Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients kamagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Microsoft word - domsstudy v5 kong.doc
The study has two primary purposes. The first is to assess whether patients using ActiPatch for treatment of Delayed Onset Muscle Soreness (DOMS) realize reduced levels of muscle pain or soreness when the ActiPatch device is applied after a DOMS inducing exercise regiment. The second is to assess the effectiveness of treatment of DOMS with ActiPatch versus acetaminophen in the form of Extra Strength Tylenol®.
This was an observational study to evaluate the treatment of Delayed Onset Muscle Soreness (DOMS). After a vigorous resistance training exercise regiment designed to induce DOMS, 102 study participants were placed into one of three groups, : 1) a control group, 2) a group that utilized the ActiPatch device, and 3) a group that received over-the-counter strength acetaminophen in the form of Extra Strength Tylenol after a vigorous resistance training exercise regiment designed to induce DOMS. . Each participant was engaged in a vigorous resistance based exercise regiment designed to induce DOMS in the bicep muscles. Upon completion of the exercise regiment, participants selected for the ActiPatch group were given ActiPatch devices which were placed on the bicep muscles. These participants wore the devices for the subsequent 48 hour period. All participants in the study returned 48 hours later. Participants in the control and ActiPatch groups were then surveyed concerning their levels of DOMS-related muscle pain and soreness. Participants within the acetaminophen group were administered 1 gram of acetaminophen in the form of Extra Strength Tylenol. Ninety minutes after administration of acetaminophen these study participants were also surveyed concerning their levels of DOMS- related muscle pain and soreness. Study was approved by RCRC Independent Review Board of Austin, Texas and has been registered with The National Institutes of Health (NIH).
The ActiPatch device manufactured by BioElectronics Corporation. was used by one group of study participants. A different group was given over-the-counter strength of acetaminophen in the form of Extra Strength Tylenol. The dosage of acetaminophen was 1 gram. The control group used neither the ActiPatch device nor acetaminophen.
Of the the 102 patients were enrolled in the study, . 38 used the ActiPatch device, 38 acted as control, and 26 used acetaminophen in the form of Extra Strength Tylenol. The mean VAS score for the ActiPatch was 1.500, significantly below the VAS scores of 2.507 for the acetaminophen group and 3.179 for the control group. Comparison between the ActiPatch group and the control group was significant at the .001 level. Comparison between the ActiPatch group and the acetaminophen group was significant at the .05 level. No study related adverse effects were reported by any participant.
The data yielded by this study appears to demonstrate that the use of ActiPatch for the treatment of Delayed Onset Muscle Soreness (DOMS) is both safe and effective. Additionally, the data yielded by the study appears to demonstrate that the continuous use of ActiPatch will result in significantly less DOMS-related pain and muscle soreness compared to a treatment regiment consisting of an OTC dosage of acetaminophen.
This was an observational study to evaluate the treatment of delayed onset muscle soreness.
Study participants were placed randomly into one of three groups 1) a control group, 2) a group that utilized ActiPatch, and 3) a group that received over-the-counter strength acetaminophen
102 participants in total - 38 used the ActiPatch, 38 acting as control, and 26 used acetaminophen
Sample size for acetaminophen group was smaller due to resistance from participants to consume acetaminophen
Aged range from 18 to 35, subjects were healthy collegiate athletes and trainers who exercise regularly and participate in team sports
Interventions were approximately 20 sets of 10 repetitions of bicep resistance exercises using free weights to induce DOMS in the bicep muscles of both arms
Approximately 48 hours post exercise, participants returned to study site and were given a Pain Recording Scale (Visual Analogue Scale) sheet to record their perceived level of DOMS pain in their bicep muscles.
Anyone who is unable to give consent or document written consent in English
Anyone who is confirmed or who could possibly be pregnant
Anyone with allergy or intolerance to acetaminophen
Participants were recruited from collegiate athletic teams and athletic training personnel.
After the DOMS inducing resistance exercise regiment was completed, each study participant was randomly assigned to one of the three participating groups. Study participants assembled randomly in a straight line. The number of participants in the line was divided by three. Starting left to right of the line the three groups were selected with the first third becoming the ActiPatch group, second third becoming the control group and the final third becoming the acetaminophen group.
As described in the informed consent forms, all adverse events were to be reported to the investigating physician or the collegiate athletic training personnel. Participants were given the direct phone number to the principal investigator. No adverse events were reported to either the principal investigator for the
Measurements of DOMS-related muscle pain assessments were done by the participants who completed a simple form that recorded pain and muscle soreness levels on the VAS line. The data was collected by the athletic training personnel under the supervision of the principal investigator. The pPrincipal investigator transferred the data to a spreadsheet from which statistical analysis was performed.
