Levitra has a minimal amount of contraindications which has increased its popularity wellbutrin xl uk You can buy quality certified medications from us at an affordable price.
Ulceras.net
The Effect of Short-Contact Topical Tretinoin Therapy for Foot Ulcers in Patients With Diabetes Wynnis L. Tom, MD; David H. Peng, MD, MPH; Atabak Allaei, BS; Daniel Hsu, DPM; Tissa R. Hata, MDObjective: To determine the efficacy and safety of short- Main Outcome Measures: The proportion of ulcers that
contact administration of topical tretinoin on foot
healed in each group and the degree of change in ulcer size. Results: Twenty-two patients, with a total of 24 foot ul- Design: Randomized, double-blind, placebo-
cers, completed the study. At the end of 16 weeks, 2 (18%)
of 11 ulcers in the control group and 6 (46%) of 13 ul-cers in the tretinoin treatment group healed completely. Setting: Outpatient clinic at a Veterans Affairs medical
Topical tretinoin therapy significantly decreased ulcer area
and depth compared with placebo treatment over the 16weeks of the study (PϽ.01 for surface area; P=.02 for
Patients: Twenty-four volunteers with diabetic foot
depth). Adverse effects mainly consisted of mild pain at
ulcers but without evidence of peripheral arterial dis-
Conclusions: Short-contact application of topical treti- Interventions: Patients were randomized to 4 weeks
noin improved the healing of foot ulcers in patients with
of daily treatment with either topical 0.05% tretinoin so-
diabetes. The tretinoin therapy was generally well toler-
lution (Retin-A) or placebo saline solution. Photo-
ated, without serious local or systemic adverse effects.
graphs and assessment of wound size and appearance wereassessed every 2 weeks for a total of 16 weeks. LOWEREXTREMITYULCERS foundthatshort-contactdailyapplica-
tion of topical tretinoin improved the heal-
ing of chronic leg ulcers in 5 patients who
patients with diabetes experiencing an ul-
cer at some time during their life.1 These
tissue, new vascular tissue, and new col-
ulcers significantly impact the quality of
life of the patient and often lead to ad-
fects of treatment with short-contact topi-
verse sequelae, including infection, osteo-
myelitis, gangrene, and amputation of the
affected limb.2 Agents able to stimulatewound healing in these patients have thepotential to reduce the large amount of
morbidity and mortality associated withlower extremity ulcers.
This study was approved by the Universityof California, San Diego, Committee forHuman Research and performed with writ-
See also pages 1368 Author Affiliations: Division of
ten informed consent from all volunteers. and 1449
Study design was a prospective, randomized,
double-blind, placebo-controlled clinical
trial in 24 human volunteers. The volunteers
Topical tretinoin (all-trans-retinoic
were patients of the Foot Clinic at the Veter-
ans Affairs Medical Center, San Diego, who
of partial- and full-thickness wounds when
had a lower extremity ulcer and a diagnosis
applied before wounding.3-5 The effects of
of diabetes mellitus. Patients who (1) were
tretinoin therapy on open wounds are still
unable to give informed consent, (2) had a
unclear. A recent report by Paquette et al6
known bleeding disorder, (3) were pregnant
(REPRINTED) ARCH DERMATOL/ VOL 141, NOV 2005
2005 American Medical Association. All rights reserved.
to which patients were assigned until the study was completed. Cadexomer iodine gel (Iodosorb; Healthpoint Ltd, Fort Worth,
Tex) was the topical agent used by the Foot Clinic for its dia-betic patients as part of standard wound care; it was the only other
topical treatment continued in all study patients.
Patients had photographs taken of their foot ulcer for evalu-
ation of initial size and appearance. The photographs (Macro3 SLR Camera; Polaroid Corp, Waltham, Mass) were taken with
standardized lighting and positioning for each patient. The ran-domly assigned solution was applied directly to the wound bedand left in contact for 10 minutes every day; it was then rinsed
off with normal saline. The 10-minute application time was cho-sen based on the case series of chronic wounds reported by Pa-quette et al.6 In their series, a short-contact 10-minute appli-
cation of topical tretinoin improved healing, with mild local
irritation; longer periods were too irritating to the surround-ing area. After rinsing off the randomly assigned solution, the
patients applied cadexomer iodine gel to the wound bed, which
was left on until the next day. This procedure was carried outonce a day for 4 weeks. Use of the assigned study solution wasthen discontinued, and treatment with cadexomer iodine gel
Figure 1. Patient disposition.
