Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Dfhcc.harvard.edu
⅐ N U M B E R 2 8 ⅐ O C T O B E R 1 2 0 0 5
Phase I Study of Gefitinib Plus Celecoxib in Recurrentor Metastatic Squamous Cell Carcinoma of the Headand NeckLori J. Wirth, Robert I. Haddad, Neal I. Lindeman, Xiaojun Zhao, Jeffrey C. Lee, Victoria A. Joshi,Charles M. Norris Jr, and Marshall R. Posner
Effective and tolerable palliative treatments are needed for patients with incurable squamous
cell carcinoma of the head and neck (SCCHN). Single-agent targeted therapies have limitedactivity in this setting. The feasibility of adding celecoxib to gefitinib for the treatment of
Patients and Methods Nineteen patients with unresectable recurrent locoregional and/or distant metastatic SCCHN
with progressive disease after at least one prior chemotherapy or chemoradiotherapy
regimen were enrolled onto this single-institution phase I study. Three dose levels were
explored: (1) celecoxib 200 mg twice daily plus gefitinib 250 mg daily; (2) celecoxib 400
mg twice daily plus gefitinib 250 mg daily; and (3) celecoxib 400 mg twice daily plus
No dose-limiting toxicities were encountered at any dose level. The most common toxicitieswere acneiform rash, diarrhea, hand reaction, dyspepsia, and anemia. Four of 18 patientsassessable for response (22%; 95% CI, 2% to 42%) achieved a confirmed partial response. Conclusion The combination of gefitinib 500 mg daily plus celecoxib 400 mg twice daily is well-tolerated. The encouraging responses seen in this early study suggest further evaluation of epidermal growth factor receptor and cyclooxygenase-2 inhibitors in SCCHN is warranted. J Clin Oncol 23:6976-6981. 2005 by American Society of Clinical Oncology
Results program showed that 5-year survival
INTRODUCTION
of patients with oral cavity and pharyngeal
(P Ͻ .05).1 Still, as these statistics imply,
approaches, approximately 40% of patients
years, major advances in surgical, radia-
able disease at some point in the course of
vances are finally becoming apparent in sur-
vival statistics. For example, for the periods
current SCCHN is, whenever feasible, sal-
from 1974 to 1976, and from 1995 to 2000,
vage surgery or radiation-based therapy. In
data from the National Health Statistics and
patients for whom a salvage approach is not
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Gefitinib ؉ Celecoxib for SCCHN
disease, palliative systemic therapy is the only option. Both
We therefore undertook this phase I study to establish
combination and single agent chemotherapy regimens have
the appropriate dosing and safety profile of gefitinib plus
demonstrated moderate response rates in this setting of ap-
the COX-2 inhibitor, celecoxib, in subjects with incurable
proximately 30% to 40%, yet the duration of response is often
SCCHN, as a first step to exploring the combined targeting
brief, and median survival is short, typically 6 to 9 months.2
Recently, targeted therapies have been explored in at-
tempts to improve on the poor outcomes in incurable
PATIENTS AND METHODS
SCCHN. To date, drugs targeting the epidermal growthfactor receptor (EGFR) have experienced the most clini-
Patients
cal development. EGFR is overexpressed in the majority
Between May 2003 and April 2004, 19 patients with incurable
of SCCHNs, and this overexpression correlates with poor
SCCHN were enrolled onto this phase I study at Dana-Farber
prognosis.3 This, coupled with the understanding of the down-
Cancer Institute and Massachusetts General Hospital. The proto-
stream consequences of EGFR signaling, including cell prolif-
col was approved by the Dana-Farber/Harvard Cancer Center
eration, suppression of apoptosis, and tumor angiogenesis, has
Office for the Protection of Research Subjects. Eligibility criteria
made EGFR an appealing target in SCCHN.4,5 EGFR inhibi-
included unresectable recurrent locoregional and/or distant met-
tors that have undergone the most clinical development in
astatic SCCHN, with progressive disease after at least one priorchemotherapy or chemoradiotherapy regimen. Subjects also were