Data was collected from the participants approximately 48 hours after the administration of the DOMS inducing resistance exercise regiment using a VAS (Visual Analogue Score) pain assessment.
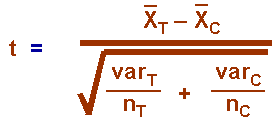
Data were collected at the end of the study. The monitor copied the data from the individual sheets and placed in a spread sheet with one entry per participant depending on the participant’s particular group, i.e., Tylenol, Control or Actipatch. Thus there were three columns, one for each group. At the end of the study, the data were provided for analysis. The data were analyzed using Excel macro’s. Means, variances and standard deviations for the VAS scores were calculated for each subsample. The difference between cell means was tested using t-tests using with the following formula:
where X is the mean for the group, VAR is the variance of the observations, n is the sample size and the subscripts T and C represent the two different groups being compared, e.g. “treatment” and “control” group.
This study used two tailed tests and significance levels of .05, .025 and .001 to determine the significantsignificance differences in sample means.
102 patients were enrolled in this study, 38 using the Actipatch, 38 acting as control, and 26 using Tylenol. Table 1 shows the mean VAS scores for each subsample along with the variances for these means, i.e., var/n .
Table 2 presents the results of the individual t-tests. Comparisons were made between Actipatch and the control group and Actipatch and the Tylenol group. The former comparison was significant at the .001 level; the latter was significant at the .05 level.
The data from this study demonstrated demonstrates that the ActiPatch device manufactured by BioElectronics Corporation. had a significant effect on reducing DOMS DOMS-related symptoms of muscle pain and soreness when compared to both a control group that received no treatment and a group that was treated with 1 gram of acetaminophen in the form of Extra Strength Tylenol. Based on this data, the principal investigator concludes that ActiPatch is safe and effective treatment for DOMS. The use of ActiPatch seems to be a convenient, safe and effective new treatment for muscle pain and soreness, especially when compared to currently FDA approved over the counter treatments, such as acetaminophen, NSAIDs and other pain medications that may have questionable safety profiles for many people.
Delayed Onset Muscle Soreness (DOMS) is a condition associated with increased physical exertion. This condition is experienced by all individuals regardless of fitness level as it is a normal physiological response to increased exertion and the introduction of unfamiliar or strenuous physical activities. The pain caused by DOMS can impair physical training and performance, and as a result, it is of great concern to trainers, coaches, and therapists. DOMS affects many more individuals than just athletes athletes. Many ordinary with many ordinary people are developing this condition as a result of excessive physical or out of the ordinary exertion. The pain and discomfort associated with this condition generally peaks at between 36 to 72 hours after an exercise routine and usually resolves within 96 hours. For several decades DOMS had been attributed to lactic build up in the muscles after exertion. Over the past few years this assumption has been shown to be unrelated to this condition. Several research studies have indicated that lactate levels return to normal within 60 minutes post exercise. Therefore, increased lactate levels cannot cause DOMS. DOMS is predominately caused by eccentric exercise. Connolly et al. (2003) explains that the injury that results from eccentric exercise causes damage to the muscle cell membrane, which sets off an inflammatory response. The inflammatory response leads to the formation of metabolic waste products, which act as chemical stimulus to the nerve endings that directly cause a sensation of pain and swelling. W. Stauber et al (2000) used a high-powered microscope to analyze muscle fibers after an intense workout. Based on his research it was clear that cell membranes were ruptured and other structural components were disrupted; however, damage to the muscle fibers is relatively small. This damage is not limited to one area, but occurs throughout the muscle fiber. This microscopic muscle damage causes an inflammatory response. It is this inflammatory response that causes muscle soreness due to, : 1) the accumulation of fluid (swelling) and 2) chemicals secreted by white blood cells that activate pain receptors (Smith, 1991). While there has been some research conducted on the treatment of DOMS, no particular treatment option has been proven to be dominant in treating or preventing the condition. The most popular intervention is pharmacological options using non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen. Stretching and warm-up exercises as well as nutritional augmentation via supplements have also been explored with varying degrees of success. NSAIDs, such as aspirin and ibuprofen, and acetaminophen are popular treatments for DOMS, but some of the research conducted in this area is inconclusive. Additionally, there are significant concerns associated with negative potential side effects such as gastrointestinal distress, liver toxicity and related coronary issues.
