Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients priligy uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Doi:10.1016/j.sleep.2003.06.006
The effects of trazodone on sleep in patients treated
Hakan Kaynaka,*, Derya Kaynaka, Erbil Go¨zu¨kırmızıa, Christian Guilleminaultb
aDepartment of Neurology, Sleep Disorders Unit, Cerrahpasa Medical School, University of Istanbul, Cerrahpasa, 34303 Istanbul, Turkey
bStanford Sleep Disorders Clinic and Research Center, Stanford, CA, USA
Received 12 March 2003; received in revised form 25 June 2003; accepted 26 June 2003
Background and purpose: To evaluate the effects of trazodone on subjective and objective measures of sleep in depressed insomnia
patients treated with selective serotonin reuptake inhibitors (SSRIs). SSRIs can exacerbate or cause new insomnia while alleviating othersymptoms of depression. Trazodone has been reported to be an effective hypnotic for patients with antidepressant-associated insomnia.
Patients and methods: Twelve female patients were given either 100 mg trazodone or placebo for 7 days in a double-blind crossover
design with a 7-day washout period. Polysomnographic recordings were repeated on the 3rd, 9th and 17th, 23rd nights after treatment withtrazodone or placebo. Sleep was assessed by Pittsburgh sleep quality index (PSQI) at the beginning and end of the study. Psychologicalevaluation was done by Hamilton depression rating scale (HDRS).
Results: Trazodone significantly increased total sleep time, percentage of stages 3 þ 4, sleep efficiency index, sleep continuity index and
decreased percentage of stage 1, number of awakenings, stage shifts compared to the baseline. This improvement was also obtained after7 days of treatment. The PSQI score was reduced to 5 ^ 1.6 at the end of the study. HDRS was reduced to 11.5 ^ 4.5 with trazodone and to12.2 ^ 3 with placebo.
Conclusion: Trazodone is effective in the treatment of antidepressant-associated insomnia.
q 2003 Elsevier B.V. All rights reserved.
Keywords: Insomnia; Depression; Trazodone; Serotonin reuptake inhibitors; Polysomnography; Hypnotic
Trazodone, a sedating triazolopyridine antidepressant, is
chemically and pharmacologically different from SSRIs. It
Insomnia is a hallmark or core symptom in the majority
possesses antidepressant and also some anxiolytic and
of depressed patients. It has been estimated that more than
hypnotic activities. The effects of trazodone on sleep have
70% of depressed women and 80% of depressed men have
been evaluated in a variety of subjects, including patients
difficulty falling and/or staying asleep or in early morning
with insomnia and depression and normal controls. It has
awakenings Insomnia may also occur as a side effect
been demonstrated to be effective in resolving depressive
of antidepressant treatments such as selective serotonin
symptomatology and improving sleep architecture .
reuptake inhibitors (SSRIs). Depressed individuals taking
Trazodone has also been reported to be an effective hypnotic
SSRIs often report persistent insomnia. These agents are
for patients with antidepressant-associated insomnia. Jacob-
stimulating antidepressants that can fail to treat preexisting
sen gave trazodone, 25 – 150 mg at night, in an open
insomnia, exacerbate preexisting insomnia or cause new
design to 48 consecutive patients who had persistent or
insomnia while alleviating other symptoms of depression
worsened insomnia while taking either monoaminooxidase
It was reported that a total of 35% of patients
inhibitors (MAOIs) or other antidepressants. He found that
receiving SSRIs or clomipramine were also taking medi-
65% had complete resolution of insomnia, 31% had partial
response and 4% had no response. Metz and Shader reported that 31% of patients who took trazodone at a dose
* Corresponding author. Tel.: þ90-212-586-1596; fax: þ90-212-632-
of 25 – 75 mg nightly to treat fluoxetine-associated insomnia
E-mail address: [email protected] (H. Kaynak).
had to stop taking trazodone because of excessive daytime
1389-9457/$ - see front matter q 2003 Elsevier B.V. All rights reserved. doi:10.1016/j.sleep.2003.06.006
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
sedation. Nierenberg et al. reported that patients taking
SSRIs were being used for the treatment of depression, with
either fluoxetine or bupropion and having antidepressant-
the dosages in the low normal range. Five patients were
associated insomnia showed clinically significant improve-
taking paroxetine (20 mg/day), three were taking sertraline
ment, according to the Pittsburgh index measure of sleep
(50 mg/day), two were taking fluoxetine (20 mg/day), and
duration and the Yale-New Haven inventory measure of
one was taking citalopram (20 mg/day). One patient was
early morning awakenings, after taking trazodone. There
taking venlafaxine (37.5 mg/day), which is both serotonin
was also a trend toward improvement in the Pittsburgh
and also norepinephrine reuptake inhibitor.
index subscales for sleep quality and sleep latency.
