identify ways of overcoming them. Examining thevarious approaches taken by different countries, it identifies three key elementsthat ought to be in place for an effective response to chronic disease: sustainedfinancing, skilled and motivated health professionals, and supportive informa-tion systems. However, it also finds that putting these elements in place willnot be sufficient in itself. The complexity of chronic diseases and the poten-tial responses to them mean that solutions will not emerge spontaneouslybut instead require a comprehensive, consistent and contextually appropriateframework that ensures that the necessary actions are taken to reconfigureorganizational structures, remove barriers to change, and invest in training and
Caring for people with chronic conditions: introduction
information technology. Success is not impossible, but the difficulties shouldnot be underestimated. The audience for this book
Few people will go through life unaffected by chronic disorders, whether assufferers, informal carers, health professionals and managers, or developing pol-icies in the health and other sectors. This book will, inevitably, be of mostinterest to the last two groups, but we hope that there will also be somethinguseful in it for the others. The nature of healthcare is changing, in many casesquite rapidly. Yet many health systems are still configured in ways that are moreappropriate for the demands of the mid twentieth century rather than the midtwenty-first. Effective responses will require initiatives at all levels to ensure thatthe right resources (skilled staff, technology, pharmaceuticals and knowledge)can be assembled in the right place at the right time, while establishing supportand incentives for everyone to work together to achieve this shared aim. Thereare no easy answers, and those working in different health systems must findmodels that are appropriate to their own circumstances. Yet there is also con-siderable scope for shared learning from each other’s successes (and failures). This book, and the companion volume of case studies, seek to contribute to thisprocess. References
Bayliss, E.A., Steiner, J.F., Fernald, D.H., Crane, L.A. and Main, D.S. (2003) Descriptions
of barriers to self-care by persons with comorbid chronic diseases, Ann Fam Med, 1:15–21.
Bodenheimer, T., Wagner, E.H. and Grumbach, K. (2002) Improving primary care for
patients with chronic illness: the chronic care model, Part 2, JAMA, 288: 1909–14.
Boyd, C., Darer, J., Boult, C. et al. (2005) Clinical practice guidelines and quality of care for
older patients with multiple comorbid diseases, JAMA, 294: 716–24.
Britton, A., McKee, M., Black, N. et al. (1999) Threats to applicability of randomised trials:
exclusions and selective participation, J Health Serv Res Policy, 4: 112–21.
Clark, N.M. (2003) Management of chronic disease by patients, Ann Rev Public Health, 24:
Coleman, M.P., Alexe, D., Albreht, T. and McKee, M. (2008) Responding to the Challenge ofCancer in EUROPE. Ljubljiana: Government of Slovenia and European Observatory onHealth Systems and Policies.
Congressional Budget Office (2004) An Analysis of the Literature on Disease ManagementPrograms. Washington, DC: US Congressional Budget Office.
Conrad, D.A. and Shortell, S.M. (1996) Integrated health systems: promise and perform-
ance, Front Health Serv Manage, 13: 3–40.
Deutsches Zentrum für Altersfragen (2005) Gesundheit und Gesundheitsversorgung. DerAlterssurvey: Aktuelles auf einen Blick, ausgewählte Ergebnisse. Bonn: Bundesministeri-ums für Familie, Senioren, Frauen und Jugend. http://www.dza.de/download/Gesundheit.pdf (accessed 12 December 2006).
Dubois, C.-A., McKee, M. and Nolte, E. (2006) Human resources for health in Europe:
future trends, opportunities, and challenges, in C.-A. Dubois, M. McKee and E. Nolte
(eds) Human Resources for Health in Europe. Buckingham/New York: Open UniversityPress/McGraw-Hill Education.
Epping-Jordan, J.E., Pruitt, S.D., Bengoa, R. and Wagner, E.H. (2004) Improving the quality
of health care for chronic conditions, Qual Saf Health Care, 13: 299–305.
Grumbach, K. (2003) Chronic illness, comorbidities, and the need for medical generalism,
Hajjar, E., Cafiero, A. and Hanlon, J. (2007) Polypharmacy in elderly patients, Am J Geriatr
Hampton, J.R. (2003) Guidelines: for the obedience of fools and the guidance of wise
Healy, J. and McKee, M. (2004) Accessing Health Care: Responding to Diversity. Oxford:
Hensher, M. and Edwards, N. (2002) The hospital and the external environment: experi-
ence in the United Kingdom, in M. McKee and J. Healy (eds) Hospitals in a ChangingEurope. Buckingham, UK: Open University Press.
