Levitra has a minimal amount of contraindications which has increased its popularity kamagra uk You can buy quality certified medications from us at an affordable price.
Newsletter
Vol. 3 No.2 R e c o v e r y S t r a t e g i e s f r o m t h e O R t o H o m e The Challenges of
In 2000, the American Cancer Society estimated
that head and neck cancers accounted for 2.5%of cancer diagnoses with concomitant high mor-
Postoperative
tality rate —2% of all cancer deaths. There are,
however, indications that the rates of newly di-agnosed oral cancers have declined and the mor-
Radiotherapy for Bonus Issue
tality rates for oral cavity and oropharyngeal can-
1.6 C
cers have been decreasing since the early 1980s. Es
The treatment plan for these patients is individu-
Post-surgical Head and
alized and depends on a number of variables. The treatment may be surgery alone, radiationalone, or a combination of both. In general, head
Neck Cancer Patients
and neck cancers when treated early are highly By Margaret Hickey RN, MSN, MS, OCN, CORLN
curable with radiation or surgery alone. Advancedcancers are candidates for treatment by a com-bination of surgery and radiation therapy.
Patients with more advanced cancers or in situ-ations where it was not possible to resect thelesion with adequate surgical margins will re-quire postoperative radiation therapy. In this ar-ticle, Ms. Hickey discusses the complex patientcare issues surrounding treatment of patients re-quiring postoperative external beam radio-therapy.
Head and neck cancer accounts these cancers rises. This ratio of men to
Successful management demands the attention
of a dedicated health-care team: radiation on-
many to be the most dreaded site for can-
vidualized for these patients with special
cologist, otolaryngologist, radiation oncologynurse, radiation therapist, social worker and di-
cer to occur, as both the disease and treat-
size and location, patient’s physical condi-
cers of the head and neck can arise in the
tion, patient’s emotional status, treating
Advisory Board
oral cavity, pharynx, or larynx. In 2000, the
team’s experience, and available treatment
Oncology Nurse Specialist, Oncology Memorial Hospital, Houston, TX,Adjunct Faculty, Trinity College of Nursing, Moline, IL
cancers are treated early (stage I and II),
Pulmonary Staff Nurse, Genesis Medical Center, Davenport, IA
they are highly curable with radiation or
Asst. Professor for Adult Acute and Critical Care NursingSecretary/Treasurer, AACN Certification Corp.
with the greatest risk are men over 40 years
Nurse Practitioner/Specialist, Associate Professor of Nursing,
by a combination of surgery and radiation. Clinical Assistant Professor of Urology, University of Virginia,Department of Urology, Charlottesville, VA, Past-president SUNA
because a history of excessive use of to-
Victoria-Base Smith, PhD, MSN, CRNA, CCRN
bacco and alcohol are contributing factors
Clinical Assistant Professor, Nurse Anesthesia,
to the development of this cancer. In the
this group of patients, they should be con-
Nurse Practitioner, Vascular Surgery, Harper Hospital, Detroit, MIVice-president, Education and Professional Development,
or in situations where it was not possible
Executive Director, Cross Country UniversitySupported by an educational grant from Dale Medical Products Inc.
Table 1: A guide to assessment of the oral cavity Category Adapted from Beck SL, Yasko JM: Guidelines for Oral Care. 2nd ed. Crystal lake, IL;Sage,1993.
to resect the lesion with adequate surgi-
treatment. The cancer, surgical resection,
cal margins will require postoperative ra-
and cytotoxic effects of radiation therapy
diation. This article will discuss the com-
plex patient-care issues surrounding treat-
in saliva production, xerostomia, another
side effect of head and neck radiation to
be discussed later in this paper, exacer-bates mucositis by causing changes to the
Radiotherapy
therapy, particularly antimetabolites such
death by eliminating the proliferation of
adjuvant therapies for head and neck can-
cer, heightens the risk of oral complica-
it together. The cells are able to function
eliminate their prior albeit unhealthy cop-
Stomatitis is one of the earliest side ef-
fects to manifest and may initially present
directly related to the rate at which cells
from 1 to 3 weeks into therapy. Early signs
divide. This holds true for both tumor cells
and normal cells. Injury occurs in normal
tissues with rapid cell proliferation, such
the stomatitis advances, ulcerative lesions
do not.2 And, the risk of a second tumor is
has significant side effects, both acute and
Mucositis
begin an aggressive, prophylactic oral regi-
the treatment site, dose, and patient’s re-
care is essential during therapy to improve
sponse. Acute side effects include mucosi-
tis or stomatitis is an inflammatory reac-
tis, xerostomia, taste changes, skin reac-
mucositis. A dental evaluation and correc-
tiple stressors, including cancer and its
tion of any periodontal and dental disease
patient has dentures, they must fit prop-
rinses should be increased to every 2 hours
flossing if pain, thrombocytopenia (plate-
they irritate the mucosa and will exacer-
are present. The soft toothbrush may need
plenty of fluids to hydrate the mucosa.
