Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Xoomer.alice.it
JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 2005, p. 6027–6031
0095-1137/05/$08.00ϩ0 doi:10.1128/JCM.43.12.6027–6031.2005Copyright 2005, American Society for Microbiology. All Rights Reserved.
Presence of Rickettsia conorii subsp. israelensis, the Causative
Agent of Israeli Spotted Fever, in Sicily, Italy, Ascertained
Giovanni M. Giammanco,1 Giustina Vitale,2 Serafino Mansueto,2 Giuseppina Capra,1
Dipartimento di Igiene e Microbiologia1 and Dipartimento di Medicina Clinica e delle Patologie Emergenti,2
Received 31 May 2005/Returned for modification 17 July 2005/Accepted 17 September 2005
A retrospective analysis by molecular-sequence-based techniques was performed to correctly identify the etiological agent of 24 Mediterranean spotted fever cases occurring in Western Sicily, Italy, from 1987 to 2001. Restriction analysis of a 632-bp PCR-amplified portion of the ompA gene allowed presumptive identification of five clinical isolates as belonging to Rickettsia conorii subsp. israelensis, the etiological agent of Israeli spotted fever (ISF). The remaining 19 rickettsial isolates were Rickettsia conorii subsp. conorii, the only pathogenic rickettsia of the spotted fever group reported in Italy until the present. Sequence analysis of the ompA gene confirmed the identification of all the R. conorii subsp. israelensis isolates and demonstrated that rickettsiosis caused by R. conorii subsp. israelensis can be traced back to 1991 in Sicily. The recorded clinical data of the five ISF patients support the idea that these strains could correlate to more-severe forms of human disease. Three of five patients experienced severe disease, and one of them died.
Mediterranean spotted fever (MSF), also known as bouton-
subspecies has been proposed in order to separate these strains
neuse fever, is caused by Rickettsia conorii, an obligately intra-
on the basis of genetic and serological methods (26). There-
cellular, slow-growing gram-negative bacterium. The disease
fore, rickettsial isolates exhibiting close genetic similarity to
usually has a benign course and is characterized by the onset of
the R. conorii Malish type strain (ATCC VR-613) should be
high fever, myalgia, arthralgia, and a typical rash. However,
classified as Rickettsia conorii subsp. conorii, while three fur-
about 6% of the cases are severe, and fatal cases do occur even
ther subspecies, Rickettsia conorii subsp. indica, Rickettsia
in young, healthy adults, with a reported death rate of about
conorii subsp. caspia, and Rickettsia conorii subsp. israelensis,
2.5% (15). MSF is endemic in Italy, where it is a reportable
have been created to accommodate isolates genetically similar
disease. The Italian Ministry of Health received reports of 890
to the type strains of the Indian tick typhus rickettsia (ATC
cases of human rickettsioses presumed to be MSF in 2002.
C VR-597), the Astrakhan fever rickettsia (A-167), and the
MSF is more common in some central and southern regions of
ISF rickettsia (ISTTCDC1), respectively (26).
Italy (20, 22), reaching an average of 10 cases for every 100,000
R. conorii subsp. israelensis was first isolated in 1974 in Israel,
inhabitants in Sicily in 2002, compared with a national average
where its distribution initially appeared to be restricted (19),
of 1.6. Rickettsia conorii is thought to be the only pathogenic
but more recently it has also been isolated in Portugal (3). In
rickettsia of the spotted fever group (SFG) in Italy (22), as well
Italy, a number of different spotted-fever-group rickettsiae
as in the Western Mediterranean area, even if the possible
have been detected in Ixodes ricinus ticks from central and
circulation of strains different from classical R. conorii has been
northern regions, raising the possibility that bacteria other
proposed, mainly for clinical reasons (different degrees of se-
than R. conorii are involved in rickettsial diseases in our coun-
try (4). Our recent finding of R. conorii subsp. israelensis infec-
In recent years, the systematic identification of rickettsial
tion in a Rhipicephalus sanguineus tick, which is the main vector
species causing human infections has continued to increase the
for MSF in Sicily, also suggested that the geographic distribu-
number of recognized human pathogens. Since 1984, several
tion of ISF might be wider than previously thought, including
new agents of SFG rickettsioses have been recognized, includ-
not only Israel and Portugal but also Italy (7). To check
ing R. japonica, R. honei, R. africae, R. felis, R. slovaca, and R.
