Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Ehi705 1153.1158
European Heart Journal (2006) 27, 1153–1158
Long-term compliance with beta-blockers,angiotensin-converting enzyme inhibitors,and statins after acute myocardial infarction
Gunnar H. Gislason1,2*, Jeppe N. Rasmussen2, Steen Z. Abildstrøm2,3, Niels Gadsbøll4,Pernille Buch1,2, Jens Friberg1, Søren Rasmussen2, Lars Køber5, Steen Stender6, Mette Madsen2,and Christian Torp-Pedersen1
1 Department of Cardiovascular Medicine, Bispebjerg University Hospital, Bispebjerg Bakke 23, DK-2400 Copenhagen NV,Denmark; 2 National Institute of Public Health, Copenhagen, Denmark; 3 Department of Cardiology, Gentofte UniversityHospital, Hellerup, Denmark; 4 Department of Internal Medicine, Roskilde County Hospital, Roskilde, Denmark; 5 Departmentof Cardiology, The Heart Centre, Rigshospitalet—National University Hospital, Copenhagen, Denmark; and6 Clinical Biochemistry, Gentofte University Hospital, Hellerup, Denmark
Received 10 October 2005; revised 5 December 2005; accepted 8 December 2005; online publish-ahead-of-print 6 January 2006
Aims To study initiation, dosages, and compliance with beta-blockers, angiotensin-converting enzyme
(ACE)-inhibitors, and statins in patients after acute myocardial infarction (AMI) and to identify likely
Methods and results Patients admitted with first AMI between 1995 and 2002 were identified by linking
nationwide administrative registers. A total of 55 315 patients survived 30 days after discharge and were
included; 58.3% received beta-blockers, 29.1% ACE-inhibitors, and 33.5% statins. After 1, 3, and 5 years,
78, 64, and 58% of survivors who had started therapy were still receiving beta-blockers, 86, 78, and 74%were receiving ACE-inhibitors, and 85, 80, and 82% were receiving statins, respectively. Increased ageand female sex were associated with improved compliance. The dosages prescribed were generally 50%or less of the dosages used in clinical trials, and dosages did not increase during the observation period. Patients who did not start treatment shortly after discharge had a low probability of starting treatmentlater. Conclusion The main problem with underuse of recommended treatment after AMI is that treatment isnot initiated at an appropriate dosage shortly after AMI. A focused effort in the immediate post-infarctionperiod would appear to provide long-term benefit.
treatment, drug dosages, and long-term compliance withbeta-blockers, ACE-inhibitors, and statins in 71 515 patients
after their first AMI between 1995 and 2002.
inhibitors, and statins are recommended for most patientsfollowing an acute myocardial infarction (AMI), but underuseis widely documented.1,2 Underuse may involve not starting
therapy, poor compliance, and underdosing. Much attention
The National Hospital Registry keeps records on all hospital admis-
has focused on the fact that many patients are never
sions in Denmark since 1978, and each hospitalization is classified
offered treatment,2 but compliance with treatment and
according to the International Classification of Diseases (ICD),
dosing has received less attention. Comprehensive analyses
until 1994 the ICD-8 and from 1994 the ICD-10. All patients are regis-
of initiation, compliance, and dosing are necessary to learn
tered via a unique and permanent civil registration number. The
the likely targets for improving long-term use. Since 1995,
Danish Registry of Medicinal Product Statistics includes information
the Danish Registry of Medicinal Product Statistics has regis-
about all prescription medicines dispensed from pharmacies in
tered all prescriptions dispensed from pharmacies in
Denmark since 1995. All prescriptions are registered at an individuallevel by using the civil registration number. The Registry classifies
Denmark according to each patient’s unique civil registration
medicines according to the Anatomical Therapeutic Chemical
number. In this study, we linked data from this Registry with
(ATC) system, an international classification system of pharmaceuti-
data from the National Hospital Registry to study initiation of
cals. As all residents in Denmark are covered by a national healthsecurity system and get the cost of drugs partly reimbursed, allpharmacies are required by law to register all prescription
* Corresponding author. Tel: þ45 3531 3328; fax: þ45 3975 1803.
dispensed in this nationwide registry. & The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected]
All patients aged 30 or older admitted with a diagnosis of first AMI
For descriptive statistics, the results are given as mean values with
(ICD-10: I21–I22) between 1995 and 2002 and alive 30 days after
standard deviation or as median values with range. To analyse
discharge (180 days for statins) were identified from the National
differences in proportion in drug use and death rates between
Hospital Registry. The diagnosis of AMI in the National Hospital
1995 and 2002, we tested for linear trend in logistic regression
Registry has been validated and has a sensitivity of 91% and predic-
models. The rates of first dispensing of treatment and break in
tive value of 93%.3 The selection procedure and characteristics of
treatment were estimated by the Kaplan–Meier method. To
the patients have been detailed previously.4,5 We registered
analyse the effect of available covariates (age, gender, year of
whether patients had a prescription of beta-blockers (ATC code
AMI, and concomitant medical treatment) on long-term compliance,
C07) and ACE-inhibitors (ATC code C09—also including angiotensin
we used Cox multivariable proportional hazard models and censor-
2 receptor blockers) dispensed 0–30 days from discharge after
ing for death. Model assumptions—the linearity of continuous
first AMI and statins (ATC code C10AA) dispensed 0–180 days from
variables, the proportional hazard assumption, and lack of
discharge. The reason the interval for statins differed was that
interaction—were tested and found valid unless otherwise indi-
the reimbursement policies for statins changed during the period.