alone was continued once a day. Photographs and measure-ments of ulcer size were taken every 2 weeks after the patientsstarted the assigned treatment, for a maximum of 16 weeks af-
Table. Patient Characteristics*
ter the initiation of the study or until complete healing of theulcer occurred, whichever came first. Various wound param-
Tretinoin
eters, including erythema, edema, purulence, and necrotic tis-
Characteristic Group† Group‡
sue, were assessed at each visit by the same investigator (W.L.T.). The patients continued to receive routine care for their ulcers,
including wound off-loading with shoes modified to reduce pres-
sure to the ulcer area, debridement of callus and dead tissue,
and protection of the ulcerated area with appropriate dress-
ings. Routine care was provided by the 3 podiatrists (D.H. and
2 uninvolved colleagues) in the Foot Clinic, based on the ap-
pearance of the ulcer and clinic protocol, without knowledge
of the assigned treatment group. Ulcer surface area was mea-
sured with computerized planimetry (Sigma Scan Pro; SPSS Inc,
Chicago, Ill), and ulcer depth was measured at the deepest part
Patient demographics were compared with a t test (SigmaStat
*Values other than location of ulcer are expressed as mean ± SE.
Version 2.03; SPSS Inc). The proportion of healed ulcers over time
was assessed with Kaplan-Meier curves, which were compared
using the log-rank test. Repeated-measures analysis of variancewas used to test for significance of changes in ulcer surface areaand depth between the 2 study groups (SAS System; SAS Insti-
at the time of enrollment, (4) had infected ulcers or nearby
tute, Cary, NC). All results are reported as mean±SE; PՅ.05 was
tissues, or (5) had lower extremity ulcers due to large artery
taken as significant for all statistical analyses.
disease (by clinical examination and/or abnormal ankle-brachial index) were excluded from the study.
Forty-one patients with diabetic foot ulcers were evaluated
between June and September 2002. Twelve patients did notqualify for the study because of clinical evidence of lower ex-tremity peripheral arterial disease; 3 patients were excluded be-
Twenty-two patients completed the 16-week study. Of
cause of known or possibly infected ulcers; and 2 patients who
these, 20 patients had a single foot ulcer. The other 2 pa-
did not meet any exclusion criteria were not willing to partici-
tients, each of whom had 2 foot ulcers,were treated with
pate in the study. Twenty-four patients, all male, were en-
the same randomly assigned solution. Two enrolled pa-
rolled in the study (Figure 1).
tients dropped out of the study before completing the ini-
Patients were randomly divided into 2 groups: treatment with
tial 4-week treatment period. One patient did not con-
topical 0.05% tretinoin solution (Retin-A; Ortho Pharmaceuti-
tinue because he received a skin allograft for his ulcer.
cal Corp, Raritan, NJ) and treatment with normal saline solu-
The other patient chose to drop out of the study in the
tion that was colored the same as the topical tretinoin. Random-
first week because he no longer wanted to change his pre-
ization was performed by an uninvolved third party who used a
computer-generated random sequence to balance the numbersof the 2 treatment groups. Each newly enrolled patient was as-
A comparison of the 2 groups of patients (topical treti-
signed a topical solution in ascending order. The study was
noin and control) is shown in the Table. The 2 sets of
double-blind in that all dispensed bottles of solutions were iden-
patients were not significantly different in regard to age
tical in appearance (identified by number only), and neither the
(P=.47), duration of diabetes (P=.82), or hemoglobin A1c
investigators nor the patients were aware of the treatment group
level (P=.39). Initial ulcer size (surface area [P=.66] and
(REPRINTED) ARCH DERMATOL/ VOL 141, NOV 2005
2005 American Medical Association. All rights reserved.
depth [P = .28]) and duration of ulceration (P = .29) werenot statistically different between the 2 groups. The lo-
cation of the ulcers was also similar.
Five (45%) of 11 ulcers in the control group demon-
strated 50% or greater reduction in size by the end of thestudy period, compared with 11 (85%) of 13 ulcers in
the tretinoin group. Two ulcers (18%) in the control grouphealed completely, compared with 6 ulcers (46%) in the
tretinoin group. The progress of healing in the 2 groupsduring the study is shown as Kaplan-Meier curves in
Figure 2. Tretinoin therapy increased the proportion of ulcers that healed completely over the 16-week pe- riod (P = .03).