whether unusual tick-transmitted rickettsiae are actually in-
aeschlimannii (9, 12–14). Unusual rickettsial strains related to
volved in MSF in Sicily, we used molecular-sequence-based
R. conorii have been described as belonging to an “R. conorii
identification techniques to retrospectively study clinical iso-
complex” which includes the Indian tick typhus rickettsia, the
lates obtained from several cases of MSF over a 15-year period
Astrakhan fever rickettsia, and the Israeli spotted fever (ISF)
and previously identified by serological tests as belonging to
rickettsia (6, 17, 19). Recently, the creation of four R. conorii
the spotted-fever-group rickettsiae. MATERIALS AND METHODS
* Corresponding author. Mailing address: Dipartimento di Igiene
Rickettsial isolates. Rickettsiae of the spotted fever group were isolated by the
shell vial technique from blood samples collected from 24 patients hospitalized
Palermo, Italy. Phone: 39 0916553661. Fax: 39 0916553676. E-mail:
for MSF in Palermo, Sicily, Italy, in the years 1987 to 2001. Heavily infected Vero
cell monolayers were harvested and stored at Ϫ80°C until use. R. conorii subsp. conorii type strain Malish (ATCC VR-613) was kindly provided by D. H. Walker
TABLE 1. Rickettsial isolates collected in Sicily from blood
samples of patients hospitalized for MSF during
PCR amplification. Bacterial DNA was obtained from 200 l of infected Vero
cell suspensions by using the Wizard Plus SV Minipreps DNA PurificationSystem (Promega, Madison, WI) according to the manufacturer’s instructions.
PCR was performed with the primer pair Rr 190.70p–190.701, which amplifies
632-bp portions of the ompA gene, under conditions described previously (18).
Two microliters of the DNA preparation was amplified in a 100-l reaction
mixture containing 10 pmol each primer; 200 M (each) dATP, dCTP, dGTP
and dTTP (Amersham Pharmacia Biotech, Uppsala, Sweden), 1.25 U AmpliTaq
Gold DNA polymerase (Applied Biosystems, Foster City, CA), and 6 l of a 25
mM solution of MgCl2. Amplifications were carried out in a DNA thermal cycler
(GeneAmp PCR System 2400; Perkin-Elmer, Applied Biosystems Division, Nor-
R. conorii subsp. israelensis
walk, CT) under the following conditions. An initial 3 min of denaturation at
95°C was followed by 35 cycles of denaturation for 20 s at 95°C, annealing for 30 s
at 46°C, and extension for 1 min at 65°C. The amplification was completed by
holding for 7 min at 72°C. PCR products were purified as previously described by
Restriction analysis. Amplified products were submitted to restriction analysis
with endonucleases PstI and RsaI (Amersham Pharmacia Biotech) as previously
described (18). Restriction fragments were resolved on 10% polyacrylamide gels,