cated. Furthermore, we calculated the persistence of therapy,
In 1995, reimbursement required individual application, but after
defined as number of patients having medicine available at any
1998, all AMI patients were reimbursed for the full cost of statins
time (having filled at least one prescription early after the AMI)
without need for individual application.
divided by the number of patients alive within particular treatment
All subsequent prescriptions were identified until the end of year
group. Patients with missing information or lost to follow-up (emi-
2002 or the date of death. Among patients who did not receive
grated), n ¼ 22 (0.04%), were censored at the time of disappear-
treatment early after discharge, we identified those who started
ance. All statistical calculations were performed using the SAS
treatment between 30 days and 1 year to estimate whether a
statistical software package, version 8.2 for UNIX servers (SAS
significant proportion initiated treatment later. As the registries do
not include information of left ventricular function and that theICD-10 cod for heart failure has a relatively low sensitivity, the
dispensed prescription of loop diuretics (ATC code C03C) 90 daysbefore to 30 days after discharge was used as a proxy for the
The Danish Data Protection Agency approved this study, and data
diagnosis of heart failure. In the same way, dispensed prescription
were made available to us such that individuals could not be
of antidiabetics (ATC code A10) 90 days before to 30 days after
discharge was used as a proxy for the diagnosis of diabetesmellitus.
During the 8-year study period, 71 515 patients had a firstadmission for AMI. The 30-day mortality was 22.7%,
The Danish Registry of Medicinal Product Statistics includes
ranging from 26.0% in 1995 to 17.4% in 2002 (P , 0.001).
information about the dispensing date of the prescription, the
A total of 55 315 patients were alive 30 days after discharge
strength of the drug, and the total number of tablets dispensed
and were included in the analysis of the use of beta-blockers
but not the prescribed dose of the drug. The dose of each prescrip-
and ACE-inhibitors after AMI. The 48 412 patients who were
tion was therefore calculated from the average dose given during
alive 180 days after discharge were included in the analysis
up to three consecutive prescriptions. Excess tablets wereallowed to be accumulated for up to three previous consecutive
of statins. The baseline characteristics of the study popu-
prescriptions at any time. On the basis of these assumptions,
we calculated whether patients at any time had tablets available
Figure 1 illustrates the timing of the first dispensing of
or not. We defined a patient as receiving treatment if tablets
each of the three drugs during the first year after AMI (cen-
sored for death). The probability of starting treatment was
To determine long-term compliance, we calculated whether
low if treatment was not started early for beta-blockers
patients who did not receive treatment were in a break of 7, 30,
and ACE-inhibitors. Only 5621 (10.7%) patients started
90, and 180 days or longer. We calculated the proportion of patients
beta-blocker treatment and 6694 (12.1%) ACE-inhibitors
who restarted therapy after a break of a particular length and found
between 31 days and 1 year after AMI. For statins, the
that a substantial proportion of patients restarted treatment again
start of treatment was slower, but between day 181 and 1
after a break shorter than 90 days. We therefore used a break of atleast 90 days as a proxy for poor compliance.
year, only 2868 (5.9%) patients started therapy. From 1995
To validate the calculations, sensitivity analysis was performed
to 2002, the number of patients initiating beta-blocker
with the average daily dose calculated also from single prescrip-
treatment later than 30 days after the infarction declined
tions, with the minimal dose equal to a previously calculated dose
from 11.5 to 9.3% (P , 0.001) and statins after 180 days
for the same patient and allowing each patient to keep residual
declined from 6.7 to 1.7% (P , 0.001), but the number of
tablets from one to five prescriptions. The manipulations resulted
patients receiving ACE-inhibitors after 30 days increased
in 75–85% agreement between the calculated doses and 2–4% with
from 10.5 to 12.0% (P , 0.001). Hospital-based physicians
changes in the number of patients stopping therapy.
issued the majority of the initial early prescriptions ofbeta-blockers, ACE-inhibitors, and statins (Table 2). The
evenly between hospital-based physicians and general
We calculated the average dosages of the most frequently used
medications within each group by multiplying the strength of the
Figure 2 illustrates the long-term compliance for patients
formulation by the number of tablets per day. The averagedosage was calculated only for patients who had medication avail-
who filled a prescription for a beta-blocker or ACE-inhibitor
able for treatment. To estimate underdosing, we compared the
within 30 days of AMI or a statin within 6 months. Short
average dosage with the dosages used in major randomized clinical
breaks in therapy were common, but many patients
restarted therapy later (Table 3). We used a break of at
Long-term compliance with beta-blockers, ACE-inhibitors, and statins
least 90 days to analyse factors of importance for poor
Baseline characteristics of the study sample
The Cox multivariable proportional hazard analysis
(Table 4) revealed that although there were increasing
number of patients initiating treatment from 1995 to
2002, this did not affect compliance. On the contrary, com-
pliance improved with beta-blockers. Women had better
compliance with beta-blockers and statins than men, and
older patients had better compliance with beta-blockers
but worse compliance with ACE-inhibitors and statins.