There has been considerable research relative to using nutritional supplementation as a potential treatment for DOMS, with particular emphasis on vitamins E and C and other antioxidants, which are thought to reduce the proliferation of free radicals that are generated during an inflammatory response. These effects are inconclusive as are other investigations into use of L-carnitine. While neither NSAIDs nor nutritional supplements have been proven to reduce the onset of DOMS, there has been some research suggesting that simple warm-up exercises can meaningfully reduce the onset of the condition. Szymanski (2003) introduced the “repeated-bout effect” as a way to reduce DOMS. The repeated-bout is a progressive adaptation to exercise that has been shown to consistently reduce DOMS and exercise induced damage to muscles. ActiPatch is a miniaturized medical device that delivers continuous electromagnetic therapy to restore damaged cells. The device is a Class III medical device that is available only through a licensed health care practitioner in the United Statesand it is not generally available to the American public. The device, however, is widely available on an over-the-counter basis outside of the United States. Significant clinical data shows that ActiPatch reduces edema, inflammation and pain. ActiPatch uses a mild electrical current and radiofrequency waves at a frequency that stops the release of pain and inflammatory mediators, increasing blood flow, and reestablishing normal cell interaction. Pulsed electromagnetic stimulation (PEMF) in some form has been used or investigated since the early 1930s. There is a large body of clinical experience that has realized its value as an effective treatment for tissue trauma, particularly in the early stages of inflammation. Numerous studies are available that document its effectiveness in orthopedic surgery, arthritis, and even plastic surgery (breast augmentation). While no study has demonstrated the complete elimination of pain, PEMF has shown less dependence on medications and some enhancement of the recovery period. Also, there has not been a single study showing any harmful effects so it is safe to conclude that PEMF is safe for human use. The precise mechanism by which PEMF works on controlling pain after injury is not known. It is theorized that it may affect pain levels by its effect of nitric oxide (NO) release, a short-lived signaling molecule in the anti-inflammatory cascade. It is also suggested that it has an effect on stabilizing cell membranes such that the edema phase of an injury is more rapidly resolved. AtciPatch Allay patches (ActiPatch)devices function at a frequency in the 27.1 MHz ISM band and are confined within the field of the patch’s loop antenna. The patch induces electric current in human tissue tissue, but it is oscillating at such a high frequency that it cannot be detected by the patient. The high frequency results in a depth of penetration into the tissues of approximately 10 cm. When the patch is used over a 24 hour period, it produces an absorbed energy of 630 mJ/cc which is well within the range of effectiveness for soft tissue injuries. The patch produces a power density at the skin surface between 14 and 73 µW/cm² and induces an electrical field of about 10 milliVolt/cm, resulting in adsorbed power
levels in the range of 7.3 µW/cm3. This provides field exposure levels at the target tissue that are five to nine orders of magnitude above the thresholds which have been established for non-thermal electromagnetically induced biological effects at the cell and tissue level. The ActiPatch uses proven medical technology to truncate the human body’s natural inflammatory response breaking the cycle of chronic inflammation. ActiPatch does this by delivering pulsed electromagnetic energy directly to the affected area and driving out the edematous fluid along with byproducts of the damaged tissue. The effect affect is a well documented and a significant overall improvement in the restorative and recovery process following injury resulting in a substantial in a significant reduction in the pain associated with soft tissue injury. These statements are supported by multiple studies, but no specific research has been done relative to its effects for on DOMS. ActiPatch was cleared by FDA in 2002 for the treatment of edema following blepharoplasty. Clinical data presented by BioElectronics to Health Canada resulted in its approval for relief of pain in musculoskeletal complaints, and the product is now available over-the-counter throughout Canada. The product is also cleared for over-the-counter sales in all 27 European Union countries and other , in addition to dozens of other countries throughout the world.