and electrophoresis was performed in 1ϫ TBE buffer, pH 8 (44.5 mM Tris, 44.5
mM boric acid, 1 mM EDTA), at 120 V for 3 h. Gels were stained with ethidium
bromide and examined with a UV transilluminator. HaeIII-digested pUC18
R. conorii subsp. israelensis
double-stranded DNA (Sigma-Aldrich, St. Louis, MO) was used as a molecular
weight marker to calculate the sizes of the restriction fragments. Sequence analysis. To confirm the presumptive identification obtained by R. conorii subsp. israelensis
restriction analysis, PCR products of the Israeli spotted fever rickettsia isolates
R. conorii subsp. israelensis
were sequenced in both the sense and antisense orientations (MWG-Biotech,
R. conorii subsp. israelensis
Germany), and forward and reverse sequence data of each sample were aligned
using the Bioedit program to obtain the final sequence. The DNA sequencesobtained in this study were analyzed using the BLAST program, availablethrough the National Center for Biotechnology Information (NCBI, Bethesda,MD; http://www.ncbi.nlm.nih.gov/BLAST/) (1). The phylogenetic relationshipbetween our sequences and those of other rickettsiae of the SFG, retrieved from
in 1995, 2000 (two), and 2001. Analysis of the sequences ob-
the GenBank database and selected on the basis of previous reports (6), was
tained from the amplified ompA fragments of the five clinical
studied. Complete alignment was performed with CLUSTAL W (21), and thealignment was analyzed using the Kimura 2-parameter model as a method of
R. conorii subsp. israelensis isolates showed their complete
substitution and neighbor joining to reconstruct the phylogenetic tree, using
identity. Comparison with homologous sequences from closely
MEGA 3.0 software (http://www.megasoftware.net/) (8). The statistical signifi-
related SFG Rickettsia spp. retrieved from GenBank showed
cance of the phylogenies constructed was estimated by bootstrap analysis with
100% identity to the reference R. conorii subsp. israelensis
1,000 pseudoreplicate data sets, and a tree was displayed with the MEGA
strain registered under accession number U43797, as well as to
Serological diagnosis. Results of serological diagnosis were recovered from
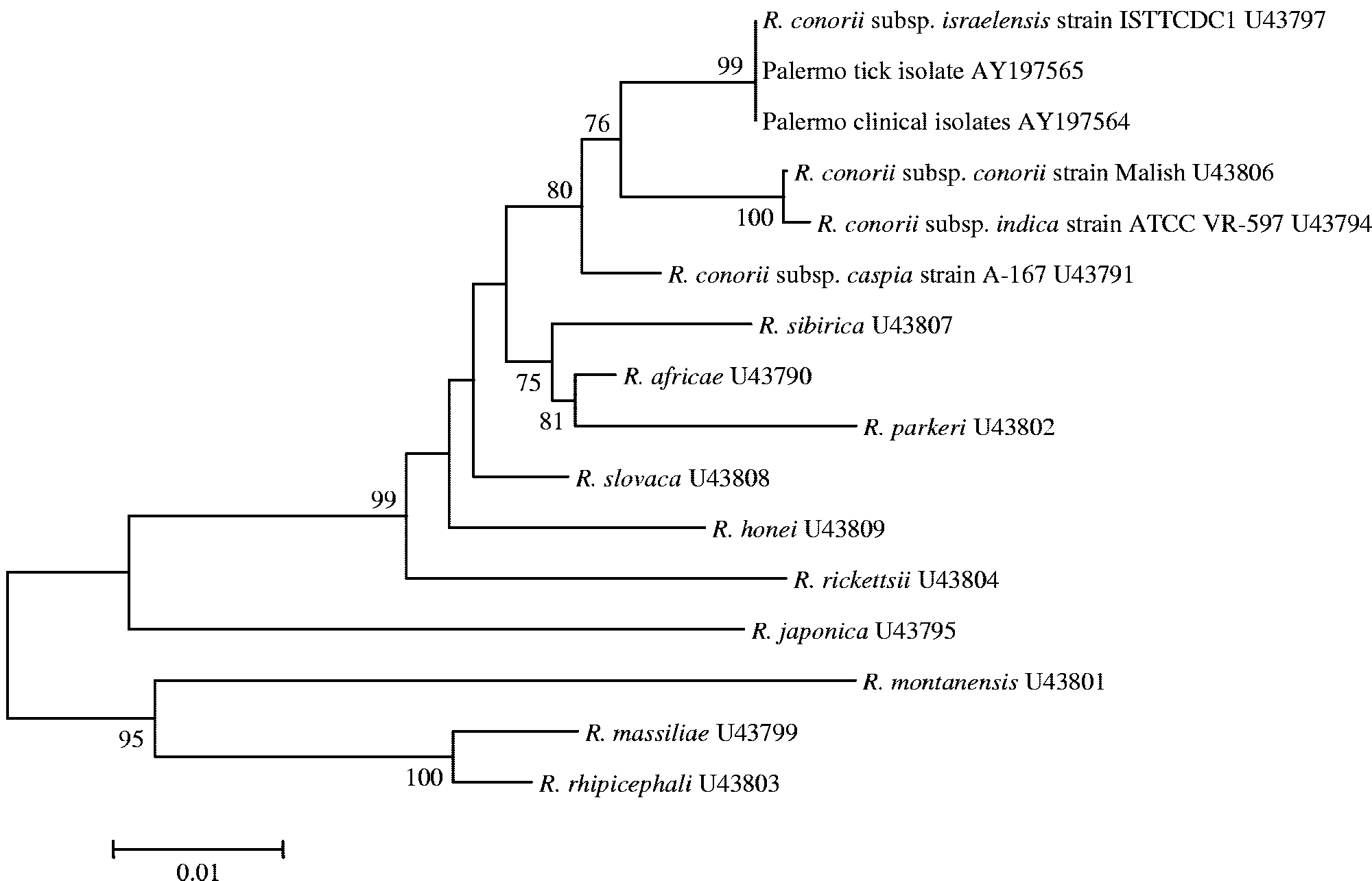
the rickettsia we isolated from a tick in 1990 (7). Figure 1
recorded data. Specific antirickettsial immunoglobulin M (IgM) and IgG deter-
shows the results of the phylogenetic analysis performed on
minations had been performed by an enzyme-linked immunosorbent assay
596-bp partial sequences of the PCR-amplified ompA genes of
(ELISA) or an indirect immunofluorescence (IIF) assay. In both cases, antigens
the five human isolates, confirming their identification as R.