Concomitant medical treatment did not worsen compliance,
except for patients taking loop diuretics had slightly poorer
Table 5 shows the average dosages of the most frequently
used beta-blockers, ACE-inhibitors, and statins. We analysed
whether dosages changed during the observation time by
comparing the average dosages used during the first year
of treatment with the average dosages used between 3
and 5 years of treatment. This revealed that the average
dosages of beta-blockers and ACE-inhibitors changed only
between 2 and 7%. The average dosages of simvastatin and
pravastatin changed ,3%, but the dosages for atorvastatin
increased 21.5% from the first year when compared with3–5 years of therapy.
SD, standard deviation. aRanging from 38.1% in 1995 to 67.9% in 2002 (P , 0.001). bRanging from 24.5% in 1995 to 35.5% in 2002 (P , 0.001). cRanging from 11.7% in 1995 to 63.0% in 2002 (P , 0.001).
This study has four main findings. (i) If prophylactic treat-ment after a myocardial infarction is not initiated at thetime of discharge, the likelihood of ever receiving treatmentis small. (ii) If treatment is started early post-AMI, mostpatients adhere to treatment
Initiation of treatment nearly always relies on the initiativeof the hospital physicians. (iv) The prescribed doses ofall three drugs were substantially lower than thoserecommended and seldom adjusted during long-termtherapy.
All three drugs were prescribed with increasing frequencyduring the study period, the increase being most pro-nounced for beta-blockers and statins. Beta-blockers andACE-inhibitors were primarily initiated during the first 30days after AMI, whereas statin therapy was more graduallyinitiated during the first 6 months (Figure 1). This was prob-ably related to Denmark’s reimbursement policies, whichchanged in 1998, and AMI patients no longer need to apply
Cumulative frequency of patients with first AMI who filled a first
individually for reimbursement of the cost of statin
prescription of beta-blocker, ACE-inhibitor, or statin within 1 year afterdischarge (censored for death).
therapy. Notably, the vast majority of early prescriptions
First prescription claim of beta-blockers, ACE-inhibitors, and statins dispensed 0–30 days and 31–365 days from discharge, accord-
ing to the type of the physician issuing the prescription
were written by hospital-based physicians, whereas general
practitioners initiated very few early prescriptions (Table 2).
After 5 years of treatment, 58% of patients were still receiv-
The relatively few patients who started late had a more
ing beta-blockers, 74% ACE-inhibitors, and 82% statins
even contribution by hospital-based physicians and general
(Figure 2). The literature is sparse regarding studies on
practitioners, but the general practitioners still only
long-term compliance with treatment post-AMI. Registries
accounted for about half the initial prescriptions. Further,
that included selected departments have shown 6-month
the number of patients initiating treatment later than 30
compliance with ACE-inhibitors and beta-blockers exceed-
days for beta-blockers and 180 days for statins from 1995
ing 80%.2,6 Studies from North America among patients
to 2002 declined substantially. This emphasizes the import-
older than 65 years of age and patients participating in
ance of initiating treatment early, as the probability of
specific insurance systems showed that 60–80% continued
treatment after 1 year.7 The most comprehensive long-
It is interesting that although treatment was mostly
initiated by hospital-based physicians, there still remains
therapy. The long-term compliance in these studies was
substantial proportion of patients who do not start treat-
50–85% after 1 year, 40–77% after 2–3 years, and 45–50%
ment. Hospital-based physicians taking care of patients
with AMI are most often specialists in internal medicine or
The difficulty in comparing these numbers with those in
cardiology, and thus should be updated in appropriate treat-
our study is that compliance has been defined in many
ment of AMI patients. Most likely, some discharging physi-
different ways. Previous studies have not distinguished
cians rely on the fact that the doctor taking care of the
between breaks and discontinuation. Most of our patients
AMI patient after discharge initiates appropriate therapy
restarted therapy after a break, especially after a brief
not already started in the hospital, whereas doctors taking
break (Table 3). Even after a break of at least 90 days,
care of the patient after discharge depend on the judge-
almost half of the patients restarted therapy with beta-
ment of the discharging physician. To prevent such misun-
blockers and ACE-inhibitors within 1 year and almost 70%
derstanding, the discharging physician should initiate
treatment in the hospital and if not started at discharge
To analyse the factors influencing long-term compliance,
give clear message to the doctor taking care of the AMI
we used the time to first break of 90 days, or longer, in
multivariable proportional hazard analysis (Table 4). The
increase in early initiation of treatment during the studyperiod was not associated with decreased long-termcompliance—instead, compliance improved moderately butstatistically significantly. Notably, multiple drug therapydid not reduce compliance, and increased age and femalesex were also associated with improved compliance. Theseresults emphasize that an increased effort during the studyperiod to initiate more medicines in more patients was notassociated with worse compliance.