SCCHN are the monoclonal antibody, cetuximab, and the
required to have assessable disease; life expectancy Ն 4 months;
small molecule tyrosine kinase inhibitors (TKIs), gefitinib and
Eastern Cooperative Group performance status of Յ 2; adequate
erlotinib. As single agents, EGFR inhibitors are well tolerated,
hematologic, renal, and liver function; use of sufficient birth con-
but thus far, they have shown only modest activity against
trol in women of childbearing potential; and signed informed
SCCHN, with estimated response rates ranging from 3.5%
consent. Exclusion criteria included hypersensitivity to celecoxib,
with gefitinib at 250 mg daily, and 10.6% at 500 mg daily, to
aspirin, or other nonsteroidal anti-inflammatory drugs (NSAIDs);
11% to 14% with cetuximab administered weekly.6-9
significant comorbidities (including coronary artery disease,symptomatic congestive heart failure, active alcohol abuse, bleed-
One strategy to enhance the efficacy of anti-EGFR ther-
ing diathesis, history of interstitial lung disease or gastrointestinal
apy while maintaining tolerability is to add in another tar-
ulcer within 12 months); other malignancy except basal cell skin
geted therapy with nonoverlapping toxicity. As with EGFR,
carcinoma or cervical carcinoma-in-situ; concomitant use of phe-
cyclooxygenase-2 (COX-2) is overexpressed in SCCHN,
nytoin, carbamazepine, barbiturates, rifampin, phenobarbital, St
and its expression correlates with poor prognosis.10 COX-2
John’s Wort, aspirin at a dose of 325 mg daily or higher, NSAIDs,
is an inducible enzyme that results in an array of down-
rofecoxib, or other COX-2 inhibitors; or systemically absorbed
stream events, including suppression of apoptosis and acti-
steroids, surgery, or radiotherapy within 30 days; pregnancy; orbreast-feeding.
vation of proliferation and angiogenesis. Of note, there isinteraction between EGFR and COX-2 signaling pathways
Dose Levels and Treatment
at several levels. For example, EGFR and COX-2 both signal
Table 1 illustrates study dose levels. Celecoxib was adminis-
through the ras/MAPK and PI3K/Akt pathways.11 Crosstalk
tered at 200 mg by mouth twice daily, with gefitinib 250 mg bymouth once daily in dose level 1. Subjects unable to take medica-
between EGFR and COX-2 has also been demonstrated at
tions by mouth were administered both drugs by gastric tube.
the level of activation. That is, EGFR-mediated MAPK ac-
Dose level 2 consisted of celecoxib 400 mg twice daily plus
tivity can induce COX-2 expression.12 In turn, COX-2, via
gefitinib 250 mg/d. Dose level 3 consisted of celecoxib 400 mg
its primary mediator, PGE2, can activate the cyclic AMP/
twice daily plus gefitinib 500 mg/d. One cycle equaled 28 days of
protein kinase A pathway to promote the expression am-
phiregulin, one of several EGFR ligands.13 The potential for
Nonhematologic dose-limiting toxicity (DLT) was defined as
enhanced activity of combining EGFR and COX-2 block-
National Cancer Institute Common Toxicity Criteria (CTC), ver-sion 2.0 grade 4 skin rash occurring in cycle 1 of treatment, grade
ade, as suggested by these interactions, has been confirmed
Ն 3 skin rash on reduced doses of gefitinib, grade Ն 3 diarrhea on
in preclinical combination studies of EGFR TKIs plus
reduced doses of gefitinib, grade 4 diarrhea with hemodynamic
COX-2 inhibitors. One such study showed that combined
collapse, grade Ն 3 gastritis or gastric ulcer on reduced doses of
therapy inhibited growth in at least an additive fashion infive SCCHN cell lines.14 In vivo, combination therapy hasbeen tested in the intestinal neoplasia APCMin/ϩ mouse model. EGFR was targeted with the TKI EKI-569, and COX-2 was
Table 1. Dose Levels
inhibited by the nonsteroidal anti-inflammatory drug, sulin-
dac. Alone, these agents reduced polyp formation by 87% and
70%, respectively, whereas combined treatment yielded a
greater than 95% reduction in polyps, suggesting that this
combination has more potent antiproliferative activity than
Abbreviations: QD, daily; bid, twice daily.