A comparison of the changes in surface area and ul-
cer depth are shown in Figure 3 and Figure 4, respec- tively. Tretinoin therapy significantly decreased ulcer area and depth compared with placebo treatment over the 16- Figure 2. Time to complete healing. The control group consisted of 11 foot ulcers (in 10 patients); the tretinoin group, 13 ulcers (in 12 patients). P = .03
week study period (PϽ.01 for surface area; P=.02 for
depth). At the end of the study period, the ulcer area hadchanged by −54.7 ± 28.8% in the tretinoin-treated group(P = .02 vs at the start of the study) and by ϩ2.7±47.2%
in the placebo-treated group (P = .18). The ulcer depth
was −60.1±13.8% in the tretinoin-treated group (P=.004
vs at the start of the study) and −29.6 ± 12.6% in the pla-
cebo-treated group (P = .04).
Two patients who were treated with 0.05% tretinoin
solution reported a very mild pain/burning sensation dur-
ing the first few days of application; this reaction did not
affect compliance and the symptoms resolved. Another
patient reported mild to moderate pain during the first
4 days of tretinoin therapy. He discontinued the treat-
ment for several days and subsequently resumed appli-
cation for the rest of the 4-week treatment period, with-
out experiencing pain. One patient in the control group
experienced mild to moderate pain with application ofhis study solution. He stopped the application for sev-
Figure 3. Change in surface area with time. Surface area was measured by
eral days during weeks 2 and 4 of the 4-week treatment
means of computerized planimetry analysis of photographs. PϽ.01 when the
period; he reported milder pain with this decreased fre-
quency of application, and his pain had resolved by thefifth week of the study. No significant erythema or edemawas noted in the area surrounding the ulcers in patients
in the tretinoin group. One patient in the control group
had mild surrounding erythema and edema at the start
of the study, both of which were gone by week 4. None
of the wounds demonstrated purulence or necrotic tis-
sue during the study period. No significant systemic ef-
fects were reported by either group.
This study demonstrated improvement in the healing of
diabetic foot ulcers when topical tretinoin was added to
standard therapy. It showed an increase in the numberof ulcers healed as well as a decrease in ulcer size, withmild adverse effects. Figure 4. Change in depth with time. Ulcer depth was measured with a probe at the deepest part of the wound. P = .02 when the 2 groups were compared.
Normal wound healing proceeds through a sequence
of overlapping processes: hemostasis, inflammation anddebridement, proliferation, wound contraction, epithe-
cular disease. These disturbances include prolonged in-
lialization, and remodeling.7,8 Patients with diabetes have
flammation, impaired neovascularization, decreased col-
multiple disturbances in wound healing, independent of
lagen synthesis, an abnormal pattern of synthesis of
their increased likelihood of developing peripheral vas-
extracellular matrix protein, and decreased fibroblast pro-
(REPRINTED) ARCH DERMATOL/ VOL 141, NOV 2005
2005 American Medical Association. All rights reserved.
tion tissue, new vascular tissue, and new collagen for-mation on histologic examination.
The present study aimed to see if short-contact appli-
cation of topical tretinoin would improve the healing offoot ulcers in patients with diabetes in a randomized, pla-cebo-controlled trial. More ulcers healed in the tretinoin-treated group over the 16-week study period. Planim-etry showed quicker decrease in the surface area and depth
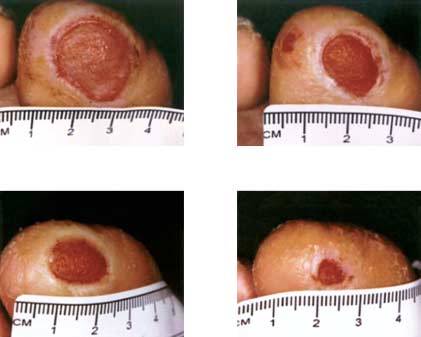
of ulcers, suggesting faster wound contraction. Im- proved formation of granulation tissue was also seen in patients treated with tretinoin (Figure 5).
Patients were entirely randomized to their treatment
group (tretinoin or placebo). It should be noted that pa-tients in the tretinoin group generally presented withslightly smaller and less chronic ulcers; although this dif-ference was not statistically significant, some of the mea-
sured improvement could be attributed to this ten-dency. Larger studies are needed to confirm efficacy.