Analysis of the dosages of the most frequently used drugswithin each class revealed substantial underdosing ofalmost all medicines, with dosages generally 50% or lessthan the dosages that randomized trials have proved to beeffective (Table 5).15–19 We also analysed whether dosageschanged from the first prescription dispensed whencompared with later on but found that patients largelystayed at their initial dosage. Defining a target dose forstatins is more difficult because this may be related to the
Persistence with therapy in patients who claimed at least one
prescription early after AMI. Each point represents number of patients with
effect on serum cholesterol levels. Our data do not cover
available medication divided by the number of patients alive at that time.
patients’ cholesterol levels, and thus we cannot conclude
The proportion of AMI patients on beta-blocker, ACE-inhibitor, or statin therapy who experienced a break of at least 7, 30, 90, or
180 days within 5 years of treatment and the proportion who had re-initiated therapy within 1 year
Proportion re-initiating treatment within 1 year
Long-term compliance with beta-blockers, ACE-inhibitors, and statins
Cox multivariable proportional hazard analysis of covariates predicting first break in therapy of more than 90 days (a proxy for low
compliance) with beta-blockers, ACE-inhibitors, and statins in patients with first AMI, 1995–2002
RR, relative risk; CI, confidence interval. a1995–96 as reference. bWomen as reference. cAged 30–59 as reference. dNon-users as reference.
Average daily dosage of the most frequently used
beta-blockers, ACE-inhibitors, and statins after AMI
The AMI diagnosis in the National Hospital Registry has beenvalidated and is sensitive as well as specific.3 The registry
includes all hospital admissions in Denmark from 1978 and
therefore not affected by selection bias by only includingselected hospitals, certain health insurance systems, or
age groups. A comprehensive accumulation of nationwide
admission data and linking to other registries is unique for
Denmark. Although the study is based on registries from a
single country, Denmark’s health insurance system, which
partly reimburses all patients for drug expenses, is typical
A break in therapy of at least 90 days was arbitrarily
selected to define long-term compliance, as one-third to
half of the population experienced break of at least 90
days. Analyses of the effects of shorter or longer breaks in
therapy did not change the results noticeably.
The diagnostic criteria for AMI changed in 1999, and
during the study period more sensitive diagnostic markers
have been introduced (i.e. troponins). Nevertheless, this
has not resulted in dramatic change in the prognosis of
AMI 24 and it is unlikely that this affects our study.
aThe most frequently used medications within each class.
bProportion of all medications used within each class. c
information about basal clinical variables such as location
Dosages used in randomized clinical trials with clinical endpoint
or size of infarction, smoking status, systolic function, and
co-morbidity. However, the indication for treatment withbeta-blocker or statin after AMI is independent of these
about the dosages of statins. Although not as prominent as
factors. Further, ACE-inhibitors are primarily indicated for
for beta-blockers and ACE-inhibitors, the dosages of statins
patients with reduced systolic function and diabetes. We
were generally lower than those used in randomized
therefore used the concomitant use of loop diuretics and
antidiabetics as a proxy for, respectively, heart failure
and diabetes, to define subgroups of patients where there
enzyme inhibitors after myocardial infarction in Denmark, 1995–2002.
was definite indication for treatment. The registries do not
5. Rasmussen J, Gislason G, Abildstrom S, Rasmussen S, Gustafsson I, Buch P,
include information about contraindications to treatment,
Friberg J, Køber L, Torp-Pedersen C, Madsen M, Stender S. Statin use
adverse reactions, or allergies that might have caused the
after acute myocardial infarction: a Danish nationwide study. Br J Clin
treatment not to start or to be terminated early after
start. Also, we do not know how many patients started
6. Eagle KA, Kline-Rogers E, Goodman SG, Gurfinkel EP, Avezum A, Flather MD,
treatment in hospital and did not continue treatment after
Granger CB, Erickson S, White K, Steg PG. Adherence to evidence-basedtherapies after discharge for acute coronary syndromes: an ongoing
discharge. Furthermore, factors such as race/ethnicity,
prospective, observational study. Am J Med 2004;117:73–81.
history of depression or other psychiatric illness, and the
7. Simpson E, Beck C, Richard H, Eisenberg MJ, Pilote L. Drug prescriptions
specialty of the physician taking care of patient could also
after acute myocardial infarction: dosage, compliance, and persistence.
8. Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in
elderly patients with and without acute coronary syndromes. JAMA
9. Muhlestein JB, Horne BD, Bair TL, Li Q, Madsen TE, Pearson RR, Anderson JL.
This study demonstrates that long-term compliance can be
Usefulness of in-hospital prescription of statin agents after angiographic
expected if treatment with beta-blockers, ACE-inhibitors,
diagnosis of coronary artery disease in improving continued compliance
and statins is started early after AMI, although dosages are
and reduced mortality. Am J Cardiol 2001;87:257–261.
seldom uptitrated during long-term therapy. In contrast, if
10. Larsen J, Andersen M, Kragstrup J, Gram LF. High persistence of statin use
in a Danish population: compliance study 1993–1998. Br J Clin Pharmacol
therapy is not started in the early phase after AMI, the
patient is unlikely to ever receive appropriate medical
11. Andrade SE, Walker AM, Gottlieb LK, Hollenberg NK, Testa MA,
treatment. Most general practitioners and other physicians
Saperia GM, Platt R. Discontinuation of antihyperlipidemic drugs—do
treating survivors of AMI seem to rely on the initiative and
rates reported in clinical trials reflect rates in primary care settings?
judgement of the hospital department from which the
12. Avorn J, Monette J, Lacour A, Bohn RL, Monane M, Mogun H, LeLorier J.
patient is discharged. This underscores the importance of
Persistence of use of lipid-lowering medications: a cross-national study.
therapy in survivors of AMI. A more focused effort from
13. Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J.
hospitals treating AMI patients in starting these patients
Long-term persistence in use of statin therapy in elderly patients. JAMA 2002;288:455–461.
on relevant medicines and titrating them to an effective
14. Kopjar B, Sales AE, Pineros SL, Sun H, Li YF, Hedeen AN. Adherence with
dose will result in long-term benefits.
statin therapy in secondary prevention of coronary heart disease in veter-ans administration male population. Am J Cardiol 2003;92:1106–1108.
15. Reiter MJ. Cardiovascular drug class specificity: beta-blockers. Prog
16. Kober L, Torp-Pedersen C, Carlsen JE, Bagger H, Eliasen P, Lyngborg K,
The study was supported by an unrestricted research grant from the
Videbaek J, Cole DS, Auclert L, Pauly NC. A clinical trial of the angiotensin-
Danish Pharmaceutical Association (Grant no. 31-03) and the Danish
converting-enzyme inhibitor trandolapril in patients with left ventricular
Heart Foundation (Grant no. 05-04-B46-A522-22207).
dysfunction after myocardial infarction. Trandolapril Cardiac Evaluation(TRACE) Study Group. N Engl J Med 1995;333:1670–1676.
17. Effect of ramipril on mortality and morbidity of survivors of acute
myocardial infarction with clinical evidence of heart failure. The AcuteInfarction Ramipril Efficacy (AIRE) Study Investigators. Lancet 1993;
The study sponsors had no involvement in study design; in
the collection, analysis, and interpretation of data; in the
18. Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ Jr, Cuddy TE, Davis BR,
writing of the report; and in the decision to submit the
Geltman EM, Goldman S, Flaker GC. Effect of captopril on mortality and
morbidity in patients with left ventricular dysfunction after myocardialinfarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med 1992;327:669–677.
Conflict of interest: several of the authors have given industry-
19. Effect of enalapril on survival in patients with reduced left ventricular
sponsored lectures and taken part in clinical trials sponsored by
the industry, but there are no specific conflicts of interest related
Investigators. N Engl J Med 1991;325:293–302.
20. Randomised trial of cholesterol lowering in 4444 patients with coronary
heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet1994;344:1383–1389.
21. Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG,
Brown L, Warnica JW, Arnold JM, Wun CC, Davis BR, Braunwald E. The
1. EUROASPIRE. A European Society of Cardiology survey of secondary
effect of pravastatin on coronary events after myocardial infarction in
prevention of coronary heart disease: principal results. EUROASPIRE
patients with average cholesterol levels. Cholesterol and Recurrent
Study Group. European Action on Secondary Prevention through
Events Trial investigators. N Engl J Med 1996;335:1001–1009.
Intervention to Reduce Events. Eur Heart J 1997;18:1569–1582.
22. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R,
2. Lifestyle and risk factor management and use of drug therapies in coro-
Joyal SV, Hill KA, Pfeffer MA, Skene AM, the Pravastatin or Atorvastatin
nary patients from 15 countries; principal results from EUROASPIRE II
Evaluation and Infection Therapy—Thrombolysis in Myocardial Infarction
Euro Heart Survey Programme. Eur Heart J 2001;22:554–572.
22 Investigators. Comparison of intensive and moderate lipid lowering
3. Madsen M, Davidsen M, Rasmussen S, Abildstrom SZ, Osler M. The validity
with statins after acute coronary syndromes. N Engl J Med 2004;
of the diagnosis of acute myocardial infarction in routine statistics: a
comparison of mortality and hospital discharge data with the Danish
23. Ess SM, Schneeweiss S, Szucs TD. European healthcare policies for
MONICA registry. J Clin Epidemiol 2003;56:124–130.
controlling drug expenditure. Pharmacoeconomics 2003;21:89–103.