Trauma to the oral cavity should be mini-
mized; this goal can be achieved by avoid-
need to be used, especially before eating.
ing foods that are too hot or cold, spicy or
Topical analgesics include sprays, gels, and
(Hurricaine®, Zilactin-B®, Orajel®). These Figure 1
done with each patient, using an oral mu-
analgesics can be used alone or mixed with
cositis grading system (Table 1). The pa-
tient should be instructed to implement a
equal proportions of xylocaine viscous 2%, the radiation field, a mucositis of the tra-
diphenhydramine elixir, and an antacid; chea or tracheitis may result. The tracheal
15 cc are administered every 2 to 4 hours mucosa becomes inflamed, some blood
streaking of the sputum may be noted, and
A number of topical agents can be used there is a risk of infection. It can best be
to protect the mucosa and to promote heal- prevented and managed by maintaining
■ brushing four times daily, 30 minutes
ing. A sucralfate (carafate) suspension can adequate humidification. The patient can
after eating and at bedtime, with a soft,
also be used. The sucralfate adheres to and use a number of techniques to increase
protects exposed proteins in the inflamed humidification. They include instilling ster-
ile normal saline (1 to 2 cc) into the stoma,
■ removing and thoroughly cleaning den-
three to four times a day; wearing a moist-
ened stomal cover; using a bedside humidi-
fier; and increasing fluid intake. Trauma
■ moistening the lips with a lip balm of
spoons of salt or 1 teaspoon of baking soda,
changes. If the patient has had a total la-
or both. Oral rinses, such as chlorhexidien
ryngectomy, the tube should coated with a
mucosa and may stimulate prostaglandin water-soluble lubricant, and an obturator
release.6,7 Orabase, a paste of carboxy- should be used when the tube is re-in-
washes are to be avoided, as most contain
methylcellulose, can be applied to the ir- serted after cleaning or no laryngectomy
alcohol and, although initially refreshing,
ritated areas but should not be used if an tube should be used at all. Whenever a tra-
infection is present. Zilactin®, a cheostomy or laryngectomy tube is used,
At the first sign of stomatitis, increase
hydoxypropylcellulose gel, forms a protec- it is vital that the tube is well secured. Cot-
the frequency of oral rinses with the solu-
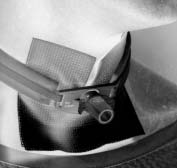
tive film that can last up to 8 hours. Vita- ton-twill tracheostomy tape or a manufac-
min E oil extracted from a 400-mg cap- tured tracheostomy tube holder (Dale
sule can be applied with a cotton-tip ap- Medical) can be used (Figure 1). The tra-
plicator to oral lesions. If the oral cavity cheostomy tube holder contains an elastic
the first sign of inflammation to prevent a
needs debrided, a 1:4 hydrogen peroxide section that enables movement and accom-
secondary fungal infection. Fungal infec-
and water solution can be used; however, modates the cough reflex, while holding
it should be discontinued when ulcers are the tube secure.