Delayed Onset Muscle Soreness Study
Clinical Study Protocol PROTOCOL NUMBER B565V2 - October 14, 2009 Title: Use of ActiPatch device for treatment of delayed Onset Muscle Soreness. Physician: Sheena Kong, M.D. San Francisco, California
Background Delayed Onset Muscle Soreness
Delayed Onset Muscle Soreness (DOMS) is a condition associated with increased physical exertion. This condition is experienced by all individuals regardless of fitness level as it is a normal physiological response to increased exertion and the introduction of unfamiliar or strenuous physical activities. The pain caused by DOMS can impair physical training and performance and as a result it is of great concern to trainers, coaches, and therapists. DOMS affects many more individuals than just athletes with many ordinary people developing this condition as a result of excessive physical or out of the ordinary exertion. The pain and discomfort associated with this condition generally peaks at between 36 to 72 hours after an exercise routine and usually resolves within 96 hours. For several decades DOMS had been attributed to lactic build up in the muscles after exertion. Over the past few years this assumption has been shown to be unrelated to this condition. Several research studies have indicated that lactate levels return to normal within 60 minutes post exercise. Therefore, increased lactate levels cannot cause DOMS. DOMS is predominately caused by eccentric exercise. Connolly et al. (2003) explains that the injury that results from eccentric exercise causes damage to the muscle cell membrane, which sets off an inflammatory response. The inflammatory response leads to the formation of metabolic waste products, which act as chemical stimulus to the nerve endings that directly cause a sensation of pain and swelling. W. Stauber et al (2000) used a high-powered microscope to analyze muscle fibers after an intense workout. Based on his research it was clear that cell membranes were ruptured and other structural components were disrupted however, damage to the muscle fibers is relatively small. This damage is not limited to one area, but occurs throughout the muscle fiber. This microscopic muscle damage causes an inflammatory response. It is this inflammatory response that causes muscle soreness due to, 1) The accumulation of fluid (swelling) and 2) chemicals secreted by white blood cells that activate pain receptors (Smith, 1991). Interventions While there has been some research conducted on the treatment of DOMS, no particular treatment option has been proven to be dominant in treating or preventing the condition. The most popular intervention is pharmacological options using non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen. Stretching and warm-up exercises as well as nutritional augmentation via supplements have also been explored with varying degrees of success. NSAIDs, such as aspirin and ibuprofen, and acetaminophen are popular treatments for DOMS, but some of the research conducted in this area is inconclusive. Additionally, there are significant concerns associated with negative potential side effects such as gastrointestinal distress, liver toxicity and related coronary issues. There has been considerable research relative to using nutritional supplementation as a potential treatment for DOMS, with particular emphasis on vitamins E and C and other antioxidants, which are thought to reduce the proliferation of free radicals that are generated during an inflammatory response. These effects are inconclusive as are other investigations into use of L-carnitine. While neither NSAIDs nor nutritional supplements have been proven to reduce the onset of DOMS, there has been some research suggesting that simple warm-up exercises can meaningfully reduce the onset of the condition. Szymanski (2003) introduced the “repeated-bout effect” as a way to reduce DOMS. The repeated-bout is a progressive adaptation to exercise that has been shown to consistently reduce DOMS and exercise induced damage to muscles. Use of ActiPatch As a Potential Alternative Treatment ActiPatch is a miniaturized medical device that delivers continuous electromagnetic therapy to restore damaged cells. The device is a Class III medical device that is available only through a licensed health care practitioner and it is not generally available to the American public. The device, however, is widely available on an over-the-counter basis outside of the United States. Significant clinical data shows that ActiPatch reduces edema, inflammation and pain. ActiPatch uses a mild electrical current and radiofrequency waves at a frequency that stops the release of pain and inflammatory mediators increasing blood flow and reestablishing normal cell interaction. Pulsed electromagnetic stimulation (PEMF) in some form has been used or investigated since the early 1930s. There is a large body of clinical experience that has realized its value as an effective treatment for tissue trauma, particularly in the early stages of inflammation. Numerous studies are available that document its effectiveness in orthopedic surgery, arthritis, and even plastic surgery (breast augmentation). While no study has demonstrated the complete elimination of pain, PEMF has shown less dependence on medications and some enhancement of the recovery period. Also, there has not been a single study showing any harmful effects so it is safe to conclude that PEMF is safe for human use. The precise mechanism by which PEMF works on controlling pain after injury is not known. It is theorized that it may affect pain levels by its effect of nitric oxide (NO) release, a short-lived signaling