4. Gislason G, Abildstrom S, Rasmussen J, Rasmussen S, Buch P, Gustafsson I,
24. Abildstrom SZ, Rasmussen S, Madsen M. Changes in hospitalization rate
Friberg J, Gadsbøll N, Køber L, Stender S, Madsen M, Torp-Pedersen C. Nation-
and mortality after acute myocardial infarction in Denmark after
wide trends in the prescription of beta-blockers and angiotensin-converting
diagnostic criteria and methods changed. Eur Heart J 2005;26:990–995.
Chabad of Bradenton & Lakewood Ranch This year more people will experience the joy of Purim! Purim is one of the most joyous and fun holidays on the Jewish calendar. On Purim, we emphasize the importance of Jewish unity and friendship by sending gifts of food to friends and family. This Purim mitzvah is called Mishloach Manot. This year Chabad is sponsoring shared Mishloach Manot gift boxes
«Investoren zollen Novartis zu wenig Respekt» Die Performance der Novartis-Titel ist eine der schwächsten der Branche. Zu Unrecht, schreibt ein bekanntes US-Anlegermagazin und stellt sich damit gegen die meisten Analysten. Novartis habe den besten Geschäftsmix unter den grossen Pharma-Unternehmen und einer der stärksten Profit-Ausblicke, schreibt dieDiese Aussage steht quer in der Lan
 European Heart Journal (2006) 27, 1153–1158
Long-term compliance with beta-blockers,angiotensin-converting enzyme inhibitors,and statins after acute myocardial infarction
Gunnar H. Gislason1,2*, Jeppe N. Rasmussen2, Steen Z. Abildstrøm2,3, Niels Gadsbøll4,Pernille Buch1,2, Jens Friberg1, Søren Rasmussen2, Lars Køber5, Steen Stender6, Mette Madsen2,and Christian Torp-Pedersen1
1 Department of Cardiovascular Medicine, Bispebjerg University Hospital, Bispebjerg Bakke 23, DK-2400 Copenhagen NV,Denmark; 2 National Institute of Public Health, Copenhagen, Denmark; 3 Department of Cardiology, Gentofte UniversityHospital, Hellerup, Denmark; 4 Department of Internal Medicine, Roskilde County Hospital, Roskilde, Denmark; 5 Departmentof Cardiology, The Heart Centre, Rigshospitalet—National University Hospital, Copenhagen, Denmark; and6 Clinical Biochemistry, Gentofte University Hospital, Hellerup, Denmark
Received 10 October 2005; revised 5 December 2005; accepted 8 December 2005; online publish-ahead-of-print 6 January 2006
Aims To study initiation, dosages, and compliance with beta-blockers, angiotensin-converting enzyme
(ACE)-inhibitors, and statins in patients after acute myocardial infarction (AMI) and to identify likely
Methods and results Patients admitted with first AMI between 1995 and 2002 were identified by linking
nationwide administrative registers. A total of 55 315 patients survived 30 days after discharge and were
included; 58.3% received beta-blockers, 29.1% ACE-inhibitors, and 33.5% statins. After 1, 3, and 5 years,
78, 64, and 58% of survivors who had started therapy were still receiving beta-blockers, 86, 78, and 74%were receiving ACE-inhibitors, and 85, 80, and 82% were receiving statins, respectively. Increased ageand female sex were associated with improved compliance. The dosages prescribed were generally 50%or less of the dosages used in clinical trials, and dosages did not increase during the observation period.
