Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients wellbutrin xl uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Guia_cuidados paliativos.indd
Appendix 6. Subcutaneous drug administration
Indications for use of subcutaneous route
The use of the subcutaneous route is indicated in those circumstances where the patient cannot take the medication orally or when the symptoms are not suffi ciently controlled by this route. In practice, the situations where the subcutaneous route is considered as a fi rst choice option are: uncontrolled nausea and vomiting, serious dysphagia, bowel occlusion syndrome that is not a surgical candidate, palliative sedation, unease, convulsions, and care in agony. Although not very frequent in daily practice, the situations that advise against the use of the subcutaneous route to administer drugs are anasarca, states of shock and severe coagulopathies.
Technique to use the subcutaneous route
The medication can be administered in two ways: in bolus or in continuous infusion using the de-vices (infusion pumps) that exist on the market. The latter are the best choice as the “bolus effect” is avoided and they permit the joint administration of mixtures of different drugs.
Infusion pumps can be elastomeric, mechanical or electronic depending on the mechanism
used. Many of them also permit the administration of drugs in bolus if required (due to break-through pain, for example).
Necessary material
• Infusion pump• Syringes• 25 G syringe driver type needle• Transparent dressing and adhesive strips• Saline solution or water for injection• Antiseptic solution (chlorhexidine, povidone-iodine)• Gloves
The procedure starts with the insertion of a 23-25 G metal needle syringe driver or a plastic
catheter into the subcutaneous cellular tissue and securing it with a transparent adhesive dressing that permits seeing the puncture area.
The most frequently used anatomic locations are the infraclavicular anterior thoracic area,
deltoideal area, the abdomen and the anteroexternal side of the thigh, avoiding areas with skin problems (fi gure 1).
It is advisable to periodically check the area where the syringe driver has been inserted to
detect local problems (hardening or oedema, reddening, infection, haematoma) that may compro-mise the absorption of the medication or the accidental release of the syringe driver. The point of insertion of the syringe driver will be changed when local problems appear that may make absorp-tion diffi cult. The administration in bolus with volumes of more than 2 ml will be avoided as this is more painful and favours the appearance of hardening and erythema, above all in the case of repeated injections.
CLINICAL PRACTICE GUIDELINE FOR PALLIATIVE CARE
Figure 1. Recommended puncture areas for subcutaneous route
(modifi ed and reproduced with the permission of Fisterra http://www.fi sterra.com/mate-rial/tecnicas/parenteral/subcutanea.asp)
Medication administered by subcutaneous route
Several drugs can be administered at the same time although their compatibility in one single device has not been well-established on many occasions.
Table 1. Most commonly used drugs by SC route in PC Indications Presentations
Amp 1 ml 1% = 10 mg Amp 1 ml 2% = 20 mg Phial 20 ml 2% = 400 mg
Premortem death rattles, sialorrhoea, respiratory Amp 1ml = 20 mgsecretions, bowel obstruction
Nausea and vomiting due to opioids, vomiting in
Amp 1 ml = 0,05 mg Amp 1 ml = 0,1 mg Phial 5 ml = 1 mg
Other drugs that have been used by SC route are: bupivacaine, buprenorphine, calcitonin, ceftri-axone, clonazepam, scopolamine, fentanyl, furosemide, granisetron, hydromorphone, hydrozy-cine, ketamine, methadone and ondansetron, among others. Infusers
Infusers are devices especially designed to infuse the medication constantly and continuously. Its use permits the mixture of drugs and their simultaneous infusion by subcutaneous route. There are several types of infusers on the market: elastomeric (with ball mechanism), mechanical (with spring or syringe mechanism) and electronic (with peristaltic type mechanism). Many of them also permit the administration of drugs in bolus if required (due to appearance of breakthrough pain, for example).
The following variables must be taken into account when loading the infuser:
• The autonomy time: one day, 5 days or 7 days, normally
• The total fi ll volume measured in ml, which is related to the above two parameters. Thus,
the total fi ll volume of a one-day infuser with a outlet fl ow of 2.1 ml/h is 50 ml (2.1 ml/h x 24 h).
The cumulative volume of the drugs to administer is calculated with these reference vari-
ables and according to their presentation formats, completing the total capacity of the device with saline solution or water for injection. Examples: a patient requires mg of morphic chloride, 5 mg of haloperidol and 30 mg of
metoclopramide a day to control nausea and vomiting. We have a 1-day elastomeric pump with an outlet fl ow of 2.1 ml/hour and a fi ll volume of 50 ml.