As mentioned, irritation caused by topical tretinoin
Figure 5. Improved healing and formation of granulation tissue in a
therapy is often a concern. In our study, short-contact
representative patient treated with topical 0.05% tretinoin solution.
application of tretinoin caused mild to moderate pain andirritation in several patients in the initial period of treat-
liferation.1,9 Current techniques of treatment include off-
ment, but either the symptoms self-resolved or the treat-
loading to avoid mechanical stress on the wound, de-
ment was able to be restarted after several days without
bridement to remove devitalized tissue, and improvement
application. No significant surrounding erythema or
edema was noted with tretinoin. Short-contact applica-
As a retinoid, tretinoin may enhance wound healing
tion appeared to be well-tolerated, as in the report by Pa-
by its effect on cell division and differentiation. The
quette et al.6 Additional factors that allowed tolerance of
use of tretinoin increases epidermal thickness and cell
topical tretinoin on open wounds included instruction
turnover, which may lead to faster reepithelialization.
to avoid application to the surrounding intact skin to re-
It also stimulates angiogenesis in the superficial der-
duce irritation to the surrounding area. Peripheral neu-
mis.11,12 This neovascularization allows delivery of
ropathy associated with diabetes, while making the pa-
oxygen and nutrients, and the endothelial cells secrete
tient more prone to injury or trauma to cause or worsen
biologically active substances, including growth fac-
foot ulcers,1 may also limit the sensation of pain due to
tors.4 The use of retinoids also increases granulation
topical tretinoin. Most of the diabetic foot ulcers were
tissue formation by increasing mucopolysaccharide,
located on the plantar surface, which has a thicker epi-
collagen, and fibronectin synthesis.12 Therefore, treti-
dermis and less sensitivity to pain.
noin has been studied as an agent that can potentially
In conclusion, this pilot study found that short-
contact application of topical tretinoin can improve the heal-
Topical tretinoin therapy has been found to improve
ing of foot ulcers in patients with diabetes. It suggests that
healing of partial- and full-thickness wounds when ap-
topical tretinoin therapy may be a good addition to the al-
plied before wounding. In human patients, it has been
ready established methods of treating diabetic foot ulcers.
found to accelerate healing when used as pretreatment
Larger randomized, controlled trials are needed to further
before the administration of trichloroacetic acid peels on
delineate the efficacy and effects of its use.
actinically damaged skin of the face and arms,3 derm-abrasion of the face,13 and electroepilation of the axillae
Accepted for Publication: December 1, 2004.
and groin.14 Reepithelialization occurred faster in full-
Correspondence: Tissa R. Hata, MD, University of Cali-
thickness wounds in actinically damaged skin that was
fornia, San Diego, Perlman Ambulatory Care Center, 9350
first treated with topical tretinoin for 16 weeks.4 Appli-
Campus Point Dr, Mailcode 0974, La Jolla, CA 92037
cation on already open wounds, however, has yielded
varying results. In some animal models, tretinoin therapy
Author Contributions: Study concept and design: Tom,
has been found to enhance healing4,15,16; in others, it has
Peng, Hsu, and Hata. Acquisition of data: Tom and Allaei.
been shown to have no effect17 or to cause inflammation
Analysis and interpretation of data: Tom, Peng, Allaei, and
and excessive granulation without reepithelializa-
Hata. Drafting of the manuscript: Tom and Allaei. Criti-
tion.5,18 It has been suggested that tretinoin may be too
cal revision of the manuscript for important intellectual con-
irritating when applied after wounding has occurred, es-
tent: Tom, Hsu, and Hata. Statistical analysis: Tom and
pecially to the surrounding skin.4,5 Recently Paquette et
Peng. Administrative, technical, and material support: Allaei,
al6 introduced the use of short-contact daily application
Hsu, and Hata. Study supervision: Hata.
of topical tretinoin and found that it improved the heal-
Acknowledgment: The topical tretinoin used in this study
ing of chronic leg ulcers in 5 patients who were using
was provided by Ortho-Neutrogena. We thank Nancy
immunosuppressive agents for systemic illnesses. Short-
Chen for assistance with study conception and design and
contact application still stimulated increased granula-
John Malone and Ingrid Kruse for patient referral.
(REPRINTED) ARCH DERMATOL/ VOL 141, NOV 2005
2005 American Medical Association. All rights reserved.
9. Martin A, Komada MR, Sane DC. Abnormal angiogenesis in diabetes mellitus. Med Res Rev. 2003;23:117-145.
10. Mekkes JR, Loots MA, Van Der Wal AC, Bos JD. Causes, investigation and treat-
1. American Diabetes Association. Consensus Development Conference on Dia-
ment of leg ulceration. Br J Dermatol. 2003;148:388-401.
betic Foot Wound Care: 7-8 April 1999, Boston, Massachusetts. Diabetes Care.