SSRI treatment duration had ranged from 4 weeks to
The above clinical reports are limited by the lack of
3 months at the beginning of the study. The mean duration
polysomnographic recordings (PSG) and a placebo control.
of SSRI treatment was 9 ^ 2.7 weeks (median: 9.5 weeks).
The aim of the present study is to evaluate the effects of
It was 9 ^ 2.6 (median: 9.5 weeks) in Group 1 and
trazodone on subjective and objective measures of sleep in
9.1 ^ 2.9 (median: 9.5 weeks) in Group 2. There was no
depressed insomnia patients treated with different SSRIs. It
statistical significance between groups 1 and 2 in terms of
is a double-blind placebo-controlled study to find out if
SSRI treatment (Mann – Whitney U test ¼ NS).
trazodone would improve sleep in depressed patients whose
Half of the randomly selected patients took placebo in
depression has been treated with SSRIs but in whom
the first treatment phase while the other half took trazodone,
insomnia was not resolved or insomnia was subsequently
and vice versa in the second treatment phase.
During an adaptation night in the sleep laboratory, each
patient’s sleep was evaluated and checked for other causes
of insomnia, such as PLMS, SRBD, etc. Following theadaptation night, they underwent baseline PSG (N2). After
Female subjects between the ages of 20 and 50 were
baseline recordings, patients were randomly assigned to
recruited from Psychiatry outpatient clinic. All of them had
either 100 mg trazodone (Group 1) or matching placebo
been diagnosed with major depression according to the
tablets (Group 2) in phase 1, and were administered the
DSM 4 criteria. They had been treated with SSRIs for at
alternative in phase 2. Each phase lasted 7 days, with a
least 3 weeks, were receiving antidepressants at the time of
washout period of 7 days between the two sets of
study, had complaints of new, exacerbated or untreated
insomnia, and continued with their treatment during the
PSGs were repeated on 3rd (N3), 9th (N9), 17th (N17)
study. An initial score of at least 18 on the Hamilton
and 23rd (N23) nights after the start of trazodone or placebo
depression rating scale (HDRS) was required. The exclusion
treatment. A 100 mg dose of trazodone was selected to
investigate its hypnotic effect, which is substantially lessthan the 150 – 600 mg dose range recommended for an
1. Suffering from concomitant mental illness other than
antidepressant effect . Medications were given 1 h
2. Alcohol abuse and addiction to other drugs3. Pregnancy or lactation
4. Suffering from any other causes of insomnia, such as
periodic leg movement during sleep (PLMS), sleep
HDRS was used for the evaluation of depression. It
related breathing disorders (SRBD), etc.
was done before baseline night and repeated after N9 and
5. Having cardiac conduction delays or arrhythmia in the
N23. Sleep was assessed by subjective rating of Pittsburgh
sleep quality index (PSQI) as sleep quality represents a
6. Having a history of intolerable adverse reaction to
complex clinical construct that is difficult to define and
measure objectively. The PSQI is a self-noted questionnairethat assesses sleep quality and sleep disturbance over a
A total of 12 female patients with a mean age of 42 ^ 9
1-month period, changed to the time frame used in this study
(range: 30 – 59, median: 43.5), responding to inclusion and
to avoid misinterpretation of PSQI. Since the treatment
exclusion criteria participated in the study and signed
phases were only 7 days, PSQI was measured at the baseline
and end of the study. This design was implemented with the
Eight patients complained of difficulties with falling
understanding that all subjects at entry would be free of
asleep and maintaining sleep, and four described relatively
hypnotics and that at the end of the study there would be a
isolated difficulty with falling asleep. Ten patients were
50% chance for the subjects to be on placebo when PSQI
suffering from untreated insomnia, while the remaining two
was administered. Study design and clinical evaluation of
developed insomnia during treatment with SSRSs. Different
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 1. Polysomnographic and clinical evaluation.