Hoffman, C., Rice, D. and Sung, H. (1996) Persons with chronic conditions. Their preva-
lence and costs, JAMA, 276: 1473–9.
Jelley, D. (2006) Which patients with which needs are leading the patient-led NHS? BMJ,
Jonsson, B. (2002) Revealing the cost of type II diabetes in Europe, Diabetologia, 45:
Junius-Walker, U., Theile, G. and Hummers-Pradier, E. (2007) Prevalence and predictors of
polypharmacy among older primary care patients in Germany, Fam Pract, 24: 14–19.
McGlynn, E.A., Asch, S.M., Adams, J. et al. (2003) The quality of health care delivered to
adults in the United States, N Engl J Med, 348: 2635–45.
McKee, M. and Clarke, A. (1995) Guidelines, enthusiasms, uncertainty, and the limits to
purchasing, BMJ, 310: 101–4.
Nolte, E., Knai, C. and McKee, M. (eds) (2008) Managing Chronic Conditions: Experience inEight Countries. Copenhagen: European Observatory on Health Systems and Policies.
Norris, S.L., Glasgow, R.E. and Engelgau, M.M. (2003) Chronic disease management. A
definition and systematic approach to component interventions, Dis Manage HealthOutcomes 11: 477–88.
Ofman, J.J., Badamgarav, E., Henning, J.M. et al. (2004) Does disease management
improve clinical and economic outcomes in patients with chronic diseases? A sys-tematic review, Am J Med, 117: 182–92.
Ouwens, M., Wollersheim, H., Hermens, R., Hulscher, M. and Grol, R. (2005) Integrated
care programmes for chronically ill patients: a review of systematic reviews, Int J QualHealth Care, 17: 141–6.
Oxford Health Alliance Working Group (2005) Economic Consequences of Chronic Diseasesand the Economic Rationale for Public and Private Intervention. Oxford: Oxford HealthAlliance [draft report].
Petersen, K. and Kane, D. (1997) Beyond disease management: population-based health
management, in W. Todd and D. Nash (eds) Disease Management. A Systems Approachto Improving Patient Outcomes. Chicago, IL: American Hospital Publishing.
Rechel, B., Dubois, C.-A. and McKee, M. (2006) The Health Care Workforce in Europe: Learn-ing From Experience. Copenhagen: World Health Organization 2006, on behalf of theEuropean Observatory on Health Systems and Policies.
Renders, C.M., Valk, G.D., Griffin, S. et al. (2001) Interventions to improve the manage-
ment of diabetes mellitus in primary care, outpatient and community settings,Cochrane Database Syst Rev, 1: CD001481.
Reynolds, M.W., Frame, D., Scheye, R. et al. (2004) A systematic review of the economic
burden of chronic angina, Am J Manag Care, 10(Suppl): S347–57.
Caring for people with chronic conditions: introduction
Ritchie, C. (2007) Health care quality and multimorbidity, Med Care, 45: 477–9. Royston, G. (1998) Shifting the balance of healthcare into the 21st century, Eur J Oper Res,
Safford, M., Allison, J. and Kiefe, C. (2007) Patient complexity: more than comorbidity.
The vector model of complexity, J Gen Intern Med, 22(Suppl 3): 380–90.
Schoen, C., Osborn, R., Doty, M. et al. (2007) Toward higher-performance health sys-
tems: adult’s health care experiences in seven countries, 2007, Health Aff, 26:w717–34.
Seddon, M.E., Marshall, M.N., Campbell, S.M. and Roland, M.O. (2001) Systematic review
of studies of quality of clinical care in general practice in the UK, Australia and NewZealand, Qual Health Care, 10: 152–8.
Singh, D. (2005a) Transforming Chronic Care. Evidence about Improving Care for People withLong-term Conditions. Birmingham: University of Birmingham, Surrey and Sussex PCTAlliance.
Singh, D. (2005b) Which Staff Improve Care for People with Long-term Conditions? A RapidReview of the Literature. Birmingham: University of Birmingham and NHS Modernisa-tion Agency.
Singh, D. and Ham, C. (2006) Improving Care for People with Long-term Conditions. A reviewof UK and International Frameworks. Birmingham: University of Birmingham, NHSInstitute for Innovation and Improvement.
Stroetmann, V.N., Husing, T., Kubitschke, L. and Stroetmann, K.A. (2002) The attitudes,
expectations and needs of elderly people in relation to e-health applications: resultsfrom a European survey, J Telemed Telecare, 8(Suppl 2): 82–4.