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Wirth et al
gefitinib and/or celecoxib, grade Ն 3 gastrointestinal hemorrhage,
icine of the Harvard Medical School/Partners Healthcare Cen-
grade Ն 3 allergic reaction, grade Ն 3 pneumonitis, or other grade
ter for Genetics and Genomics (CLIA# 22D1005307). EGFR
Ն 3 nonhematologic toxicity on reduced doses of gefitinib and/or
and KRAS amplification was investigated by quantitative real-
celecoxib. Hematologic DLT was defined as “clinically relevant
time PCR performed on a PRISM 7700 sequences detector
CTC grade Ն 3 hematologic toxicity” (ie, absolute neutrophil
(Applied Biosystems, Foster City, CA), using a QuantiTect
count Ͻ 1.0 ϫ 109/L) for more than 7 days, fever (Ͼ 38.5°C) with
SYBR Green kit (Qiagen Inc, Valencia, CA). The standard curve
neutropenia, platelet count less than 50 ϫ 109/L, and/or grade 4
method was used to calculate target gene copy number. PCR
anemia. Three patients were enrolled at each dose level. Enroll-
sequences for each target used are as previously described.19
ment proceeded to the next dose level after all three patients were
PCR reactions were performed at least in duplicate, and means
treated for Ն 4 weeks and safety data were reviewed. If no DLTs
are reported. Amplification ratios Ն 2.0 were considered indic-
occurred, the next dose level was opened. If one DLT occurred,
three additional patients were enrolled at the current dose level. Ifno additional DLT occurred, enrollment continued at the nextlevel. If an additional DLT occurred (ie, two or more DLTs per six
patients), then the previous dose level would be declared themaximum tolerated dose (MTD). If two DLTs occurred, no fur-
Patient Characteristics
ther dose escalation would be done, and the previous dose level
Nineteen patients were enrolled on study (Table 2).
would be declared the MTD. If the MTD would not be reached
The median age was 55 years (range, 26 to 68 years). Nine
because one or zero DLTs were encountered at dose level 3, thisdose would be considered the maximum dose, and 10 additional
patients (47%) had recurrent unresectable locoregional
patients would be enrolled at this dose or the MTD to gain addi-
SCCHN, five (26%) had distant metastatic SCCHN, and
tional experience with this regimen.
five (26%) had both locoregional and distant metastatic
Tumor assessment for response took place at the end of every
disease. All patients had received at least one prior chemo-
two cycles (ie, 8 weeks) of therapy. In patients completing six
therapy or chemoradiotherapy regimen. Eight patients
cycles of therapy, the evaluation for response was performed after
started on study at the time of relapsed disease following
every third cycle. Response was assessed radiographically accord-
definitive chemoradiotherapy, two patients were enrolled
ing to Response Evaluation Criteria in Solid Tumors (RECIST)and by physical examination including fiberoptic endoscopy of the
after progressive disease following reirradiation with con-
head and neck. Patients with stable disease or better, continuedtreatment with gefitinib and celecoxib until progressive disease orunacceptable toxicity. Progression-free survival (PFS) and overallsurvival (OS) were estimated by the Kaplan-Meier method from
Table 2. Patient Characteristics
the start of therapy until, respectively, disease progression, and
Assessment of Potential Biomarker Predictors of Response
All available formalin-fixed paraffin-embedded patient tissue
samples were evaluated for tumor content by available hematox-
ylin and eosin–stained slides. Tumor was dissected from normal-
appearing tissue by manual microdissection, and DNA extracted.