• 50 mg Morphine = 5 1-ml ampoules of 1% morphic chloride = 5 ml
• 5 mg Haloperidol = 1 1-ml ampoule = 1 ml
• 30 mg Metoclopramide = 3 2-ml ampoules = 6 ml
In all, the medication occupies a volume of 12 ml; the volume of saline solution we will use
to fi ll the pump is 38 ml saline solution (50 ml total volume – 12 ml medication).
When the medication needs are known and stable, an infuser for several days can be used. In
the above case, if we have a 5-day infuser with an outlet fl ow of 1.5 ml/h and a fi ll volume of 275 ml, the preparation would be done as follows:
• Morphine 50 mg/day = 250 mg/5 days = 25 amp 1% = 25 ml
• Haloperidol 5 mg/day = 25 mg/5 days = 5 amp = 5 ml
• Metoclopramide 30 mg/day = 150 mg/5 day = 15 amp = 30 ml
In this case the medication occupies a volume of 60 ml, so the volume of saline solution
necessary to completely fi ll the device is 215 ml (275- 60 ml).
CLINICAL PRACTICE GUIDELINE FOR PALLIATIVE CARE
Compatibility of mixtures
• In our setting, the dilution is generally done with saline solution, as its tonicity is very
similar to physiological solution, except for drugs such as diamorphine or cycline where dilution in water for injection is recommended (diamorphine is a widely used drug in Anglo-Saxon countries but it is not available in our setting). Water for injection has a lower risk of precipitation, so some sources recommend its use when making mixtures of several drugs (except when octreotide or ketamine are used); it is also advisable to dilute mixtures in order to reduce the risk of precipitation.
• Dexamethasone and ketorolac must not be mixed with other drugs.
• It is advisable to throw away any mixture that produces precipitates or solution turbidity.
• It is recommended not to mix more than three drugs due to the increased risk of precipita-
The most commonly used mixtures include morphine, butylscopolamine and midazolam,
normally used in agony situations, and the mixture comprised of morphine, haloperidol and bu-tylscopolamine, used for the palliative treatment of the bowel occlusion syndrome.
Table 2, modifi ed from Porta et al., shows some of the mixtures of 3 compatible drugs used
in clinical practice that include morphine. Information about the compatibility of mixtures can be consulted at http://www.pallcare.info/
Table 2. Compatible mixtures of three drugs that include morphine
This appendix has been prepared based on the following references:
1. Porta-Sales J, Gomez-Batiste X, Tuca A, editores. Manual de control de síntomas en pacientes con cáncer avan zado y terminal.
2. NHS Greater Glasgow, Acute Services Division, Palliative Care Practice Development Team. Guidelines for the use of Subcutaneous
Medications in Palliative Care. March 2007 Available at en: http://www.palliativecareglasgow.info/pdf/guidelines_subcutaneous_meds_corrected.pdf
3. Department of Pharmacy, Auckland District Health Board. Compatibility of syringe drives admixtures for continuo- us subcutane-
ous infusion. Available at: http://www.nzhpa.org.nz/SDAdCompProj.pdf
4. Dickman A, Scheneider J, Varga J: The Syringe Driver. Continuous subcutaneous infusions in palliative care. Oxford University
Blood Pressure, 2011; Early Online, 1–4 ORIGINAL ARTICLE Masked hypertension unfavourably affects haemostasis parameters D. P. PAPADOPOULOS 1 , C. THOMOPOULOS 2 , I. MOUROUZIS 1 , A. KOTROTSOU 1 , E. SANIDAS 1 , U. PAPAZACHOU 2 , M. DASKALAKI 2 & T.K. MAKRIS 2 1 ESH Excellent Center of Hypertension, Laiko Univesity Hospital, Athens, Greece, 2 ESH Excellent Center of Hyp
Broad Band Light (“Reds”) - Pre and Post Treatment Guidelines Pre-Treatment Guidelines To decrease the chance of unwanted side effects, avoid tanning the skin for 6 weeks prior to treatment Make sure all sunless tanners have faded prior to your laser treatment (1 week is a typical time period for wearing off of sunless tanners) For Cold Sore Sufferers --Take your Anti-
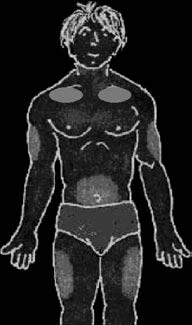 Figure 1. Recommended puncture areas for subcutaneous route
Figure 1. Recommended puncture areas for subcutaneous route