molecule in the anti-inflammatory cascade. It is also suggested that it has an effect on stabilizing cell membranes such that the edema phase of an injury is more rapidly resolved. Allay patches (ActiPatch) function at a frequency in the 27.1 MHz ISM band and are confined within the field of the patch’s loop antenna. The patch induces electric current in human tissue but it is oscillating at such a high frequency that it cannot be detected by the patient. The high frequency results in a depth of penetration into the tissues of approximately 10 cm. When the patch is used over a 24 hour period, it produces an absorbed energy of 630 mJ/cc which is well within the range of effectiveness for soft tissue injuries. The patch produces a power density at the skin surface between 14 and 73 µW/cm² and induces an electrical field of about 10 milliVolt/cm, resulting in adsorbed power levels in the range of 7.3 µW/cm3. This provides field exposure levels at the target tissue that are five to nine orders of magnitude above the thresholds which have been established for non-thermal electromagnetically induced biological effects at the cell and tissue level. The ActiPatch uses proven medical technology to truncate the human body’s natural inflammatory response breaking the cycle of chronic inflammation. ActiPatch does this by delivering pulsed electromagnetic energy directly to the affected area and driving out the edematous fluid along with byproducts of the damaged tissue. The effect is a well documented and significant overall improvement in the restorative and recovery process following injury in a significant reduction in the pain associated with soft tissue injury. These statements are supported by multiple studies, but no specific research has been done relative to its effects for DOMS. ActiPatch was cleared by FDA in 2002 for the treatment of edema following blepharoplasty. Clinical data presented by BioElectronics to Health Canada resulted in its approval for relief of pain in musculoskeletal complaints and the product is now available over-the-counter throughout Canada. The product is also cleared for over-the-counter sales in all 27 European Union countries, in addition to dozens of other countries throughout the world. Study Aims This study will evaluate the effects of ActiPatch relative to the treatment of delayed onset muscle soreness (DOMS). Use of the ActiPatch will be compared to a control group of individuals that will receive no treatment and to a group that will receive over-the-counter strength acetaminophen. The overall goals of the study are the following:
• Determine if ActiPatch is an effective treatment for DOMS • Determine the relative effectiveness of ActiPatch versus acetaminophen
Study Design Summary
This will be an observational study to evaluate the treatment of delayed onset muscle soreness.
Study participants will randomly placed into one of three groups 1) a control group, 2) a group that utilizes ActiPatch, and 3) a group that will receive over-the-counter strength acetaminophen
There will be approximately 105 participants in total with approximately 35 in each group
Age range of 18 to 35, subjects will be healthy collegiate athletes who exercise regularly and participate in team sports
Interventions will be approximately 20 sets of 10 repetitions of bicep resistance exercises using free weights to reduce DOMS in the bicep muscles of both arms
Approximately 48 hours post exercise, participants will be given a Pain Recording Scale sheet to record their perceived level of bicep- related DOMS pain.
Study Specifics
Study participants will be placed randomly in one of three groups: 1) A Control Group 2) An ActiPatch Usage Group 3) Acetaminophen Dosage Group Each group will engage in resistance training of the bicep muscle of each arm in order to induce DOMS. The training regimen will be supervised by a highly trained collegiate coaching staff that regularly administers weight training exercises. Additionally, the collegiate athletic director will be on-site to supervise activities, as will principal investigator, Sheena Kong, MD. Each participant will engage in approximately 20 sets of 10 repetitions of eccentric arm curls to induce DOMS in the bicep of each arm. Participants in the ActiPatch usage group will have ActiPatch devices placed and secured over each bicep upon completion of the exercise regiment. These devices will continue to be worn, except during bathing, for a 48 hour period. Approximately 48 hours post exercise regiment all participants will meet with the principal investigator. Activities at this meeting will consist of the following:
• The Control Group - Participants in the control group will complete a pain evaluation survey to
determine the level of DOMS being experienced.
• ActiPatch Usage Group - Participants in the ActiPatch usage group will have the ActiPatch
removed and will then complete a pain evaluation survey to determine the level of DOMS
• Acetaminophen Dosage Group - Participants in the acetaminophen dosage will be provided with
one gram of over-the-counter acetaminophen in the form of Extra Strength Tylenol®. Participants in this group will wait for one hour and then complete a pain evaluation survey to determine the level of DOMS being experienced.