condition. PSQI scores were tabulated at the beginning andend of the study and compared between groups 1 and 2. PSG
PSG recordings included two EEGs (C3-A2, C4-A1),
sleep parameters of baseline night were compared with
two EOGs and one chin EMG. Respiration was recorded by
those of the first and last treatment nights of trazodone and
standard measures of airflow (oro-nasal thermistors), effort
placebo. Sleep parameters in the first treatment night (acute
(abdominal and thoracic strain gauges) and oxygen
effect) were also compared with those in the last treatment
saturation (finger pulse oximetry). Leg movements were
night (short-term effect), after 7 days of treatment with
recorded by right and left tibialis EMGs during the
The time of retiring was the same as at home but time in
bed was controlled at 8 h in all PSGs. The following PSGparameters were evaluated: total sleep time (TST), percen-
tage of stages 1, 2, 3 þ 4 and REM sleep, sleep latency,REM sleep latency, sleep efficiency index (SEI), sleep
continuity index (SCI), number of awakenings (# awake; aactivity , 15 s), number of stage shifts (# shifts) and mean
The initial HDRS score was 23.4 ^ 3.7. It was reduced
duration of each sleep cycle (cycle). SEI is TST per time in
to 12.2 ^ 3 ðP , 0:005Þ with placebo and to 11.5 ^ 4.5
bed (from lights out to lights on) and SCI is TST per total
ðP , 0:005Þ with trazodone treatment. This represented a
sleep period (from the first falling asleep to last awakening).
mean decrease of 46.3 and 49.2%, respectively. The effects
All PSG recordings were scored by blinded sleep specialists.
of trazodone and placebo on mean HDRS scores did notdiffer significantly.
The mean global score of the PSQI was 15 ^ 2.5 at the
beginning of the study (range: 9 – 19). It was 14.6 ^ 3.4 for
The order of the treatments was assigned randomly.
Group 1 ðn ¼ 6Þ and 15.5 ^ 1.5 for Group 2 ðn ¼ 6Þ at entry
There was no significant difference between phases 1 and 2
(Mann – Whitney U ¼ NS). After 3 weeks of trazodone/
subjects in the overall PSQI data and HDRS scores after
placebo treatment with washout period, it was reduced to
placebo treatment (Mann – Whitney U test ¼ NS). There-
5 ^ 1.6 (range: 2 – 7) ðP , 0:005Þ: It was 4.83 ^ 2.14 for
fore, PSG data and HDRS scores were grouped based on the
Group 1 and 5.17 ^ 1.17 for Group 2. There was no
treatment, regardless of the order. There was an equal
significant difference between the two groups at the end of
number of subjects in each group as none of the subjects
the study. According to the last PSQI, there was a similar
improvement in subjective sleep quality in both groups,
The data were grouped as baseline, drug, and placebo
despite the fact that 50% of the subjects had just received
conditions. The 14-day time difference between the two
placebo for 15 days. Compared to baseline, the change in
groups was not taken into consideration. The drug condition
PSQI score was significant for both groups (Wilcoxon
data consisted of data from the ‘first trazodone’ group
matched pair rank test ¼ 0.027). The global PSQI score was
(Group 1) on N3-N9 and ‘first placebo’ group (Group 2) on
5 or less in half of the patients, 6 in four patients and 7 in
N17-N23. The placebo condition data consisted of data
only two patients. It was 4.8 ^ 2.1 for Group 1 and
from the first trazodone group on N17-N23 (Group 1) and
first placebo group on N3-N9 (Group 2).
Side effects: Complaints were minimum. During the
The following comparisons were made using the
trazodone intake one subject reported mild and transient
Wilcoxon matched pair signed rank test. Mean percentage
acid indigestion and two others had mild daytime sedation
of reduction in HDRS as of the last treatment nights of
in the morning. Neither complaint was mentioned during the
placebo and trazodone were compared with the baseline
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 2. Global PSQI scores of patients at the beginning and at the end of the study.
they were still significantly higher than the baselinecondition. However, decreases in stage1 (3 ^ 2%,
Baseline sleep parameters of our patients are shown in
P , 0:001), number of awakenings (12 ^ 13, P , 0:05)
Large numbers of awakenings (25.1 ^ 11) and
and number of stage shifts (64 ^ 46, P , 0:01) and
stage shifts (106.2 ^ 37.6) led to low SEI (79.8 ^ 12.4%)
increases in percentage of stage 3 and 4 (31 ^ 13%,
and low SCI (85 ^ 9%). Mean sleep duration was
P , 0:01) were more significant in the last treatment
382.1 ^ 57.9 min and mean sleep latency was 18.8 ^
night of trazodone. Sleep latency was reduced from 17 to
28.7 min. Slow wave sleep (SWS) was well preserved
14 min. Percentage of REM sleep was slightly lower in
the last night (16 ^ 8%) than in the first (18 ^ 9%),
(13.2 ^ 4.9%) and stage 2 was increased (60.7 ^ 11.1%).
while its latency prolonged to 230 from 200 min.
