Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients wellbutrin xl uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Vincristine case
Intrathecal Errors
Daniel M. Lugassy, M.D. David H. Jang, M.D. Lewis S. Nelson, M.D. New York University Medical Toxicology Fellowship New York City Poison Control Center Case 1 Summary: Intrathecal chemotherapy
A 16 year-old boy with a acute lymphoblastic leukemia (ALL) is receiving his seventh
weekly prophylactic intrathecal chemotherapeutic treatment with methotrexate (MTX) 15 mg, cytarabine 50 mg and hydrocortisone 50 mg. During the intrathecal injection, he complains of burning pain in both legs, prompting abrupt cessation of administration. The patient’s neurologic exam does not reveal any motor weakness or abnormal rectal tone. The symptoms subside within approximately twenty minutes. Shortly thereafter it is discovered that cytarabine and MTX were unintentionally dissolved in bacteriostatic water, which contains 0.9% of benzyl alcohol, instead of preservative-free water. Case 2 Summary: Intraventricular chemotherapy
A 52 year-old woman with central nervous system (CNS) lymphoma presents for her
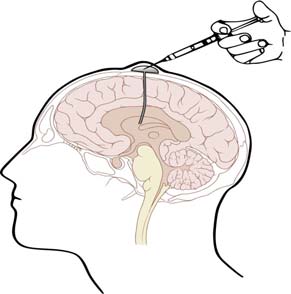
scheduled infusions of intravenous vincristine and intracerebroventricular methotrexate. The patient receives methotrexate through an Ommya reservoir (Figure 1), but the vincristine (2 mg), which was intended for intravenous administration, is also infused into the Ommya reservoir.
Figure 1: Ommya reservoir: This device consists of a small balloon (reservoir) underneath the scalp connected to tubing that traverses the skull into an intracranial location such as the ventricular space. The reservoir allows easy access to the cerebrospinal fluid for sampling or administration of an intracerebroventricular infusion of chemotherapeutics. (Image: Lynch, P.)
What is the benefit of intrathecal pharmacotherapy?
Intrathecal administration is defined as the injection or infusion of a xenobiotic into the
cerebrospinal fluid (CSF) at any level of the cerebrospinal axis, including into the cerebral ventricles (e.g., Ommya reservoir). Advantages of this route of administration include direct delivery to CNS, fewer side effects, and lower dose to attain appropriate CNS drug concentrations when compared to other routes. Administration of intrathecal medications
typically occurs though an indwelling lumbar catheter or spinal/epidural needle. Medication classes that are commonly administered intrathecally include antibiotics, chemotherapeutics, anesthetics, and analgesics.
While intrathecal medication administration is less commonly performed than
administration by most other routes and complications less frequent, those complications that occur can be catastrophic. A dosing error, improper compounding, and delivery of medications not intended for intrathecal administration (e.g., vincristine, benzyl alcohol) are causes of such errors. There are many factors that govern the safety and potential toxicity of intrathecal medications such as lipophilicity, ionic state, and osmolarity. What concerns should one have about benzyl alcohol (benzene methanol)?
Benzyl alcohol is a colorless liquid with a mild aromatic odor that is used as a solvent
due to its polarity and low vapor pressure. It is also commonly added to pharmaceuticals as a bacteriostatic. Benzyl alcohol is present in intravenous medications such as lorazepam, vecuronium, and diazepam in concentrations that range from 0.9% to 2%.
Benzyl alcohol is oxidized to benzoic acid and subsequently conjugated with glycine in
the liver to form hippuric acid, which is then renally eliminated. In the 1980’s, a “gasping” syndrome was described in low-birth weight infants who either received intravenous pharmaceuticals containing benzyl alcohol or flushes with bacteriostatic saline/water containing 0.9% benzyl alcohol. This syndrome consisted of bradycardia, hypotension, gasping respirations, acidosis, seizures, and death. Preterm infants lack the ability to properly conjugate benzoic acid (perhaps from glycine deficiency) resulting in the bioaccumulation of benzoic acid.
Intrathecal chemotherapeutics diluted in solutions containing benzyl alcohol preservative
are reported to cause transient paraplegia. Experimental animal evidence of benzyl alcohol applied to dorsal nerve roots suggests this acute effect is caused by nerve conduction blockade, akin to that occurring with a local anesthetic. Chronic exposure to benzyl alcohol results in patchy demyelination that may be irreversible, resulting in neuronal death. Treatment of patients with intrathecal benzyl alcohol injection is typically supportive but significant exposures may require aggressive CSF exchange and lavage as described below. Several case reports demonstrate neurotoxicity after intrathecal exposure to bacteriostatic preservative. Why should vincristine never be administered intrathecally?