Study Participant Exclusions The following groups of individuals will be excluded:
• Anyone unable to give consent or document written consent in English • Anyone confirmed or who could possibly be pregnant • Anyone with allergy or intolerance to acetaminophen • Anyone with known active liver disease
Potential Risks and Benefits Benefits: evaluation of the ActiPatch device and acetaminophen for treatment of DOMS Risk: In thousands of uses of the ActiPatch not a single safety issue has ever been raised. FDA has cleared the device for the treatment of edema after blepharoplasty (eyelid surgery) and the device is widely used off label by dozens of physicians throughout the United States. Additionally, as is outlined above, the device is cleared by Health Canada and the European Union for over-the-counter sales and is widely available in dozens of additional countries. Because the device is placed on the skin over the bicep muscle there is a slight possibility of extremely low level skin irritation from wearing the patch. Risk of taking acetaminophen is very low as all participants will receive dosages well below daily OTC limits. VII. Monitoring and Reporting of Adverse Effects Principal investigator will be on-site during administration of protocol to monitor any adverse effects. This may include any exercise related issues, application of ActiPatch devices or administration of OTC dosages of acetaminophen. Additionally, principal investigator has made her telephone number of available to all study participants on a 24 hour per day basis so that any participant may report any adverse effects or any other issues that may arise. Principal investigator will log any and all adverse effects reported by participants or any observed during the investigation of this protocol. All such adverse effects, if any, will be promptly logged and reported
to both research sponsor and RCRC IRB via written communications.
VIII. Maintenance of Study and Participant Records All records will be assembled and recorded by principal investigator. Records will be stored as principal investigator's office in a secured manner. Records stored at principal investigator’s office will be stored in a locked file cabinet located within a separated and locked private office. No other personnel will have access to these files during administration of study protocol.
Acetaminophen Comparative Study Dr. Sheena Kong Subject Name:_________________________________________________ PAIN RECORDING SCALE
Are you experiencing pain as a result of the exercise regiment: (Please circle the correct answer) YES or NO If you are experiencing pain or discomfort as a result of the exercise regiment please answer the following: Pain Day - Day Two Place a mark on the line your estimate of the amount of pain you felt today. And give a number from 1 to 10 below your mark.
(none) (annoying) (uncomfortable) (dreadful) (agonizing)
Delayed onset muscle soreness study Dr. Sheena Kong PATIENT INFORMED CONSENT Title: Delayed Onset Muscle Soreness Study - Comparison between ActiPatch PEMF Device and Acetaminophen
Sponsor:
BioElectronics Corp Frederick, Maryland Investigator: Sheena Kong, MD Phone:
(925) 922- 2560 Research Site: Diablo Valley College Pleasant Hill, California Participant:
______________________________________________________
______________________________________________________
______________________________________________________
This consent form may contain words that you do not understand. Please ask Dr. Kong to explain any words or information that you do not understand. Introduction You are being invited to participate in a research study. Before you decide to take part in the study, you should read this document. This document, called and informed consent document, explains the study. Please ask as many questions as needed so that you can decide if you want to be in the study. To be in this research study, you cannot already be in another medical research study. Please be honest and complete in providing your answers.
Purpose of the Study This study is being sponsored by BioElectronic Corporation. The study is designed to determine the pain relieving properties of a medical device called ActiPatch. The effects of ActiPatch will be compared to the effects of acetaminophen. ActiPatch is an FDA cleared device, but should be considered in “investigational device” relative to the treatment of delayed onset of muscle soreness. ActiPatch is available over the counter in Canada, all 27 countries of the European Union, and in dozens of other countries around the world. Within the United States it is available by prescription. You will be randomly, meaning you will be assigned by chance, like the flip of a coin, into one of three groups. 1) a control group that will receive no treatment, 2) a group that will wear the ActiPatch medical device for 48 hours, or 3) a group that will take over-the-counter acetaminophen. All of the participants will rate their degree of delayed onset muscle soreness 48 hours after weight training exercises. You may or may not be informed of the results of this study. The study doctor is not being compensated to conduct this research trial. What Will Happen During the Study
During the study you will exercise in a manner similar to your normal exercise routines except you will receive additional exercise to induce a condition called DOMS, which stands for Delayed Onset Muscle Soreness. This is simply soreness that results from exercise. All exercise routines will be supervised by the coaching staffs that you already know very well. The exercise routine will be completed in your normal training facility. In addition, Dr. Sheena Kong will be present to supervise. Length of the Study and Number of Participants Expected to Take Part in the Study
There will be approximately 130 to 150 total participants in the study. The ages will range from 18 to 35 years old. The exercise routine will take place during a single day, with results recorded approximately 48 hours later. Side Effects and Risks The ActiPatch device is extremely safe and has been used by thousands of patients through out the world without a single safety issue ever being raised. The device is placed on the skin and is attached using a comfortable to wear Velcro strap. The only known possible side effect is the very slight possibility of a very minor skin irritation of the skin where the device is placed. The chance of this side effect is very slight and if it does occur it is very minor.