Exons 18 to 24 of EGFR were evaluated for mutations by amplifi-
cation using nested primers. Polymerase chain reaction (PCR)
products were then sequenced in both sense and antisense direc-
tions as previously described.16,17 Exons 2 and 3 of KRAS were
amplified in a set of individual nested PCR reactions. The primers
used in the external PCR amplification were as follows: exon 2
forward: 5Ј CTTAAGCGTCGATGGAGGAG; exon 2 reverse: 5Ј
CCCTGACATACTCCCAAGGA; exon 3 forward: 5Ј TGGGTAT-
GTGGTAGCATCTCA; exon 3 reverse: 5Ј AATCCCAGCACCAC-
CACTAC. The primers used in the internal PCR amplification
were as follows: exon 2 forward: 5Ј GTGTGACATGTTCTA-
ATATAGTCA, exon 2 reverse: 5Ј GAATGGTCCTGCACCAG-
TAA; exon 3 forward: 5Ј TCAAGTCCTTTGCCCATTTT, exon 3
reverse: 5Ј TGCATGGCATTAGCAAAGAC.18 Universal linker se-
quences were added to the 5Ј ends of the internal primers (forward
5ЈTGTAAAACGACGGCCAGT; reverse 5ЈAACAGCTATGAC-
CATG). PCR products were sequenced bi-directionally by dye-
terminator sequencing using a universal primer. Sequence analysis
was performed by Mutation Surveyor (SoftGenetics, State College,
Abbreviations: ECOG PS, Eastern Cooperative Oncology Group perfor-
PA), and manually by two reviewers. The KRAS exon 2 and 3
mance score; MRND, modified radical neck dissection.
analyses were conducted by the Laboratory for Molecular Med-
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Gefitinib ؉ Celecoxib for SCCHN
current chemotherapy, and nine patients were treated after
seen. Celecoxib was discontinued in one patient due to
progression on palliative chemotherapy following prior de-
allergic drug eruption of grade 2 severity, and in one patient
finitive therapy. Overall, a total of 91 cycles of gefitinib and
due to grade 3 renal insufficiency. Both patients continued
celecoxib were administered, with a median of three cycles
gefitinib alone until disease progression. Other toxicities
per patient. Three patients were treated at dose levels one
encountered were: grade 1 nausea (n ϭ 3), grade 1 vomiting
and two, and 13 patients were treated at dose level three.
(n ϭ 2), paronychia (n ϭ 2), and grade 2 dehydration (n ϭ1). One patient experienced grade 2 seizure (n ϭ 1), which
Toxicities
was thought to be unrelated to treatment. One patient
No DLTs were encountered at any dose level. Adverse
experienced a fatal internal carotid artery hemorrhage after
events deemed at least possibly related to therapy by study
66 weeks of treatment. This event was considered unlikely
investigators are described. The most common toxicities
to be related to treatment and was attributed to progressive
encountered were acneiform rash, diarrhea, hand reaction,
disease. No cases of interstitial lung disease or cardiovascu-
dyspepsia and anemia (Table 3). Ten patients (53%) treated
lar events were encountered, and no dose reductions were
across all three dose levels experienced grade 1 or 2 acne-
required throughout the study period.
iform rash. Two patients (11%), both treated in dose level 3,developed grade 3 acneiform rash. Eleven patients (58%)
Response and Survival
treated across all three dose levels experienced diarrhea.
One patient in dose level 3 was lost to follow-up at 4
One patient in dose level 1 was treated for grade 3 diarrhea
weeks, and was thus not assessable for response. Four of
during cycle 3. The diarrhea resolved after gefitinib was held
eighteen patients (22%; 95% CI, 2% to 42%) achieved a
for 6 days and the patient received intravenous fluids, lop-
confirmed partial response (PR). No complete responses
eramide, atropine sulfate/diphenoxylate hydrochloride,
were seen. Responses were seen in all dose levels. One oc-
and octreotide. All other cases of diarrhea were grade 1 or 2.
curred in dose level 1, two in dose level 2, and one in dose
Six patients (32%) developed grade 1 or 2 hand reaction
level 3. Six patients (33%; 95% CI, 11% to 55%) achieved
(erythema with or without peeling or pain). Four patients
stable disease (SD). The median duration of response was
(21%), one in dose level 1 and three in dose level 3, experi-
19 weeks (range, 16 to 66 weeks), or 4.8 months. The me-
enced grade 1 or 2 dyspepsia. Six patients (32%) experi-
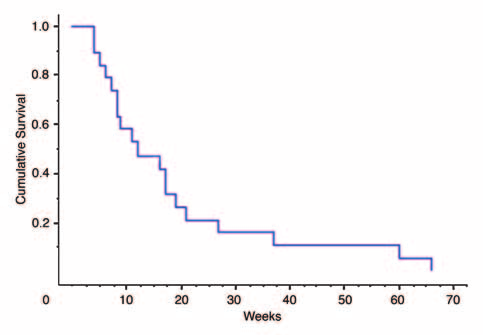
dian PFS and OS times were 12 weeks (range, 4 to 66 weeks)
enced grade 1 anemia: one each in dose levels 1 and 2 and
and 24 weeks (range, 11 to 70 weeks), respectively (Figs 1
four in dose level 3. No other hematologic toxicities were
and 2). Of particular interest were two cases of prolongedtherapy with gefitinib and celecoxib. One patient who washeavily pretreated for multiply recurrent locoregional dis-ease experienced an impressive durable response lasting 66
Table 3. Toxicities Occurring Across All Cycles of Therapy
weeks. Another patient who had numerous lung metastases
following induction chemotherapy and chemoradiother-
Biomarkers Assessment
Formalin-fixed paraffin embedded tumor tissue was
available for 12 of the 19 patients. PCR for EGFR and KRAS
NOTE. Toxicity grades are according to National Cancer Institute Com-
Fig 1. Progression-free survival.