Vincristine is derived from the Madagascar rosy periwinkle plant (Catharanthus roseus)
and was initially thought to have a role in the treatment of diabetes. Investigations failed to prove
any antidiabetic effects, but did reveal its ability to cause severe bone marrow suppression. Vincristine and other vinca alkaloids such as vinblastine bind tubulin, disrupting the formation and causing depolymerization of microtubules responsible for many critical cell functions. Microtubule dysfunction leads to cell division arrest in metaphase resulting in rapid cell death. Rapidly dividing cells, such as those that are cancerous, intestinal, epithelial, and hematopoetic in origin, are most affected. This accounts for the use of vincristine to treat lymphoma, leukemia, and certain solid tumors.
Vincristine used intravenously causes well recognized dose-limiting neurotoxicity, often
manifested as peripheral neuropathy. Findings include sensory deficits, ocular palsies, and bowel dysfunction. These effects are often reversible with drug discontinuation. Under normal circumstances CNS toxicity does not occur with intravenous administration because vincristine does not penetrate the blood brain barrier.
It is never appropriate to administer vincristine directly into the cerebrospinal
compartment by either intrathecal or intracerebroventricular route. The first case report of intrathecal administration of vincristine was published in 1968, and there have since been more than 55 cases reported worldwide. When inadvertently administered in this manner the fatality rate approaches 100%. There appears to be only 5 reported long term survivors, all of whom suffered significant permanent neurologic deficits. The effects may be seen within the first few hours after exposure, but are often delayed for 24-72 hours. Clinical toxicity after intrathecal injection generally follows a predictable course, manifesting as a progressive ascending myeloencephalopathy. Initially signs and symptoms include distal lower extremity weakness, parathesias, pain, and loss of tendon reflexes. Neurological deficits begin at the lumbosacral level of exposure and ascend superiorly spreading across other levels of the spinal cord and finally to the brain. The neurologic damage then rises to involve the trunk and upper extremities, with concurrent autonomic dysfunction of the bladder, bowel and other organs. Central nervous system effects usually follow including chemical meningitis, headache, altered mental status, central respiratory failure, and coma. At autopsy, CNS lesions of patients exposed to intrathecal vincristine show ascending chemical leptomeningitis and ventriculitis with underlying necrosis of the spinal cord, brain stem and cerebellum. What is the management of a patient with central nervous system exposure to vincristine?
The following are general guidelines for inadvertent intrathecal exposure, such as
following methotrexate overdose or unintended administration of vincristine. These guidelines cannot be truly evidence based given the infrequent and variable nature of such exposures. Individual cases may warrant varying levels of intervention, but following intrathecal or intracerebroventricular vincristine emergent measures should be taken to attenuate the exposure. The single most important intervention that may impact survival is the immediate aspiration of local CSF to retrieve as much drug as possible. Time is extremely critical as the amount recovered falls dramatically within the first few hours. In human cases reports of intrathecal methotrexate overdose 10 mL of CSF aspirate recovered 94% of the drug at 30 minutes after exposure, but only 10% was recovered at 180 minutes. Placing the patient in the upright position immediately if possible is also a common intervention after intrathecal administration errors, using gravity to delay the ascent of the drug to the brain. In the case reported here, vincristine was injected directly into the ventricle of the brain, so immediate cerebral exposure has already
occurred and it is unclear whether such positioning after intracerebroventricular exposure provides any benefit.
Subsequent to positioning and aspiration, aliquots of 20-75 mL in adults or 10-20 mL in
children of CSF should be removed sequentially. Each disposed amount of CSF should be replaced by sterile technique with equal amounts of normal saline or lactated Ringers. While CSF exchange is occurring, in critical exposures such as vincristine the patient can be prepared for CSF lavage. Commonly, a ventriculostomy or cervical spinal catheter and a lumbar drain are inserted, allowing fluid (e.g., normal saline) to be infused through the brain or upper spinal cord, respectively, and drained out of the lumbar region. In case 2 and other previous reports the Ommya reservoir allowed infusion of fluid so that only the placement of a lumbar drain was needed. The addition of fresh frozen plasma (FFP) to the isotonic fluid is recommended for its ability to bind vincristine. Generally 15-25 mL of FFP is added to one liter of lactated Ringers and the rate of lavage should approach a goal of 150 mL/hour (reasonable but based on little data). It is recommended that CSF lavage be performed for a minimum of 24 hours, but this is based on case reports and the understanding that most drugs, including vincristine, will no longer be present in the CSF after 24 hours. Are there other adjuncts or interventions that may be used specifically for intrathecal vincristine exposure?