Those to be excluded from the study There are some individuals who could possibly suffer for some adverse effects from participating in the study. Therefore, the following individuals are not able to participate in the study and will be excluded. If any of these apply to you please do not sign this consent form:
• Anyone who is unable to consent or document written consent in English • Anyone confirmed or who could possibly be pregnant • Anyone with an allergy or intolerance to acetaminophen • Anyone with known active liver disease
Compensation Your participation in this study is entirely voluntary. No monetary compensation for participation in this study has been set aside. You are free to contact Dr. Kong if you have questions and problems during the course of participation in this study. She can be reach 24-hours per day at (925) 922-2560. Alternatives Alternatives to the ActiPatch for the treatment muscle pain include anti-inflammatory and pain medications, over-the-counter menstrual relief medications, and topical heat therapies. Benefits The following are the direct and indirect benefits which you may derive from participation in this study: reduced pain, a reduced feeling of swelling, and a reduced need for oral medications. Confidentiality Your records will be held confidential by all parties involved in this research study and you will not be identified in any publication. However, the Food and Drug Administration has the right to access your medical/research records and identity, and may have the need to release this information. In addition, personal information may be disclosed if required by state or federal law. You have a right to privacy. This means all information obtained as a part of this study will only be used as described above. The results of this study may be published in a scientific book or journal. If this is done, your name will not be used without your specific written permission. In addition, if photographs, audiotapes or videotapes are taken during the study, then you must give special written permission for their use. All information about you from this research project will be kept in a locked space. The following people will have access to the study records: Study physician
Company Sponsor RCRC Independent Review Board (IRB) RCRC and accrediting agencies may inspect and copier records, which may have your name on them. Therefore, your total privacy cannot be guaranteed. Participation Your being in this study is voluntary. You may refuse to be in the study without penalty to you or without loss of any treatment rights. You may also leave the study at any time without penalty or loss of benefits. New Findings You will be told of anything new learned during this study which could affect your willingness to continue being in the study. Your physician or the sponsor has the right to terminate the study based on this information. Whom to contact with Questions You have a right to have all questions about the study answered in a way that you clearly understand the answer. Answers to questions, concerns or complaints about this research study, or to report a research related injury, or for information about study procedures please contact Dr. Kong at the below listed number. If you require any medical attention please go to the nearest emergency room. You may contact RCRC if you:
• Would like to speak with someone not related to the research, • Have questions concerns or complaints regarding the research study, or • A question about your rights and welfare as a research participant.
Chairman, RCRC Independent Review Board 2111 West Braker Lane, Suite 400 Austin, TX 78758 or you may e-mail [email protected] or you may call: 888-200-5820 between 8 a.m. and 5 p.m. Central Time RCRC has approved the study and this informed consent document. RCRC is a group of scientific and nonscientific people who review, and approve or disapprove research involving people by following the federal regulations. This group is also required by the federal regulations to do periodic review of ongoing research studies.
Leaving the Study
Taking part in the study is your choice. You may choose either to take part or not take part in the study. You have the right to leave the study at any time. If you do not want to be in the study, there will be no penalty to you, and you will not lose any benefits to which you or otherwise entitled. If you wish to leave the study please contact the study doctor at the number listed on the first page of this consent document to schedule study exit procedures. Your part in the study may be stopped at any time without you being passed. The following people can stop the study at any time - your study doctor, RCRC independent review board, The US FDA, US Department of Health and Human Services, or the sponsor company. Agreement to be in the Study
This consent document contains important information to help you decide if you want to be in the study. If you have questions that are not answered in this consent document, please ask the person explaining this document. By consenting to anticipate you agree that you have been given a copy of all pages of this consent document. You have an opportunity to ask questions and receive satisfactory answers to all your questions about the study. You understand that you're free to leave a study at any time without having to give a reason and without affecting your medical care. You understand that your study related medical records may be reviewed by the Company sponsor the study or by government authorities. If you do not agree with the statement above, you should not sign this and formed consent document
If you have any questions, you may contact Dr. Sheena Kong. I understand and am satisfied with the above information, and I acknowledge having received a copy of this consent form. __________________________________________
__________________________________________
Person Explaining Consent Document - Printed Name and Signature Date
FUNDACIÓN HONDUREÑA DE INVESTIGACIÓN AGRÍCOLA CACAOTEROS ANALIZAN LOS SERVICIOS AMBIENTALES DEL CACAO EN HONDURAS El Proyecto Cacao Centroamérica (PCC) ejecutado envarios países de la región centroamericana por el Cen-tro Agronómico Tropical de Investigación y Enseñanza(CATIE) en coordinación con instituciones locales, realizó enlas instalaciones de la FHIA, La Lima,
Molecular mechanisms that could contribute to prolonged effectiveness of PDE5 inhibitors to improve erectile function Int J Impot Res 2008;20:333–342; DOI:10.1038/ijir.2008.4; Department of Molecular Physiology and Biophysics, Vanderbilt University School of Medicine, Nashvil e, TN, Correspondence to: Professor SH Francis, Department of Molecular Physiology and Biophysics, Vanderbilt
 Data was collected from the participants approximately 48 hours after the administration of the DOMS inducing resistance exercise regiment using a VAS (Visual Analogue Score) pain assessment.