Prolonged REM latency (222.9 ^ 93.4 min) was observed
In summary, the significant improvement in sleep
parameters in the first night of trazodone administration
The administration of trazodone significantly increased
was also observed after 7 days of treatment, compared to the
TST (435 ^ 34, P , 0:01), percentage of stages 3 þ 4
baseline night. The improvement in sleep parameters was
(28 ^ 14, P , 0:05), SEI (90 ^ 7%, P , 0:01) and SCI
more marked in the last treatment night, but no significant
(94 ^ 6%, P , 0:01) and significantly decreased percen-
difference was found between two treatment nights of
tage of stage 1 (3 ^ 1, P , 0:001), number of awakenings
(13 ^ 6, P , 0:01) and number of stage shifts (69 ^ 21,
Placebo treatment produced no significant alterations in
P , 0:05) on the first night, compared to the baseline night
sleep parameters, either in the first or last night compared to
the baseline. Sleep latency was prolonged to a mean of 24
At the end of trazodone treatment period (short term
and 33 min in the first and last treatment nights, respec-
effect), TST (428 ^ 39, P , 0:05), SEI (89 ^ 8%,
tively. Though the number of stage shifts was reduced to 89
P , 0:05) and SCI (93 ^ 7%, P , 0:05) tended to decrease
with acute administration, it reached 128 in the last
slightly compared to the first treatment night, although
treatment night, which was higher than the baseline night.
P values compared to baseline night. aP , 0:05; bP , 0:01; cP , 0:005; dP , 0:001:
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
The only significant finding with placebo treatment was an
awakenings and stage shifts, and augmentation of SWS. The
increase in the number of stage shifts during the last night
findings in our patients were more marked than those
(128 ^ 3, P , 0:01) compared to its acute administration
reported by Mouret et al. after only one night of drug intake.
(89 ^ 36). Sleep parameters with trazodone and placebo
Scharf and Sachais reported on six depressed patients
who took 150 mg doses of trazodone for 2 days, 200 mg for2 days and 250 mg by the end of the first week. Theirsubjects had decreased sleep latency and increased TST,
stage 4 NREM sleep and REM latency. The observed effectson REM sleep after the first day and after 1 week of
Our study confirms the finding that the administration of
treatment were different than those seen in our patients, who
a low dose of trazodone objectively improves sleep duration
initially had an increase in percentage of REM sleep with a
in patients who are being treated with antidepressants and
shortening of its latency. REM sleep latency was longer
have insomnia . Insomnia may be a side effect of some
after 1 week of trazodone than at baseline.
antidepressants such as SSRIs, or may be related to
A polygraphic study of the effects of trazodone on sleep
depression. It has been reported that 6 days of fluoxetine
parameters of depressed patients being treated with daily
treatment leads to significant decrease in REM sleep and
doses of SSRIs is lacking. In our study, trazodone,
increase in sleep latency and REM latency, without a
compared to placebo, produced significant improvement
significant increase in the number of awakenings during the
in sleep parameters with augmentation of TST, SWS, SEI
night . Hendricks et al. reported that fluoxetine
and SCI and reduction in stage 1, number of awakenings
appeared to increase in stage 1, suppress REM sleep and
and number of stage shifts after 1 week of treatment; there
increase REM latency. Another study done with fluoxetine
was no significant difference between the first and last
supported these findings and also showed decrease in SWS
night effects of trazodone on polysomnographic data.
Paroxetin has been reported to reduce TST, REM sleep
Although there was a notable reduction in HDRS, none of
and SEI, and increase REM latency and number of
the sleep parameters significantly improved with placebo
treatment. These findings indicate that trazodone amelio-
The sleep disturbances seen in depression are well
rated sleep disturbance in depressed patients, independent
described. They include increased nocturnal wake time,
of changes in depression, and that it was effective after the
decreased SWS and shortened REM latency. The mean
HDRS score was 23.4 ^ 3.7 at the beginning of our study,
The PSQI was administered at the beginning and end of
reflecting moderate depression despite SSRI treatment for a
our study. None of the subjects had been treated with
mean of 9 weeks (minimum 4 weeks). The elevated HDRS
trazodone at the outset, and subjective complaints were
scores in our patients suggest that depression may have been
clear. At the end, 50% of the subjects had not received
impacting sleep disturbance. Sleep onset complaints during
trazodone for at least 2 weeks (due to washout and placebo
SSRI treatment show that sleep problems are a side effect of
periods). Despite this situation, the mean PSQI score of our
these drugs. Although it is not possible to calculate apercentage of sleep problems arising from depression versus
patients was significantly reduced from 15 to 5; it has been
SSRIs, we know that both components affect sleep.