European Heart Journal (2006) 27, 1153–1158
Long-term compliance with beta-blockers,angiotensin-converting enzyme inhibitors,and statins after acute myocardial infarction
Gunnar H. Gislason1,2*, Jeppe N. Rasmussen2, Steen Z. Abildstrøm2,3, Niels Gadsbøll4,Pernille Buch1,2, Jens Friberg1, Søren Rasmussen2, Lars Køber5, Steen Stender6, Mette Madsen2,and Christian Torp-Pedersen1
1 Department of Cardiovascular Medicine, Bispebjerg University Hospital, Bispebjerg Bakke 23, DK-2400 Copenhagen NV,Denmark; 2 National Institute of Public Health, Copenhagen, Denmark; 3 Department of Cardiology, Gentofte UniversityHospital, Hellerup, Denmark; 4 Department of Internal Medicine, Roskilde County Hospital, Roskilde, Denmark; 5 Departmentof Cardiology, The Heart Centre, Rigshospitalet—National University Hospital, Copenhagen, Denmark; and6 Clinical Biochemistry, Gentofte University Hospital, Hellerup, Denmark
Received 10 October 2005; revised 5 December 2005; accepted 8 December 2005; online publish-ahead-of-print 6 January 2006
Aims To study initiation, dosages, and compliance with beta-blockers, angiotensin-converting enzyme
(ACE)-inhibitors, and statins in patients after acute myocardial infarction (AMI) and to identify likely
Methods and results Patients admitted with first AMI between 1995 and 2002 were identified by linking
nationwide administrative registers. A total of 55 315 patients survived 30 days after discharge and were
included; 58.3% received beta-blockers, 29.1% ACE-inhibitors, and 33.5% statins. After 1, 3, and 5 years,
78, 64, and 58% of survivors who had started therapy were still receiving beta-blockers, 86, 78, and 74%were receiving ACE-inhibitors, and 85, 80, and 82% were receiving statins, respectively. Increased ageand female sex were associated with improved compliance. The dosages prescribed were generally 50%or less of the dosages used in clinical trials, and dosages did not increase during the observation period.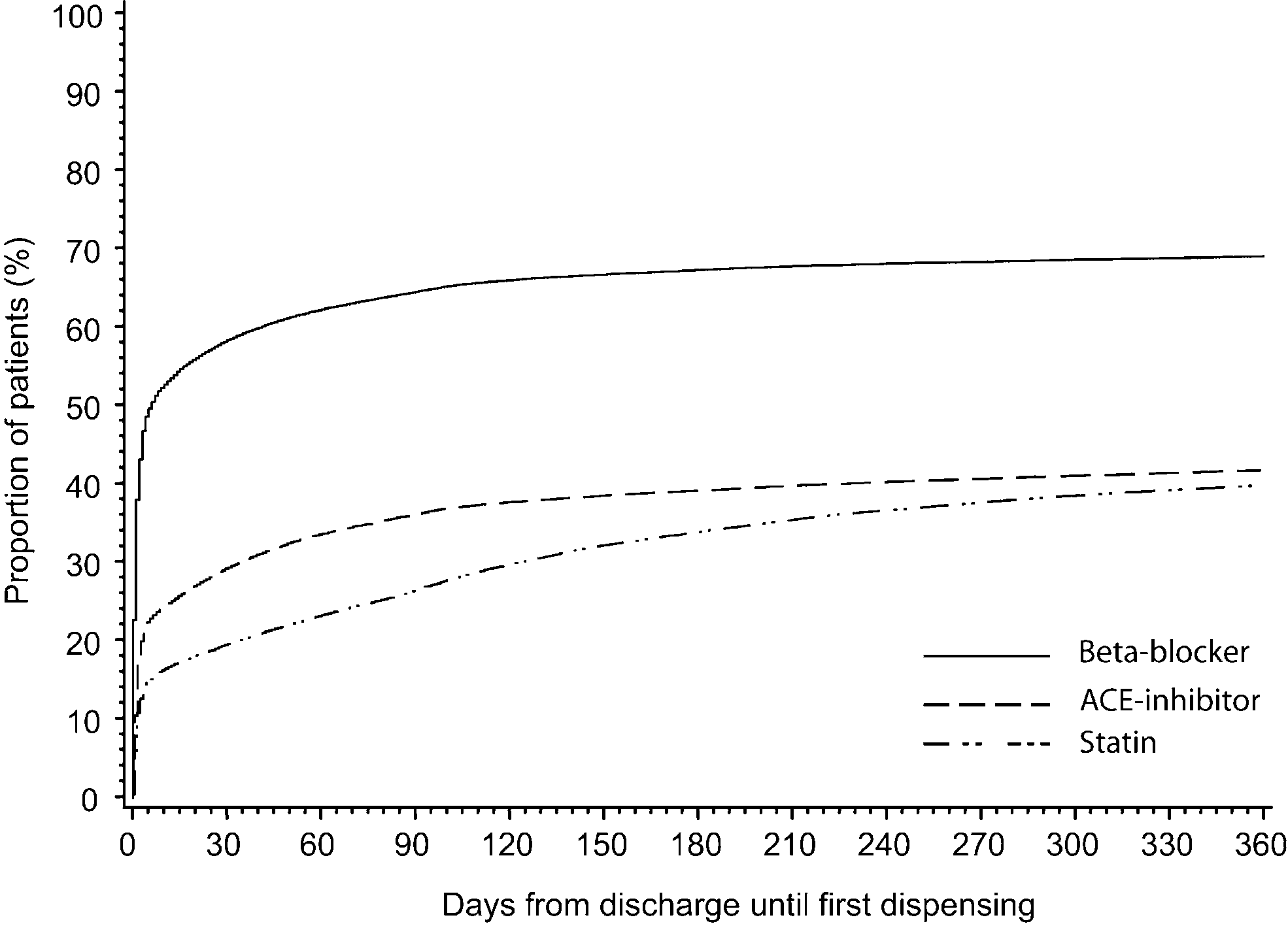 Long-term compliance with beta-blockers, ACE-inhibitors, and statins
least 90 days to analyse factors of importance for poor
Baseline characteristics of the study sample
The Cox multivariable proportional hazard analysis
(Table 4) revealed that although there were increasing
number of patients initiating treatment from 1995 to
2002, this did not affect compliance. On the contrary, com-
pliance improved with beta-blockers. Women had better
compliance with beta-blockers and statins than men, and
older patients had better compliance with beta-blockers
but worse compliance with ACE-inhibitors and statins.