debrided, as prolonged use can inhibit tis-
may be delayed if a fungal infection is as-
Table 2: Radiation Therapy Oncology Group radiation morbidity scoring
sociated with the mucositis, but generally
criteria: salivary gland Acute Reactions Xerostomia
Mild mouth dryness/ slightly thickened saliva/ may have slightly altered taste, such asmetallic taste/ changes are not reflected by alteration in baseline feeding
minor salivary glands. It is a natural lubri-
Moderate to complete dryness/ thick, sticky saliva/ markedly altered taste
in saliva begin the digestive process. Sa-
Late Reactions
debris and bacteria, aids in taste, and is
Slight dryness of mouth / good response on stimulation
important for speech. Salivary glands pro-duce 1,000 to 1,500 ml of saliva each day.8
Moderate dryness of mouth / poor response on stimulation
Complete dryness of mouth / no response on stimulation
sult from radiation therapy to the head and
neck region, certain chemotherapy agents,
Source: Radiation Therapy Oncology Group (RTOG), American College of Radiology, Philadelphia, PA
and surgery that involves removal of sali-vary gland(s). Radiotherapy-induced xe-
maintain nutrition. The sensation of dry-
rostomia results from radiation damage to
ness is best alleviated with frequent oral
the salivary glands. As radiation exposure
equate oral care exacerbate the threat of
rinses and sips of water or juice. Meticu-
rostomia is noted. If the radiation dose ex-
be initiated at the start of therapy as de-
they will not recover.9 Some patients re-
help to relieve symptoms temporarily. En-
sleeping, speaking, and the ability to per-
courage the patient to increase oral intake
form physical exercise. There is a lack of
tients’ ability to compensate for the sali-
ropey, which makes it difficult to eat dry
vary changes.10 Rating scales can be used
such as Salivart® or MouthKote®. They are
to describe the degree of xerostomia. The
the need to take frequent sips of fluids,
which may result in early satiety. Oral dry-
than water alone. The use of sugarless gum
ness alters the taste of food and smell. This
help to increase the salivary flow. Sleep
tive impact on the patient’s nutritional sta-
tus. Saliva is also important for retention
affect oral comfort, mucosal health, den-
and stability of dentures. Sleep is inter-
the mouth with a teaspoon of olive oil or
tition, deglutition, the ability to chew nor-
mally, and the ability to speak. The patient
that the tongue is stuck to the roof of the
lematic, especially at mealtime. Papain is
tions, sore lip and tongue, ulcerations, ill-
tions are impaired by the need to take sips
fitting dentures, difficulty swallowing, and
to dissolve tenacious secretions. The pa-
abnormalities of taste and smell. Xerosto-
der to articulate clearly; this necessity is
tient may find some relief by eating papa-
mia affects oral health, as it contributes
to the development of dental caries, loss
of teeth, mucositis, oral infections, and os-
solution of meat tenderizer and water can
teonecrosis. The patient is often instructed
tended to provide comfort, to prevent and
to use fluoride trays daily during treatment
minimize stomatitis/oral infections, and to
to help to dissolve the thick secretions.
tual or potential malnutrition. A lack of
nutrition, and xerostomia interferes with
oral intake should be anticipated. At the
this goal. The lack of saliva interferes with
chewing, digestion, and taste. Changes in
ter therapy begins and continue for 14 to
21 days after its completion. Partial re-
high-protein diets, oral supplements, food
maintain nutrition. Soft, moist foods are
ment; a complete recovery of normal taste
preparation tips, and other suggestions to
easier to eat. The use of gravies and sauces
stimulate appetite. Despite this counsel-
ing, patients may require the insertion of
make it easier to chew and swallow. Avoid
a feeding tube to maintain nutrition; it is
dry, sticky foods like peanut butter. Alco-
preferable to use the gastrointestinal tract
and place a percutaneous gastric tube. The
be avoided, as they further dry and irri-
application of a G-tube holder will lower
tube profile and help to discourage patient
“pull-out.” It allows the patient to be more
comfort and irritation caused by adhesive
important for supportive care, as they di-
treating anorexia and cachexia, related to
can be used to stimulate salivary flow.
perience taste changes resulting from sur-
Amifostine (Ethyol®) is a radioprotective
gery, chemotherapy, and radiotherapy.
can be used to stimulate appetite include
Surgery to the oral cavity and tongue lead
mize the occurrence of acute and late xe-
to a loss of sweet and salty receptors; pro-
foods, small frequent meals, eliminate any
rostomia, mucositis, and loss of taste.
cedures involving the palate lead to a loss
unpleasant odors or add pleasant ones, use
of sour and bitter receptors. Patients with
Taste changes
exercise. To counteract changes to taste,
altered olfactory component to taste, re-
mary sensations: sweet, sour, bitter, and
sulting from the diversion of airflow from
salty. Taste buds, the receptors and con-
lemon, and vanilla; avoid using hot spices,
ductors of taste sensation, respond to all
grees. Alterations in taste and smell have
on appetite and contribute to nutritional
well as moisten food. Maintaining the nu-
dependent of treatment for their disease.11
deficits. People with cancer who lose 10%
tritional status improves quality of life and
not live as long as those with similar can-
xerostomia. Taste alterations are believed
Skin reactions
to result from both the loss of saliva and
ished at diagnosis; this physical state is ex-
the direct pathological effect of radiation
affects swallow, taste, and appetite. Now,
radiation dose beneath the skin surface.