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Wirth et al
patients experienced grade 1 to 2 rash at 500 mg and 250 mgdaily, respectively. No Ն grade 3 rash was seen. In our study,64% of patients had skin rash. Two cases were grade 3, allothers were grade 1 to 2. In the prior studies, diarrheaoccurred in 50% (6% grade 3; all others grade 1-2) and30% (3% grade 3; all others grade 1 to 2) of patients,respectively. With this combination of gefinitib plus cele-coxib, 58% of patients experienced diarrhea (5% grade 3;all others grade 1 to 2). Additional toxicities encounteredwith this combination were occasional dyspepsia, infre-quent allergic drug eruption and renal insufficiency. Therefore, the addition of celecoxib to gefitinib does notseem to affect the degree of gefitinib-specific toxicity, butdoes contribute celecoxib-related toxicities to the side
Fig 2. Overall survival.
effect profile. With the respective overall response ratesof 11% and 4% seen in the prior gefitinib single-agentphase II studies, the response rate of 22% in this study is
failed from two of these 12 specimens. Of the 10 remain-
encouraging, particularly in light of the minor increase in
ing specimens, one came from a patient with a PR to
toxicity that celecoxib adds to gefitinib. Moreover, im-
treatment, four were from patients with SD, and five were
pressive durable responses to gefitinib plus celecoxib can
from patients with PD. No mutations were found in
be seen. While these results must be interpreted cau-
EGFR exons 18 to 24 or KRAS exons 2 and 3. EGFR andKRAS amplification was determined by quantitative PCR
tiously due to the small sample size of 18 patients and
in these 10 specimens. EGFR was not amplified in any
wide 95% confidence intervals, the combination of EGFR
tumor studied, while four of 10 specimens (40%) were
and COX-2 inhibitors for the treatment of SCCHN war-
found to have amplified KRAS with copy numbers rang-
With the small sample size in this study, evaluation of
tumor markers predictive of response was limited. Theseanalyses were even further limited by the success in obtain-
DISCUSSION
ing tumor tissue and DNA from only one patient with aresponse to treatment. Nonetheless, we uncovered no evi-
This study has shown that gefitinib plus celecoxib is a
dence to suggest that factors predictive of response to EGFR
low-toxicity, well-tolerated regimen in patients with in-
TKIs in non–small-cell lung cancer (NSCLC), such as
curable, unresectable previously treated SCCHN. No
mutations in the EGFR tyrosine kinase domain or proto-
DLTs were encountered at any dose level. In SCCHN,
oncogene KRAS involved in signal transduction down-
there is a strong rationale for investigating the 500 mg
stream from EGFR, play a role in SCCHN response to these
dose, given the higher response rate seen with 500 mg in
agents. This is not surprising considering that even though
phase II study compared with that seen with 250 mg.6,7
the response rates of NSCLC and SCCHN to EGFR TKIs are
Further dose escalation of gefitinib beyond 500 mg daily
similar, the nature of response to therapy is quite different.