had been obtained from a clinical isolate of R. conorii subsp. conorii (strainMAVI). Antigens had been freshly prepared in the hospital laboratory as de-
conorii subsp. israelensis.
Epidemiological, clinical, and laboratory data for the five
Statistical analysis. Epidemiological and clinical data of the two groups of
patients were recovered from the archives and are given in
patients, those infected by R. conorii subsp. conorii and those infected by R.conorii subsp. israelensis, were compared and submitted to statistical analysis by
Before the onset of the disease, none of the patients had a
the 2 test or the F test for analysis of variance. Results were consideredsignificant when the P value was Յ0.05.
history of tick bite, tick exposure, or a stay in an epidemiolog-
Nucleotide sequence accession number. The ompA gene sequence of the
ically suspected location. The illness had a sudden onset with
Italian clinical isolates of R. conorii subsp. israelensis described in this study has
fever, but no specific symptoms appeared during the first sev-
been deposited in GenBank and assigned accession number AY197564.
eral days. In all the patients, a macular or maculopapular rashappeared. Only two patients had a tache noire (eschar). Initial
antibacterial treatment at home (with oral penicillins or ceph-alosporins) had been started by three patients but did not
All the infected Vero cell suspensions from our collection
result in improvement. Five to 8 days after the onset of symp-
were positive for the ompA gene by PCR. Restriction analysis
toms, the patients were admitted to the hospital. Although they
with endonucleases PstI and RsaI was performed on all the
immediately received oral doxycycline therapy, in three cases
amplicons obtained. The observation of a peculiar 3-band PstI
disseminated intravascular coagulation (DIC) and progression
restriction profile allowed presumptive identification of five
toward coma was observed. One of these patients died the day
clinical isolates as belonging to R. conorii subsp. israelensis,
after admission, and DIC with acute renal and hepatic failure
while the remaining 19 rickettsial isolates were R. conorii
was diagnosed on the basis of laboratory tests showing severe
subsp. conorii (Table 1). The oldest R. conorii subsp. israelensis
thrombocytopenia, prolonged prothrombin time and activated
strain was isolated in 1991, while the other four were obtained
partial thromboplastin time, the presence of fibrin degradation
INFECTION WITH ISRAELI SPOTTED FEVER AGENT IN SICILY
FIG. 1. Phylogenetic analysis of rickettsiae based on partial ompA gene sequences. The GenBank accession number for each sequence is shown
adjacent to the strain designation. Numbers near each node represent bootstrap values. Bar, number of inferred substitutions at each site.