the microvilli of the taste buds may be the
as they face radiation and the multiple oral
complications caused by stomatitis, xeros-
tumor bed may be close to or even involve
tomia, and taste changes, maintaining ad-
the skin. Within the irradiated field, the
sweet taste is least affected. This change
skin will react to treatment. Melanocytes
plaint of pain. Topical analgesics should
electrolyte imbalance or dehydration, and
struction exceeds the rate of repair, and
be used, especially before meals. This pain
can be quite severe and chronic. Narcotic
posure of the dermis results. The loss of
analgesics should be used, if warranted.
tance of exercise to alleviate fatigue is an
the dermis are problematic but rarely does
the site become infected. Healing is spon-
Conclusion
fort. Use of long-acting opioids works well
to control the chronic pain of stomatits. A
number of agents are available, including
include the collar line, clavicular area, and
head and neck cancer. Patients experience
changes, skin reactions, pain, and fatigue.
efits to this patient population, because it
clothing on skin within the radiation field.
The tracheal stoma needs to be kept clean
and is effective for 72 hours. As with any
radiation oncologist, otolaryngologist, ra-
and dry. If the patient has a metal tracheo-
pist, social worker, and dietician. The team
ing therapy. If there is a lot of drainage
without the involvement and efforts of the
patient and family. They must be provided
dressing needs to be changed frequently.
plaint of patients with cancer. As many as
tating; it is important to keep them clean
96% of patients report fatigue in conjunc-
and dry and to avoid constriction. A tra-
therapy.14 Like pain, fatigue can only be
measured by the patient’s subjective re-
and has a positive impact on the patient’s
port. Multiple factors contribute to fatigue
ment. These factors either disrupt oxygen
neck cancer patients are “special people.”
twill tape with a built-in elastic section to
nutrition and hydration. Psychological fac-
tors, such as anxiety and depression, also
tial. The irritated skin needs to be treated
of providing nursing care to this popula-
with care. Skin within the radiation field
of patients undergo radiotherapy.15 Treat-
tion is equally special. Mary Jo Dropkin,
ment-related fatigue has a clear temporal
sionally, fatigue persists for a prolonged
horrified, struggling to maintain pressure
on a ruptured carotid artery, and shaving
around a facial defect. It is being there
out discussing them with the radiation or
fatigue is to correct any potential contribu-
for the first look in the mirror after sur-
gery, appreciating laughter without sound,
drugs, treatment of sleep disorders, effec-
around the hall with one so severely dis-
16. Yuska CM. Introduction. Seminars in Oncology
figured that he was afraid to venture out
Cross Country University is an ac-credited provider of continuing edu-
Suggested readings
truly beneficial only after the defect is ac-
1. Fleming ID, Cooper JS, Henson DE, Hutter RVP,
et al. (eds.). AJCC Cancer Staging Handbook.
Philadelphia: Lippincott-Raven Publishers, 1997.
2. Fowler JF, Lindsstrom MJ. Loss of local control with
After reading this educational offering, the reader
neck cancer patient is a direct encounter
prolongation in radiotherapy. International Journal
should be able to:
Review treatment modalities for head and neck cancer.
3. Hansen O, Overgaard J, Hansen HS, Overgaard M,
2. Describe prevention and management of mucositis in
et al. Importance of overall treatment time for the
References
a patient receiving radiation therapy to the head and
outcome of radiotherapy of advanced head and neck
1. American Cancer Society, Cancer Facts and Figures
carcinoma: dependency on tumor differentiation.
3. Discuss the management of xerostomia and its effects
2000, http://www.cancer.org/statistics/cff2000/data/
Radiotherapy and Oncology 1997,43(1):47-51.
on a patient receiving radiation therapy for head and
2. Browman GP, Wong G, Hodson I, Sathya J, Russell
4. Describe the treatment of skin reactions that may
R, McAlpine L, Skingley P, Levine MN. Influence of
cigarette smoking on the efficacy of radiationtherapy in head and neck cancer. New England
5. Describe pain management for the head and neck
Journal of Medicine 1993,328(3):159-163.