There are four additional adjuncts that have been used in cases of intrathecal or
intracerebroventricular vincristine exposure (please see dosing of each below). Dexamethasone is given to prevent and treat meningeal inflammation. Glutamic acid, pyridoxine, and folinic acid are also used in cases of neuraxial exposure because of data suggesting their benefit treating the neurotoxicity of intravenous vincristine. Glutamic acid and vincristine share a common cellular transport mechanism; therefore glutamic acid may competitively inhibit vincristine entry into the cell. In addition glutamic acid appears to stabilize tubulin structure and promote microtubule formation. Human and animal data demonstrate that glutamic acid may prevent peripheral neuropathy from intravenous vincristine. In an animal model pyridoxine reduced neurotoxicity from vincristine, but in a human trial it failed to show a benefit. Folinic acid (leucovorin) has also been used to treat vincristine associated peripheral neuropathy and myelosuppression, because vincristine may also inhibit dihydrofolate reductase and thymidylate synthetase. An antibody to vinca alkaloids has shown limited benefit for intravenous vincristine overdose but there has been no evidence for its role following intrathecal exposure. Dosing recommendations of adjuncts used after intrathecal vincristine: 1. Dexamethasone 4 mg/m2 IV every 6 hours 2. Glutamic acid 10 g IV over 24 hours, or 500 mg PO three times a day 3. Pyridoxine 50 mg IV every 8 hours 4. Folinic acid 25 mg IV every 6 hours How can intrathecal errors be prevented?
Because errors in intrathecal administration of chemotherapeutics are potentially
devastating with significant morbidity and mortality a focus on prevention is of critical importance. Failures may occur in several steps along the process of ordering, preparation,
labeling, and administration. Intrathecal errors should never occur and are often due to poorly designed or absent safety checks. The Joint Commission issued a sentinel event alert in 2005 to provide guidance to all hospitals, chemotherapeutic infusion centers and other facilities where intrathecal injections or infusions are given. Human error theory (by Reason) recommends systems that support front line workers by both simplifying the practice and complicating error production. Practical procedures at all levels from pharmacy, transport, nursing and physicians need to be implemented to prevent such errors.
In case 1, an error occurred in the pharmacy where bacteriostatic water was inadvertently
used during an intrathecal preparation. In case 2, intrathecal vincristine administration occurred because both an intrathecal and intravenous drug were at the patient’s bedside concurrently and there were no specific policies or procedures in place for intrathecal administration.
The following are just a few recommendations that may help to prevent these intrathecal
errors. Establish dedicated locations for the preparation and administration of intrathecal medications (IT Zone) that restricts any other activities from being performed. The IT zone in pharmacy is used only for intrathecal medication preparation, where agents not intended for intrathecal use are strictly prohibited. Label the syringe for intrathecal use only. Transport should be by a dedicated messenger or the administering/verifying clinician delivering the agent directly to the administration IT zone at the scheduled time of administration. The IT zone is only for the intrathecal agent and no intravenous medications should be permitted in the space. Some facilities have policies that patients who are on a regimen of intrathecal and intravenous chemotherapy receive medications via these two different routes on two separate days solely to prevent such errors. In pediatric cases where sedation or general anesthesia is administered the IT zone (e.g. dedicated Mayo stand) should ideally be outside of the reach of the anesthesiologist to prevent inadvertent placement of another drug in the zone. A “time out” procedure, using a dual person check that includes the administering clinician should occur, including a specific confirmation that the intrathecal label on the syringe is visible. It has also been suggested that vincristine only be prepared as a small volume infusion rather than in a syringe to prevent confusion as most intrathecal agents are given by syringe only. Ideally, the labels and connectors for the tubing and catheters involved in the various routes of administration will adequately warn or frankly prevent delivery of a medication by an incorrect route. Such a technological solution is not currently available. Case 1 Resolution: Benzyl Alcohol Case
The patient was placed in an upright position and interventional radiology was consulted for possible placement of a lumbar drain. He was admitted for observation, no lumbar drain was placed, and he did not develop any further neurologic sequelae. Case 2 Resolution: Vincristine Case