products and D-dimer, elevated levels of serum transaminases,
after 18 and 21 days, respectively. The remaining two ISF cases
bilirubin, creatinine, and blood urea nitrogen, decreased cre-
were milder, with clinical symptoms resolving after 7 and 12
atinine clearance, hepatomegaly, and splenomegaly. No ultra-
sound test or liver biopsy was performed to ascertain the extent
The serological data we recovered showed that specific an-
of hepatic necrosis. The other two coma patients recovered
tirickettsial Ig determinations had been performed for all ofthe patients. With the single exception of the patient who diedthe day after admission, at least two serum samples per patient
TABLE 2. Comparison of epidemiological and clinical data of
had been obtained and tested during hospitalization. For four
5 patients with ISF and 19 patients with classical MSF
patients, serological tests showed evidence of acute rickettsialinfection, e.g., the presence of IgM antibodies, seroconversion,
or a fourfold rise in antibody titer against SFG rickettsial
antigens (Table 3). In three cases, sera reacted at high titers
with the R. conorii subsp. conorii MAVI strain used for these
tests. The two serological tests used were generally in agree-
ment, but the IgG titer (slightly increasing in paired sam-
ples) revealed by ELISA for patient 1 was not detected by
The clinical data recovered for the 19 patients suffering from
classical Rickettsia conorii subsp. conorii MSF showed that all
but 2 had mild forms of disease and 12 had a typical eschar.
The mean age of R. conorii subsp. conorii MSF patients was 54
a NA, not available. b NS, not significant. ‡, P value calculated by the 2 test. §, statistical signifi-
cance calculated by analysis of variance through the F test. DISCUSSION c Diagnosed based on the following laboratory signs: thrombocytopenia
(Ͻ100,000/mm3), prolonged prothrombin time (Ͼ15 s) and activated partial
Our study demonstrates the presence of ISF caused by R.
thromboplastin time (Ͼ40 s), and presence of fibrin degradation products (Ͼ10
g/ml) and/or D-dimer (Ͼ0.5 g/ml). conorii subsp. israelensis in Sicily. This result was not surprising,
TABLE 3. Serological data of five patients with R. conorii subsp. israelensis infection
Titer by the following serological testc:
a Dates are given as mo/day/yr or mo/day. b Doxycycline therapy. c Both an ELISA and an IIF assay were performed with freshly prepared antigens obtained from a clinical isolate of R. conorii subsp. conorii (strain MAVI) as
since the infection had already been detected in R. sanguineus
Sicilian ISF patients did not allow calculation of a precise
ticks, the main vector for MSF in Sicily (7). Moreover, we were
severity score, three out of five patients could be considered to
able to trace back the infection in humans at least to the
have suffered from severe forms of disease, since one died of
beginning of the 1990s, since the first reported case was in
his illness and for the remaining two patients impaired con-
1991. Therefore, we can now affirm that the distribution of ISF
sciousness and progression toward coma was observed, and
is wider than previously thought and includes not only Israel
hospitalization in intensive care units, for more than 15 days,
and the Iberian Peninsula but also Sicily.
was required. Both the appearance of DIC signs and loss of
The Rhipicephalus sanguineus tick is the main vector for
consciousness were significantly associated with ISF (Table 2).