Suhrcke, M., McKee, M., Sauto Arce, R., Tsolova, S. and Mortensen, J. (2005) The Contribu-tion of Health to the Economy in the European Union. Brussels: European Commission.
Tinetti, M., Bogardus, S. and Agostini, J. (2004) Potential pitfalls of disease-specific guide-
lines for patients with multiple conditions, N Engl J Med, 351: 2870–4.
TNS Opinion & Social (2007) Health in the European Union. Special Eurobarometer 272e.
Tsai, A.C., Morton, S.C., Mangione, C.M. and Keeler, E.B. (2005) A meta-analysis of
interventions to improve care for chronic illnesses, Am J Manag Care, 11: 478–88.
Unwin, N., Epping Jordan, J. and Bonita, R. (2004) Rethinking the terms non-communic-
able disease and chronic disease, J Epidemiol Community Health, 58: 801.
van den Akker, M., Buntinx, F., Metsemakers, J., Roos, S. and Knottnerus, J. (1998) Multi-
morbidity in general practice: prevalence, incidence, and determinants of co-occurringchronic and recurrent diseases, J Clin Epidemiol, 51: 367–75.
Wagner, E.H., Austin, B.T. and Von Korff, M. (1996) Organizing care for patients with
chronic illness, Milbank Q, 74: 511–44.
Wagner, E.H., Davis, C., Schaefer, J., Von Korff, M. and Austin, B. (1999) A survey of
leading chronic disease management programs: Are they consistent with the litera-ture? Manage Care Q, 7: 56–66.
Wanless, D. (2002) Securing our Future Health: Taking a Long-term View. London: HM
Weingarten, S.R., Henning, J.M., Badamgarav, E. et al. (2002) Interventions used in
disease management programmes for patients with chronic illness: which ones work?Meta-analysis of published reports, BMJ, 325: 925.
WHO (2003) Adherence to Long-Term Therapies. Evidence for Action. Geneva: World Health
WHO (2002) Innovative Care for Chronic Conditions: Building Blocks for Action. Geneva:
Wilson, T., Buck, D. and Ham, C. (2005) Rising to the challenge: will the NHS support
people with long-term conditions? BMJ, 330: 657–61.
Wolff, J., Starfield, B. and Anderson, G.F. (2002) Prevalence, expenditures, and complica-
tions of multiple chronic conditions in the elderly, Arch Intern Med, 162: 2269–76.
Yach, D., Hawkes, C., Gould, C.L. and Hofman, K.J. (2004) The global burden of chronic
diseases: overcoming impediments to prevention and control, JAMA, 291: 2616–22.
Zwar, N., Harris, M., Griffiths, R. et al. (2006) A Systematic Review of Chronic Disease Man-agement. Sydney: Australian Primary Health Care Institute.
Intrathecal Errors Daniel M. Lugassy, M.D. David H. Jang, M.D. Lewis S. Nelson, M.D. New York University Medical Toxicology Fellowship New York City Poison Control Center Case 1 Summary: Intrathecal chemotherapy A 16 year-old boy with a acute lymphoblastic leukemia (ALL) is receiving his seventh weekly prophylactic intrathecal chemotherapeutic treatment with methotrexate (MTX)
Substance Abuse Treatment Breaking News for the T reatment Field Acamprosate: A New Medication for Alcohol Use Disorders What is acamprosate? glutamate and gamma-aminobutyric acid (GABA) neurotransmitter systems. Although acamprosate’s Acamprosate (calcium acetyl homotaurinate) is a mechanism of action has not been clearly established, new prescription medication t
 Caring for people with chronic conditions: introduction
that has already been undertaken, such as the increasing volume of reviewsof the effectiveness of the different components of the CCM that form partof many disease management and related care programmes (see for example(Renders et al. 2001; Bodenheimer et al. 2002; Weingarten et al. 2002; Ofmanet al. 2004; Ouwens et al. 2005; Tsai et al. 2005; Zwar et al. 2006). Instead, weuse the headings to examine in depth some of the key features related to thegrowing complexity of healthcare that have so far received less attention.
Caring for people with chronic conditions: introduction
that has already been undertaken, such as the increasing volume of reviewsof the effectiveness of the different components of the CCM that form partof many disease management and related care programmes (see for example(Renders et al. 2001; Bodenheimer et al. 2002; Weingarten et al. 2002; Ofmanet al. 2004; Ouwens et al. 2005; Tsai et al. 2005; Zwar et al. 2006). Instead, weuse the headings to examine in depth some of the key features related to thegrowing complexity of healthcare that have so far received less attention.