Long-term compliance with beta-blockers, ACE-inhibitors, and statins
least 90 days to analyse factors of importance for poor
Baseline characteristics of the study sample
The Cox multivariable proportional hazard analysis
(Table 4) revealed that although there were increasing
number of patients initiating treatment from 1995 to
2002, this did not affect compliance. On the contrary, com-
pliance improved with beta-blockers. Women had better
compliance with beta-blockers and statins than men, and
older patients had better compliance with beta-blockers
but worse compliance with ACE-inhibitors and statins.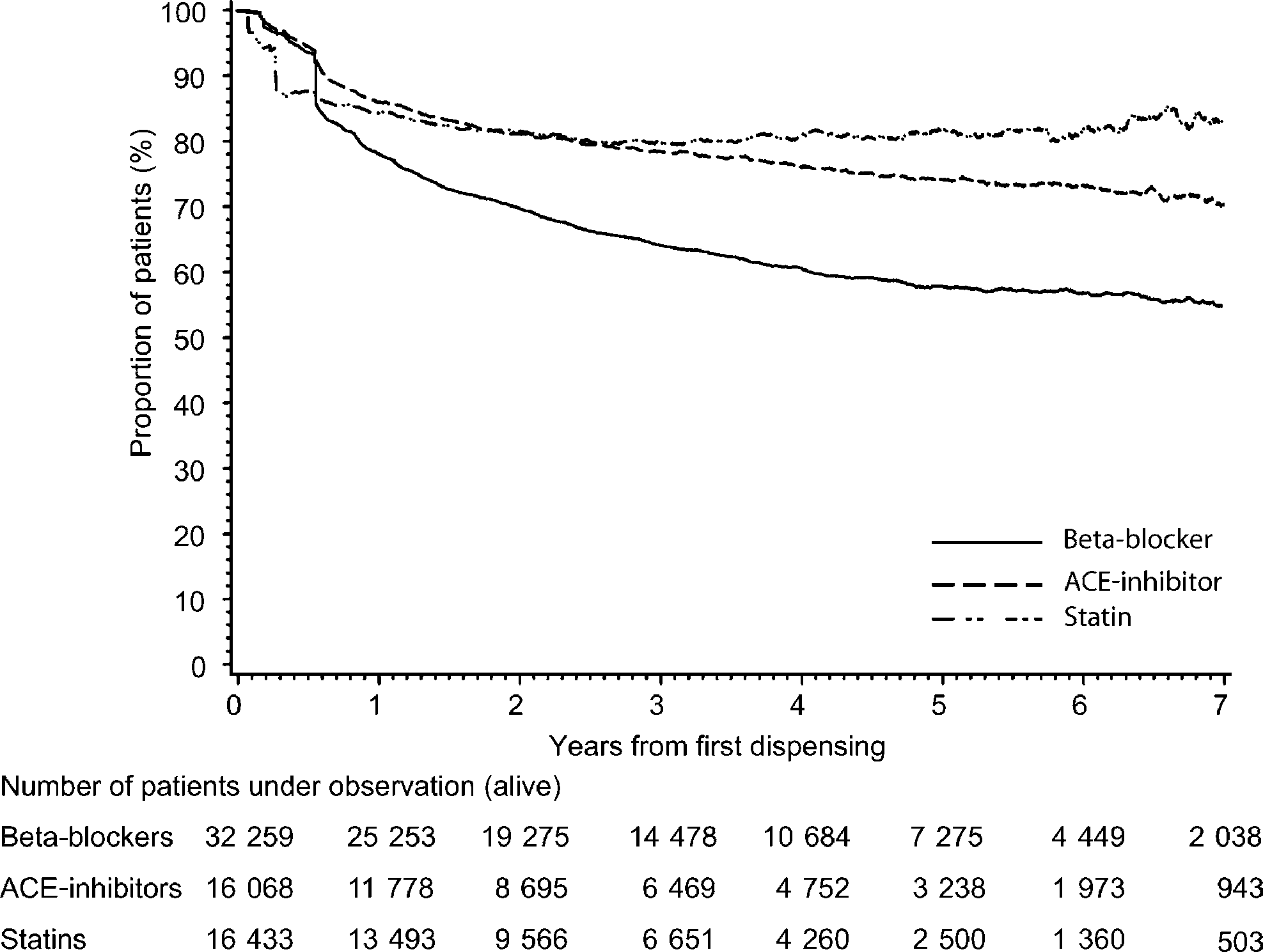 were written by hospital-based physicians, whereas general
practitioners initiated very few early prescriptions (Table 2).
were written by hospital-based physicians, whereas general
practitioners initiated very few early prescriptions (Table 2).