MSF in Mediterranean countries. Although contact with ticks
The supposed ability of the Israeli spotted fever rickettsia to
could not be documented from the recorded anamnestic data,
cause life-threatening disease has been ascribed to late diag-
it must be assumed also for Sicilian ISF patients and can be
nosis due to uncharacteristic presentation (25). An increase in
granted by the presence of the typical eschar associated with
severe cases of MSF has been seen in Sicily in recent years (11)
the tick bite site which was observed on two of them. The
and in Portugal in 1997, where it has been related to the
Sicilian ISF patients lived in urban or semirural areas of west-
presence of R. conorii subsp. israelensis (2, 5). A fulminant
ern Sicily, and none of them had left Italy during the previous
course of Israeli spotted fever has been correlated with glu-
year. R. conorii subsp. israelensis strains might have been im-
cose-6-phosphate dehydrogenase deficiency (16), but none of
ported from areas of endemicity through imported ticks (e.g.,
the Sicilian ISF patients had been tested for this.
on migrating birds) or rodents in recent years, but a long
The fact that a rapidly fatal outcome can occur stresses the
history of endemicity in Sicily cannot be excluded. The sea-
importance of prompt diagnosis and treatment, even for ap-
sonal distribution of infections was between June and Septem-
parently benign disease. In most cases, diagnosis of MSF is
ber, corresponding to that generally observed for MSF in our
based on serology. The serological data of our patients showed
region. Although the disease apparently affected slightly
that R. conorii subsp. israelensis produces a clear immuno-
younger people than classical R. conorii subsp. conorii MSF
logical response, providing evidence for acute rickettsial infec-
(mean ages, 49 and 54 years, respectively), this difference was
tion, and that serological tests using R. conorii subsp. conorii
not statistically significant, and only one of five ISF patients
antigens are able to detect it, confirming that cross-reactions
are common among rickettsiae of the two subspecies (26).
Clinical diagnosis of MSF relies on the following symptoms:
However, in some cases antibodies could be detected only
fever, tache noire, and rash. The absence of tache noire, the
several days after the onset of the disease. Confirmatory diag-
characteristic eschar at the site of the tick bite, has been de-
nosis in the acute phase must rely either on the detection of
scribed for Israeli spotted fever (3, 19). When the typical tache
rickettsiae in the clinical specimens by culture isolation with
noire sign is not present, there is a risk of delay in administra-
the shell vial technique, followed by identification using immu-
tion of appropriate antibiotic treatment. The inconsistent pres-
nohistochemistry or the indirect fluorescent antibody test, or
ence of the tache noire had already been observed in the past
on the detection of rickettsial DNA by PCR. The PCR tests
for MSF patients in Sicily (24). In this study, only two out of
have been demonstrated to allow fast detection of as few as 100
five ISF patients had a typical MSF tache noire, but the ab-
copies of rickettsial DNA through amplification of specific
sence of this feature was not significantly related to ISF pa-
sequences of the genes encoding the 16S rRNA, the 17-kDa
tients. Although the recorded clinical data we found on the
protein, citrate synthase (gltA), and the outer membrane pro-
INFECTION WITH ISRAELI SPOTTED FEVER AGENT IN SICILY
teins OmpA and OmpB (9, 10). However, in early stages and
12. Raoult, D., P. E. Fournier, P. Abboud, and F. Caron. 2002. First documented
until diagnosis continues to be clinical, patients should start
human Rickettsia aeschlimannii infection. Emerg. Infect. Dis. 8:748–749.