was, however, not considered in light of data from a large
Most notably, responses to EGFR TKIs in NSCLC are typi-
study in advanced non–small-cell lung cancer random-
cally dramatic and durable over many months.21,22 This is
izing patients between 250 mg and 500 mg that showed
in contrast to the less dramatic responses seen in SCCHN,
no difference between the two doses with respect toresponse, survival or overall symptoms, whereas acne-
lasting a median of 1.6 months with gefitinib alone in
iform rash and diarrhea were both increased with the
Cohen et al, and 4.8 months with gefitinib and celecoxib in
higher dose, suggesting that gefitinib dose escalation of-
this study.7 It is most likely that the different responses to
fers limited benefit.20 Therefore, we conclude that the
EGFR tyrosine kinase inhibition in NSCLC and SCCHN are
recommended dose for future phase II study is gefitinib
a consequence of distinct tissue-specific mechanisms in
500 mg per day plus celecoxib 400 mg twice daily.
these two diseases. That said, one recent study has identified
Prior phase II studies of gefitinib alone at doses of 500
the same E746-A750 deletion mutation in the EGFR ty-
mg and 250 mg daily in a similar pretreated SCCHN popu-
rosine kinase domain that is the most common mutation
lation showed that the principal gefitinib-related toxicities
detected in NSCLC in 3 of 41 (7.3%) SCCHN tumors test-
of rash and diarrhea are comparable to those seen in this
ed.23 Clearly, there is need for confirmation of EGFR mu-
study.6 For example, with gefitinib alone, 48% and 64% of
tations in SCCHN, correlation of mutational status with
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Gefitinib ؉ Celecoxib for SCCHN
response to EGFR TKI therapy and further exploration of
for Genetics and Genomics Laboratory for Molecular Medi-
the biologic mechanisms of EGFR inhibition in SCCHN.
cine and Sequencing Group for their roles in the developmentof the KRAS exon 2 and 3 sequencing assay. Acknowledgment Authors’ Disclosures of Potential
We thank Paul Babb, Kate Montgomery, Baoyan Zhang,
Conflicts of Interest
and the Harvard Medical School/Partners Healthcare Center
The authors indicated no potential conflicts of interest.
(IMC-C225), in combination with cisplatin in pa-
indicators in patients with non-small cell lung
REFERENCES
tients with recurrent squamous cell carcinoma of
cancer treated with chemotherapy alone and in
the head and neck (SCCHN) refractory to cispla-
combination with erlotinib. J Clin Oncol 23:5900-
1. Jemal A, Murray T, Ward E, et al: Cancer
tin containing chemotherapy. Proc Am Soc Clin
statistics, 2005. CA Cancer J Clin 55:10-30, 2005
17. Paez JG, Janne PA, Lee JC, et al: EGFR 2. Cohen EE, Lingen MW, Vokes EE: The 10. Gallo O, Masini E, Bianchi B, et al: Corre-
mutations in lung cancer: Correlation with clinical
expanding role of systemic therapy in head and
lation between cyclooxygenase-2 pathways and
response to gefitinib therapy. Science 304:1497-
neck cancer. J Clin Oncol 22:1743-1752, 2004
tumor angiogenesis in head and neck cancer and
3. Grandis JR, Melhem MF, Gooding WE, et
its prognosistic significance. Neoplasia 3:53-66,
18. Davies H, Bignell GR, Cox C, et al: Muta-
al: Levels of TGF-alpha and EGFR protein in head
tions of the BRAF gene in human cancer. Nature
and neck squamous cell carcinoma and patient
11. Dannenberg AJ, Lippman SM, Mann JR,
survival. J Natl Cancer Inst 90:824-832, 1998
et al: Cyclooxygenase-2 and epidermal growth
19. Zhao X, Li C, Paez JG, et al: An integrated 4. Cohen EE: Novel therapeutic targets in
factor receptor: Pharmacologic targets for che-
view of copy number and allelic alterations in the
squamous cell carcinoma of the head and neck.