3. Spitz MR. Epidemiology and risk factors for head
6. Discuss multidimensional causes and management of
fatigue in patients receiving radiation therapy for head
4. Strohl RA. The etiology and management of acute
To receive continuing education credit, simply do the
and late sequelae of radiation therapy in persons
following:
with head and neck cancers. ORL Head and Neck
ana. Her past experience includes the directorship
2. Complete the post-test for the educational offering.
5. Miller SE. Stomatitis and Esophagitis. In Yasko JM
Mark an X next to the correct answer. (You may make
(ed.). Nursing management of symptoms associated
of Tulane Cancer Centre, Tulane University Hos-
with chemotherapy. 4th edition. Bala Cynwyd,PA:Meniscus Health Care Communications, 1998,
pital and Clinic, New Orleans, and the clinical di-
rectorship of the General Clinical Research Cen-
4. Mail, fax, or send on-line the completed learner
6. Loprinzi CL, Ghosh C, Camoriano J, Sloan J, et al.
evaluation and post-test to the address below.
Phase III controlled evaluation of sucralfate to
ter, University of Pittsburgh Medical Center, Pitts-
5. 1.6 contact hours will be awarded for this educational
alleviate stomatitis in patients receiving fluoruracil-
burgh, Pennsylvania. She is a past-president and
offering through Cross Country University, an accredited
based chemotherapy. Journal of Clinical Oncology
active member of the Society of Otorhinolaryngol-
provider of continuing education in nursing by the
American Nurses Credentialing Center’s Commission on
7. Cengiz M, Ozyar E, Ozturk D, Akyol F, Atahan IL,
Accreditation (ANCC) and an approved CE provider by
Hayran M. Sucralfate in the prevention of radiation-
the American Society of Radiologic Technologists, as it
induced oral mucositis. Journal of Clinical
Perspectives, a quarterly newsletter focusing on post-
6. To earn 1.6 contact hours of continuing education, you
8. Dreizen S, Brown LR, Handler S, Levy BM.
operative recovery strategies, is distributed free-of-
must achieve a score of 75% or more. If you do not pass
Radiation-induced xerostomia in cancer patients:
charge to health professionals. Perspectives is pub-
the test, you may take it again one time.
effect on salivary and serum electrolytes. Cancer
lished by Saxe Healthcare Communications and is
Your results will be sent within four weeks after the form
funded through an education grant from Dale Medi-
9. Dreizen S, Brown LR, Daley TE. Short- and long-
cal Products Inc. The newsletter’s objective is to pro-
term effects of radiation-induced xerostomia in head
8. The administrative fee has been waived through an
vide nurses and other health professionals with timely
and neck cancer patients on salivary flow. Journal of
educational grant from Dale Medical Products, Inc.
and relevant information on postoperative recovery
9. Answer forms must be postmarked by Jan. 7, 2006,
strategies, focusing on the continuum of care from
10. Mossman K, Shatzman A, Chencharick J. Long-
operating room to recovery room, ward, or home.
term effects of radiotherapy on taste and salivary
Name _______________________________________
function in man. International Journal Radiation
The opinions expressed in Perspectives are those of
Credentials ___________________________________
Oncology Biology Physics 1982,8:991-997.
the authors and not necessarily of the editorial staff,
11. DeWys W, Walters K. Abnormalities of taste
Position/title __________________________________
Cross Country University, or Dale Medical Products Inc.
sensations in cancer patients. Cancer 1975,36:1888-
The publisher, Cross Country University and Dale Medi-
Address _____________________________________
cal Corp. disclaim any responsibility or liability for such
City _________________________ State __________
12. Bender C. Taste alterations. In: Yasko JM (ed.).
Zip _________________________________________
Nursing management of symptoms associated with
We welcome opinions and subscription requests
Phone ______________________________________
from our readers. When appropriate, letters to the
Fax _________________________________________
editors will be published in future issues.
License #: ____________________________________
13. Ottery F. Supportive nutrition to prevent cachexia
* Soc. Sec. No. ________________________________
and improve quality of life. Seminars in Oncology1995,22(Suppl. 3):98-111.