13. Raoult, D., P. E. Fournier, F. Fenollar, M. Jensenius, T. Prioe, J. J. de Pina,
appropriate therapy without delay if suspicion of rickettsiosis
G. Caruso, N. Jones, H. Laferl, J. E. Rosenblatt, and T. J. Marrie. 2001.
arises in order to prevent a poor outcome due to aggressive
Rickettsia africae, a tick-borne pathogen in travelers to sub-Saharan Africa.
rickettsial strains. Prevention programs aimed at containing
N. Engl. J. Med. 344:1504–1510.
14. Raoult, D., and V. Roux. 1997. Rickettsioses as paradigms of new or emerg-
contact with infected ticks should be encouraged not only in
ing infectious diseases. Clin. Microbiol. Rev. 10:694–719.
Sicily but also in countries where rickettsial diseases are en-
15. Raoult, D., P. J. Weiller, A. Chagnon, H. Chaudet, H. Gallais, and P. Casanova. 1986. Mediterranean spotted fever: clinical, laboratory and epi- demiological features of 199 cases. Am. J. Trop. Med. Hyg. 35:845–850.
16. Regev-Yochay, G., E. Segal, and E. Rubinstein. 2000. Glucose-6-phosphate REFERENCES
dehydrogenase deficiency: possible determinant for a fulminant course of
1. Altschul, S. F., T. L. Madden, A. A. Schaffer, J. Zhang, Z. Zhang, W. Miller,
Israeli spotted fever. Isr. Med. Assoc. J. 2:781–782. and D. J. Lipman. 1997. Gapped BLAST and PSI-BLAST: a new generation
17. Regnery, R. L., C. L. Spruill, and B. D. Plikaytis. 1991. Genotypic identifi-
of protein database search programs. Nucleic Acids Res. 25:3389–3402.
cation of rickettsiae and estimation of intraspecies sequence divergence for
2. Amaro, M., F. Bacellar, and A. Franca. 2003. Report of eight cases of fatal
portions of two rickettsial genes. J. Bacteriol. 173:1576–1589.
and severe Mediterranean spotted fever in Portugal. Ann. N. Y. Acad. Sci.
18. Roux, V., P. E. Fournier, and D. Raoult. 1996. Differentiation of spotted 990:331–343.
fever group rickettsiae by sequencing and analysis of restriction fragment
3. Bacellar, F., L. Beati, A. Franca, J. Pocas, R. Regnery, and A. Filipe. 1999.
length polymorphism of PCR-amplified DNA of the gene encoding the
Israeli spotted fever rickettsia (Rickettsia conorii complex) associated with
protein rOmpA. J. Clin. Microbiol. 34:2058–2065.
human disease in Portugal. Emerg. Infect. Dis. 5:835–836.
19. Roux, V., and D. Raoult. 1999. Phylogenetic analysis and taxonomic rela-
4. Beninati, T., N. Lo, H. Noda, F. Esposito, A. Rizzoli, G. Favia, and C. Genchi.
tionships among the genus Rickettsia, p. 52–66. In D. Raoult and P. Brouqui
2002. First detection of spotted fever group rickettsiae in Ixodes ricinus from
(ed.), Rickettsiae and rickettsial diseases at the turn of the third millennium.
Italy. Emerg. Infect. Dis. 8:983–986.
5. de Sousa, R., S. D. Nobrega, F. Bacellar, and J. Torgal. 2003. Mediterranean
20. Scaffidi, V. 1981. Current endemic expansion of boutonneuse fever in Italy.
spotted fever in Portugal: risk factors for fatal outcome in 105 hospitalized
Minerva Med. 72:2063–2070. (In Italian.)
patients. Ann. N. Y. Acad. Sci. 990:285–294.
21. Thompson, J. D., D. G. Higgins, and T. J. Gibson. 1994. CLUSTAL W:
6. Fournier, P. E., V. Roux, and D. Raoult. 1998. Phylogenetic analysis of
improving the sensitivity of progressive multiple sequence alignment through
spotted fever group rickettsiae by study of the outer surface protein rOmpA.
sequence weighting, position-specific gap penalties and weight matrix choice.
Int. J. Syst. Bacteriol. 48:839–849.