Approximately 15 minutes after the injection of vincristine into the Ommya reservoir the error was realized and 30 mL of CSF was aspirated from the reservoir. The patient was transferred to the neurosurgical ICU for CSF exchange and ventriculolumbar lavage. FFP was added to the perfusate and dexamethasone, glutamic acid, pyridoxine and folinic acid were administered intravenously at the recommended doses discussed earlier. The patient had no complaints or neurological deficits until day 3, when she began to have subtle hearing loss, headache and mild
left lower extremity weakness. Her symptoms progressed rapidly with ascending paralysis, autonomic dysfunction, respiratory failure, and coma, and she expired on day 12. Conclusion
The limited utility of rescue measures after the incorrect administration of agent
intrathecally underscores the need for absolute adherence to safety requirements. While the majority of reported errors involve chemotherapeutic agents the potential for a misadministration event exists with any intrathecal agent. Should a misadministration occur, critical actions in the management of intrathecal errors include prompt recognition, maintaining access to the lumbosacral space with immediate withdrawal of CSF followed by isotonic fluid replacement. Unless the toxicity of the agent is known, all intrathecal errors should be assumed to be potentially fatal with emphasis on aggressive and timely treatment. References
1. Jones T, Feler C, Simmons B, et al. Neurologic complications including paralysis after a medication error
involving implanted intrathecal catheters. Am J Med 2002;112:31-36
2. Hahn AF, Feasby TE, Gilbert JJ. Paraparesis following intrathecal chemotherapy. Neurology
3. Al Ferayan A, Russell NA, Al Wohaibi M, et al. Cerebrospinal fluid lavage in the treatment of inadvertent
intrathecal vincristine injection. Childs Nerv Syst 1999;15:87-89
4. Jackson DV, Pope EK, McMahan RA, et al. Clinical trial of pyridoxine to reduce vincristine neurotoxicity.
5. Lagman JL, Tigue CC, Trifilio SM, et al. Inadvertent intrathecal administration of vincristine. Community
6. Qweider M, Gilsbach J, Rohde V. Inadvertent intrathecal vincristine administration: a neurosurgical
emergency. Case report. J Neurosurg Spine 2007;6:280-283
7. Michelagnoli MP, Bailey CC, Wilson I, et al. Potential salvage therapy for inadvertent intrathecal
administration of vincristine. Br J Haematol 1997;99:364-367
8. Gilbar P, Carrington C. Preventing intrathecal administration of vincristine. Med J Aust 2004;181:464-464 9. Ozyurek H, Turker H, Akbalik M, et al. Pyridoxine and pyridostigmine treatment in vincristine-induced
neuropathy. Pediatr Hematol Oncol 2007;24:447-452
10. Gutowski MC, Fix DV, Corvalan JR, et al. Reduction of toxicity of a vinca alkaloid by an anti-vinca
alkaloid antibody. Cancer Invest 1995;13:370-374
11. Wang, RY. Antineoplastic. In Goldfrank's Toxicologic Emergencies, 8th edition Flomenbaum NE, Lewin
NA, Howland MA, Hoffman RS, Nelson LS., Editors. 2006, McGraw-Hill: New York. p. 805-825.
12. Nordt SP, Vivero LE. Pharmaceutical Additives. In Goldfrank's Toxicologic Emergencies, 8th edition.
Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS., Editors. 2006, McGraw-Hill: New York. p. 829-842.
13. Rao RB. Special Considerations: Intrathecal Administration. In Goldfrank's Toxicologic Emergencies, 9th
edition. Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS., Editors. 2009, McGraw-Hill: New York.
14. Joint Commission Sentinel Event Alert Issue 34 – July 14, 2005; Preventing vincristine administration
errors (Joint Commission website). Available at Accessed on December 17, 2009.
15. Reason, J. Managing the risks of organizational accidents. Brookfield, Vermont: Ashgate Publishing Co.
Dr. D. Siri, FAAAAI, FACAAI Dr. R. Govindaiah Dr. E. Pratt Allergy Skin Test Info rmation and Instructions What is skin testing? If you suspect that a particular allergen (for Skin testing is a rapid way to detect if you are allergic to an inhalant or food. It is more sensitive provoking your symptoms, please inform the and economical than allergy blood tests. Specifically, i
 Intrathecal Errors
Intrathecal Errors 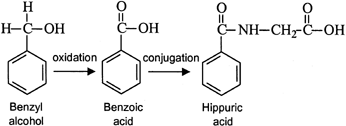 typically occurs though an indwelling lumbar catheter or spinal/epidural needle. Medication classes that are commonly administered intrathecally include antibiotics, chemotherapeutics, anesthetics, and analgesics.
While intrathecal medication administration is less commonly performed than
administration by most other routes and complications less frequent, those complications that
typically occurs though an indwelling lumbar catheter or spinal/epidural needle. Medication classes that are commonly administered intrathecally include antibiotics, chemotherapeutics, anesthetics, and analgesics.
While intrathecal medication administration is less commonly performed than
administration by most other routes and complications less frequent, those complications that