11. Bhawan J. Short- and long-term histologic effects of topical tretinoin on pho-
todamaged skin. Int J Dermatol. 1998;37:286-292.
2. Vileikyte L. Diabetic foot ulcers: a quality of life issue. Diabetes Metab Res Rev.
12. Elson ML. The role of retinoids in wound healing. J Am Acad Dermatol. 1998;39:
3. Hevia O, Nemeth AJ, Taylor JR. Tretinoin accelerates healing after trichloroace-
13. Mandy SH. Tretinoin in the preoperative and postoperative management of
tic acid chemical peel. Arch Dermatol. 1991;127:678-682.
dermabrasion. J Am Acad Dermatol. 1986;15:878-879, 888-889.
4. Popp C, Kligman AM, Stoudemayer TJ. Pretreatment of photoaged forearm skin
14. Anthony J, Miller L, Dinehart SM. Topical tretinoin decreases healing times of
with topical tretinoin accelerates healing of full-thickness wounds. Br J Dermatol.
electroepilation-induced wounds. Dermatologica. 1991;183:129-131.
15. Basak PY, Eroglu E, Altuntas I, Agalar F, Basak K, Sutcu R. Comparison of the
5. Hung VC, Lee JY, Zitelli JA, Hebda PA. Topical tretinoin and epithelial wound healing.
effects of tretinoin, adapalene and collagenase in an experimental model of wound
Arch Dermatol. 1989;125:65-69.
healing. Eur J Dermatol. 2002;12:145-148.
6. Paquette D, Badiavas E, Falanga V. Short-contact topical tretinoin therapy to stimu-
16. Hunt TK, Ehrlich HP, Garcia JA, Dunphy JE. Effect of vitamin A on reversing the
late granulation tissue in chronic wounds. J Am Acad Dermatol. 2001;45:382-
inhibitory effect of cortisone on healing of open wounds in animals and man.
7. Brissett AE, Hom DB. The effects of tissue sealants, platelet gels, and growth
17. Otley CC, Gayner SM, Ahmed I, Moore EJ, Roenigk RK, Sherris DA. Preopera-
factors on wound healing. Curr Opin Otolaryngol Head Neck Surg. 2003;11:
tive and postoperative topical tretinoin on high-tension excisional wounds and
full-thickness skin grafts in a porcine model: a pilot study. Dermatol Surg. 1999;
8. Hess CL, Howard MA, Attinger CE. A review of mechanical adjuncts in wound
healing: hydrotherapy, ultrasound, negative pressure therapy, hyperbaric oxy-
18. Watcher MA, Wheeland RG. The role of topical agents in the healing of full-
gen, and electrostimulation. Ann Plast Surg. 2003;51:210-218.
thickness wounds. J Dermatol Surg Oncol. 1989;15:1188-1195. Trial Registration Required
As a member of the International Committee of Medi-cal Journal Editors (ICMJE), Archives of Dermatology willrequire, as a condition of consideration for publication,registration of all trials in a public trials registry (suchas http://ClinicalTrials.gov). Trials must be registered ator before the onset of patient enrollment. This policy ap-plies to any clinical trial starting enrollment after July1, 2005. For trials that began enrollment before this date,registration will be required by September 13, 2005, be-fore considering the trial for publication. The trial reg-istration number should be supplied at the time of sub-mission.
For details about this new policy, and for information
on how the ICMJE defines a clinical trial, see the edito-rial by DeAngelis et al in the January issue of Archives ofDermatology (2005;141:76-77). Also see the Instructionsto Authors on our Web site: www.archdermatol.com.
(REPRINTED) ARCH DERMATOL/ VOL 141, NOV 2005
2005 American Medical Association. All rights reserved.
Shaklee Health Sciences e-Bulletin Fall 2007 New study shows Echinacea helps reduce likelihood of contracting a cold as well as shorten its duration. According to researchers at the University of Connecticut School of Pharmacy, Echinacea actually reduces the chances of catching the common cold by 58 percent and reduces the duration of the common cold by nearly one and a half
VETADRYL® A Flavored Diphenhydramine HCl Tablet For Dogs and Cats VETADRYL® 10 VETADRYL® 30 CAUTION: Federal law restricts this drug to use by or on the order of a CAUTION: Federal law restricts this drug to use by or on the order of a Each scored tablet contains Each scored tablet contains Diphenhydramine HCl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
 tion tissue, new vascular tissue, and new collagen for-mation on histologic examination.
tion tissue, new vascular tissue, and new collagen for-mation on histologic examination.