Data were collected at the end of the study. The monitor copied the data from the individual sheets and placed in a spread sheet with one entry per participant depending on the participant’s particular group, i.e., Tylenol, Control or Actipatch. Thus there were three columns, one for each group. At the end of the study, the data were provided for analysis. The data were analyzed using Excel macro’s. Means, variances and standard deviations for the VAS scores were calculated for each subsample. The difference between cell means was tested using t-tests using with the following formula:
where X is the mean for the group, VAR is the variance of the observations, n is the sample size and the subscripts T and C represent the two different groups being compared, e.g. “treatment” and “control” group.
This study used two tailed tests and significance levels of .05, .025 and .001 to determine the significantsignificance differences in sample means.
102 patients were enrolled in this study, 38 using the Actipatch, 38 acting as control, and 26 using Tylenol. Table 1 shows the mean VAS scores for each subsample along with the variances for these means, i.e., var/n .
Table 2 presents the results of the individual t-tests. Comparisons were made between Actipatch and the control group and Actipatch and the Tylenol group. The former comparison was significant at the .001 level; the latter was significant at the .05 level.
The data from this study demonstrated demonstrates that the ActiPatch device manufactured by BioElectronics Corporation. had a significant effect on reducing DOMS DOMS-related symptoms of muscle pain and soreness when compared to both a control group that received no treatment and a group that was treated with 1 gram of acetaminophen in the form of Extra Strength Tylenol. Based on this data, the principal investigator concludes that ActiPatch is safe and effective treatment for DOMS. The use of ActiPatch seems to be a convenient, safe and effective new treatment for muscle pain and soreness, especially when compared to currently FDA approved over the counter treatments, such as acetaminophen, NSAIDs and other pain medications that may have questionable safety profiles for many people.
Delayed Onset Muscle Soreness (DOMS) is a condition associated with increased physical exertion.
Data was collected from the participants approximately 48 hours after the administration of the DOMS inducing resistance exercise regiment using a VAS (Visual Analogue Score) pain assessment.
Data were collected at the end of the study. The monitor copied the data from the individual sheets and placed in a spread sheet with one entry per participant depending on the participant’s particular group, i.e., Tylenol, Control or Actipatch. Thus there were three columns, one for each group. At the end of the study, the data were provided for analysis. The data were analyzed using Excel macro’s. Means, variances and standard deviations for the VAS scores were calculated for each subsample. The difference between cell means was tested using t-tests using with the following formula:
where X is the mean for the group, VAR is the variance of the observations, n is the sample size and the subscripts T and C represent the two different groups being compared, e.g. “treatment” and “control” group.
This study used two tailed tests and significance levels of .05, .025 and .001 to determine the significantsignificance differences in sample means.
102 patients were enrolled in this study, 38 using the Actipatch, 38 acting as control, and 26 using Tylenol. Table 1 shows the mean VAS scores for each subsample along with the variances for these means, i.e., var/n .
Table 2 presents the results of the individual t-tests. Comparisons were made between Actipatch and the control group and Actipatch and the Tylenol group. The former comparison was significant at the .001 level; the latter was significant at the .05 level.
The data from this study demonstrated demonstrates that the ActiPatch device manufactured by BioElectronics Corporation. had a significant effect on reducing DOMS DOMS-related symptoms of muscle pain and soreness when compared to both a control group that received no treatment and a group that was treated with 1 gram of acetaminophen in the form of Extra Strength Tylenol. Based on this data, the principal investigator concludes that ActiPatch is safe and effective treatment for DOMS. The use of ActiPatch seems to be a convenient, safe and effective new treatment for muscle pain and soreness, especially when compared to currently FDA approved over the counter treatments, such as acetaminophen, NSAIDs and other pain medications that may have questionable safety profiles for many people.
Delayed Onset Muscle Soreness (DOMS) is a condition associated with increased physical exertion.