E-mail _______________________________________
14. Portenoy RK, Itri LM. Cancer-related fatigue:
Saxe Healthcare Communications
Guidelines for evaluation and management. The
P.O. Box 1282, Burlington, VT 05402 Cross Country University Fax; (802) 872-7558
15. Ream E, Richardson A. From theory to practice:
6551 Park of Commerce Blvd. N.W. [email protected]
Designing interventions to reduce fatigue in patients
Suite 200 Boca Raton, FL 33487-8218 or Fax: (561) 988-6301 www.perspectivesinnursing.org 1. Head and neck cancers occur more 8. Amifostine is a cytotoxic agent which often in individuals who: enhances the cell killing effects of radiation therapy. 5. Tracheitis can be prevented/ minimized with adequate 9. Managing the impact of taste 2. Radiation alone or surgery alone humidification and: alterations on diet due to xerostomia each has a high cure rate in stage I and direct effects of radiation therapy and II head and neck cancers. to the taste buds can be best managed by: 3. Early signs and symptoms of
b. Inserting a central line for total parental
stomatitis include: 6. Xerostomia may not be reversible if radiation dose exceeds 4000 cGy to the salivary glands. 10. Healing of an area of moist 7. Xerostomia profoundly affects: desquamation of the skin within the 4. Patient teaching regarding radiation field is:
a. Eating, sleeping, speaking, and ability to
appropriate preventative dental hygiene for stomatitis includes:
b. Eating, speaking, hearing, and ability to
weeks after radiation treatment iscompleted
Oral self exam ii. Rinsing with Listerine four times
c. Eating, sleeping, speaking, and ability to
iii. Brushing after eating and at
c. Frequently treated by skin grafts after
bedtime with a soft toothbrush iv. Avoid flossing Apply lip balm to keep lips moist Mark your answers with an X in the box next to the correct answer Participant’s Evaluation
1. What is the highest degree you have earned?
Using 1 =Strongly disagree to 6= Strongly agree rating scale, please circle the number that best reflects the extent of your agreement to each statement. Strongly Disagree Strongly Agree
2. Indicate to what degree you met the objectives for this program:
Review treatment modalities for head and neck cancer.
Describe prevention and management of mucositis in a patient receiving radiationtherapy to the head and neck region.
Discuss the management of xerostomia and its affects on a patient receivingradiation therapy for head and neck cancer.
Describe the treatment of skin reactions that may occur with head and neckradiation.
Describe pain management for the head and neck cancer patient.
Discuss multidimensional causes and management of fatigue in patients receivingradiation therapy for head and neck cancer.
3. Have you used home study in the past? ■ Yes ■ No4. How many home-study courses do you typically use per year?
5. What is your preferred format? ■ video ■ audio-cassette
6. What other areas would you like to cover through home study?
Mail to: Cross Country University, 6551 Park of Commerce Blvd. N.W., Suite 200, Boca Raton, FL 33487-8218• or Fax: (561) 988-6301
Supported by an educational grant from Dale Medical Products Inc.
Detail-Document #200509 −This Detail-Document accompanies the related article published in− PHARMACIST’S LETTER / PRESCRIBER’S LETTER Drug-Induced Photosensitivity Lead author: Kelly M. Shields, Pharm.D. Drugs Reported to Cause Photosensitivity Reactions 1-11 Therapeutic Class Comments ( Zyrtec ), cyproheptadine ( Periactin ), diphenhydramine ( Benadryl ),
Links to Contents: Membership of professional organisations and societies Senate of Dental Specialties Formerly member on behalf of the British Society of Periodontology British Society of Periodontology 2001-2002: Scientific advisor to the president, Professor Francis Hughes European Association of Osseointegration Fellow of the International College of Dentists Senior Memb
 patient has dentures, they must fit prop-
rinses should be increased to every 2 hours
flossing if pain, thrombocytopenia (plate-
they irritate the mucosa and will exacer-
are present. The soft toothbrush may need
plenty of fluids to hydrate the mucosa.
patient has dentures, they must fit prop-
rinses should be increased to every 2 hours
flossing if pain, thrombocytopenia (plate-
they irritate the mucosa and will exacer-
are present. The soft toothbrush may need
plenty of fluids to hydrate the mucosa. 16. Yuska CM. Introduction. Seminars in Oncology
figured that he was afraid to venture out
Cross Country University is an ac-credited provider of continuing edu-
Suggested readings
16. Yuska CM. Introduction. Seminars in Oncology
figured that he was afraid to venture out
Cross Country University is an ac-credited provider of continuing edu-
Suggested readings