moprevention. J Clin Oncol 23:254-266, 2005
cancer genome using single nucleotide polymor-
12. Sheng H, Williams CS, Shao J, et al: Induc-
phism arrays. Cancer Res 64:3060-3071, 2004
5. Pomerantz RG, Grandis JR: The epidermal
tion of cyclooxygenase-2 by activated Ha-ras
20. Kris MG, Natale RB, Herbst RS, et al:
growth factor receptor signaling network in head
oncogene in Rat-1 fibroblasts and the role of
Efficacy of gefitinib, an inhibitor of the epidermal
and neck carcinogenesis and implications for
mitogen-activated protein kinase pathway. J Biol
growth factor receptor tyrosine kinase, in symp-
targeted therapy. Semin Oncol 31:734-743, 2004
tomatic patients with non-small cell lung cancer:
6. Kane MA, Cohen E, List M, et al: Phase II 13. Shao J, Lee SB, Guo H, et al: Prostaglan-
A randomized trial. JAMA 290:2149-2158, 2003
study of 250 mg gefitinib in advanced squamous
din E2 stimulates the growth of colon cancer
21. Pao W, Miller V, Zakowski M, et al: EGF
cell carcinoma of the head and neck (SCCHN).
cells via induction of amphiregulin. Cancer Res
receptor gene mutations are common in lung
cancers from “never smokers” and are associ-
7. Cohen EE, Rosen F, Stadler WM, et al: 14. Chen Z, Zhang X, Li M, et al: Simulta-
ated with sensitivity of tumors to gefitinib and
Phase II trial of ZD1839 in recurrent or metastatic
neously targeting epidermal growth factor recep-
erlotinib. Proc Natl Acad Sci U S A 101:13306-
squamous cell carcinoma of the head and neck.
tor tyrosine kinase and cyclooxygenase-2, an
efficient approach to inhibition of squamous cell
22. Janne PA, Engelman JA, Johnson BE: 8. Baselga J, Pfister D, Cooper MR, et al:
carcinoma of the head and neck. Clin Cancer Res
Epidermal growth factor receptor mutations in
Phase I studies of anti-epidermal growth factor
non-small-cell lung cancer: Implications for treat-
receptor chimeric antibody C225 alone and in
15. Torrance CJ, Jackson PE, Montgomery E,
ment and tumor biology. J Clin Oncol 23:3227-
combination with cisplatin. J Clin Oncol 18:904-
et al: Combinatorial chemoprevention of intesti-
23. Lee JW, Soung YH, Kim SY, et al: Somatic 9. Kies MS, Arquette MA, Nabell L, et al: 16. Eberhard DA, Johnson BE, Amler LC, et al:
mutations of egfr gene in squamous cell carci-
Final report of the efficacy and safety of the
Mutations in the epidermal growth factor recep-
noma of the head and neck. Clin Cancer Res
anti-epidermal growth factor antibody Erbitux
tor and in KRAS are predictive and prognostic
Downloaded from www.jco.org at DANA FARBER CANCER INST on December 1, 2005 .
Copyright 2005 by the American Society of Clinical Oncology. All rights reserved.
Quelle: http://www.naturepower.ch/blog/ Medikamente schädigen Ihren Vitalstoffhaushalt Wussten Sie, dass schon ein ganz normales Kopfschmerzmittel dafür sorgen kann, dass der Vitalstoff-haushalt in Ihrem Körper aus den Fugen gerät? Wie etliche andere Medikamente nämlich können auch Kopfschmerzmittel zu einer verstärkten Vitalstoff-Ausscheidung und einer verringerten Vitalstoffauf-na
OSTEOPOROSIS RISK FACTORS AND TREATMENT OPTIONS FACT SHEET What is osteoporosis? Osteoporosis is a disease characterized by low bone mass and structural deterioration of bone tissue, leading to bone fragility and an increased susceptibility to fractures of the hip, spine and wrist. Wolff’s Law (1868) states that bone mass and density will be increased in areas of stress. Conversely
 Gefitinib ؉ Celecoxib for SCCHN
Gefitinib ؉ Celecoxib for SCCHN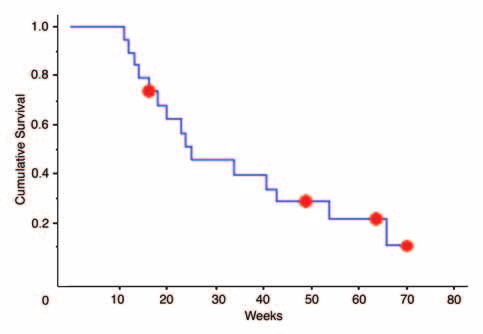 Wirth et al
Wirth et al