Nucleic Acids Res. 22:4673–4680.
7. Giammanco, G. M., S. Mansueto, P. Ammatuna, and G. Vitale. 2003. Israeli
22. Tringali, G., V. Intonazzo, A. M. Perna, S. Mansueto, G. Vitale, and D. H.
spotted fever rickettsia in Sicilian Rhipicephalus sanguineus ticks. Emerg. Walker. 1986. Epidemiology of boutonneuse fever in western Sicily. Distri-
Infect. Dis. 9:892–893.
bution and prevalence of spotted fever group rickettsial infection in dog ticks
8. Kumar, S., K. Tamura, and M. Nei. 2004. MEGA3: integrated software for
(Rhipicephalus sanguineus). Am. J. Epidemiol. 123:721–727.
Molecular Evolutionary Genetics Analysis and sequence alignment. Brief Bioinform. 5:150–163.
23. Vitale, G., R. Di Stefano, G. Damiani, and S. Mansueto. 1989. Character-
9. La Scola, B., and D. Raoult. 1997. Laboratory diagnosis of rickettsioses:
ization of Sicilian strains of spotted fever group rickettsiae by using mono-
current approaches to diagnosis of old and new rickettsial diseases. J. Clin.
clonal antibodies. J. Clin. Microbiol. 27:1081–1085.
Microbiol. 35:2715–2727.
24. Walker, D. H., S. Mansueto, and G. Tringali. 1986. Frequent occurrence of
10. Leitner, M., S. Yitzhaki, S. Rzotkiewicz, and A. Keysary. 2002. Polymerase
hepatic lesions in boutonneuse fever. Acta Trop. 43:175–181.
chain reaction-based diagnosis of Mediterranean spotted fever in serum and
25. Yagupsky, P., and B. Wolach. 1993. Fatal Israeli spotted fever in children.
tissue samples. Am. J. Trop. Med. Hyg. 67:166–169.
Clin. Infect. Dis. 17:850–853.
11. Picciotto, D., A. Provenzani, S. Sorrentino, F. Vitale, G. Vesco, S. Caracappa,
26. Zhu, Y., P. E. Fournier, M. Eremeeva, and D. Raoult. 2005. Proposal to and M. G. Verso. 2000. Rickettsia infections in Sicily and mass media:
create subspecies of Rickettsia conorii based on multilocus sequence typing
attention not entirely groundless. Med. Lav. 91:494–500.
and an emended description of Rickettsia conorii. BMC Microbiol. 5:11.
"Viagra" could reduce multiple sclerosis symptoms "Viagra" could reduce multiple sclerosis symptoms 05/2011 - Medicine and Health. IBB researchers have discovered that "Viagra" drastically reduces multiple sclerosis symptoms in animal models with the disease. The research demonstrates that a practically complete recovery occurs in 50% of the animals after eight days of t
que seu coração está mais rápido que o normal, e você pode se sentir tonto ou apresentar tremores. Você pode também ter dor de cabeça. Esses efeitos normalmente passam em poucas horas, mas você deve comunicar ao seu Se a dose usada foi muito maior do que a correta, chame seu médico imediatamente ou se dirija ao hospital ou pronto-socorro mais próximo. Leve esta bula ou medicamento
 INFECTION WITH ISRAELI SPOTTED FEVER AGENT IN SICILY
FIG. 1. Phylogenetic analysis of rickettsiae based on partial ompA gene sequences. The GenBank accession number for each sequence is shown
adjacent to the strain designation. Numbers near each node represent bootstrap values. Bar, number of inferred substitutions at each site.
INFECTION WITH ISRAELI SPOTTED FEVER AGENT IN SICILY
FIG. 1. Phylogenetic analysis of rickettsiae based on partial ompA gene sequences. The GenBank accession number for each sequence is shown
adjacent to the strain designation. Numbers near each node represent bootstrap values. Bar, number of inferred substitutions at each site.