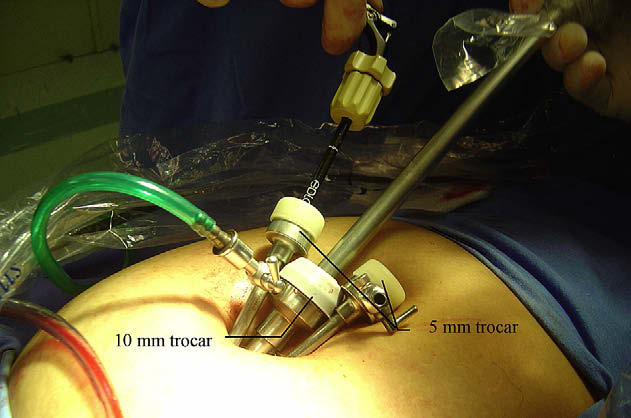
 Savaris. Ectopic pregnancy managed with LESS technique. Fertil Steril 2009.
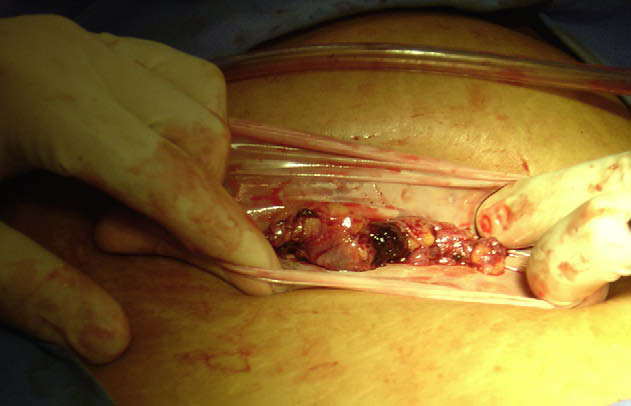
Savaris. Ectopic pregnancy managed with LESS technique. Fertil Steril 2009.cardiologiaclinica.cl
Diabetes, Síndrome Metabólico y Enfermedad CardiovascularHernán Prat M. Unidad de Factores de Riesgo, Depto. Cardiovascular, Hospital Clínico, Universidad de ChileEntre los factores de riesgo cardiovascular (FRC) más bió la conjunción de hipertensión, hiperglicemia y la gota como conocidos están la hipertensión arterial, el tabaquismo, la un síndrome.(4) Posteriormente, varias otra