previously reported that global PSQI # 5 correctly identified
The baseline PSG data of our patients reflects the overall
89.6% of healthy, middle-aged control subjects There
effects of SSRIs and depression on sleep parameters. A
was no significant difference in PSQI scores between the
reduction of TST and SEI, increase in the number of
two groups at the conclusion of the study, and the scores
awakenings, and preservation of SWS was found. REM
were significantly better than those obtained at baseline. The
duration was reduced (13.2 ^ 4.9%) while REM latency
fact that PSQI scores in Group 2 were improved after
2 weeks without trazodone indicates the importance of close
Mouret et al. studied the polysomnographic changes
and repetitive subjective evaluations of sleep and the
induced by trazodone (100 – 600 mg) in 10 depressed
subjective effect of the attention given to the sleep problem
patients not taking other medications. On the night
by the research team. One may question, however, whether
following the first dose of 100 mg trazodone, their patients
there is a spillover effect from the initial (first 7 days) use of
had increased TST and stage 2 and decreased sleep latency
trazodone. Despite the fact that such an effect has never
and number of awakenings. When the dose was increased
been reported, similar results are often observed in
within 4 days to 400 – 600 mg nightly stage 4 and REM
crossover design protocols, even with controlled placebo,
latency increased in addition to sustained improvement of
as in our case. However, the polysomnographic data clearly
sleep variables observed after 1 day of treatment. We found
show the dissociation of subjective and objective results.
an insignificant decrease in stage 2 NREM sleep, but our
When placebo intake was associated with improved
findings were otherwise the same. After 1 week of trazodone
subjective scores, polysomnographic data showed declines.
100 mg treatment all sleep parameter improvements were
Objective sleep improvement declined within a short period
highly significant, with reduction in stage 1 sleep, number of
(maximum 15 days) in our population. These polygraphic
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
results support evidence of the beneficial effect of the
[5] Rascati K. Drug utilization review of concomitant use of specific
trazodone administration in these depressed patients.
serotonin reuptake inhibitors or clomipramine with antianxiety/sleep
It has been mentioned that the persistence of insomnia
medications. Clin Ther 1995;17(4):786 – 90.
[6] Muratatorio A, Maggini C, Coccanna G, Guazelli M. Polygraphic
may be responsible for recurrence of depressive symptoms,
study of the all night sleep pattern in neurotic and depressed patients
emphasizing the importance of treating poor sleep in these
treated with trazodone. In: Ban TH, Silvestrini B, editors. Trazodone,
patients. The insomnia may be related to the symptoms
modern problems in pharmacopsychiatry, vol. 9. Basel: Karger; 1974.
themselves, and to side effects related to SSRIs. Our study
indicates that subjective reports may not be a good indicator
[7] Montgomery J, Oswald I, Morgan K, Adam K. Trazodone enhances
of the severity of sleep disruption and that polysomno-
sleep on subjective quality but not objective duration. Br J ClinPharmacol 1983;16:139.
[8] Mouret J, Lemoine P, Minuit MP, et al. Effects of trazodone on the
It has been reported that trazodone causes less severe
sleep depressed subjects: a polygraphic study. Psychopharmacology
anticholinergic side effects than tricyclics. As a sedating
antidepressant, it has a short half-life. It is effective in
[9] Jacobsen FM. Low-dose trazodone as a hypnotic in patients treated
inducing and maintaining sleep throughout 5-week trials,
with MAOIs and other psychotropics: a pilot study. J Clin Psychiatry1990;51:298– 302.
but very little information is available about longer
[10] Metz A, Shader RI. Adverse interactions encountered when using
trazodone to treat insomnia associated with fluoxetine. Int Clin
In conclusion, trazodone 100 mg improved objective
measurements of sleep in adult female patients with
[11] Nierenberg A, Adler L, Peselow E, et al. Trazodone for antidepress-
moderate depression receiving low/normal dosages of
ant-associated insomnia. Am J Psychiatry 1994;151(7):1069 – 72.
SSRIs, even from the first administration of treatment. A
[12] Mc Cue RE, Georgotas A. Newer generation antidepressants and
lithium. In: Georgotas A, Cancro R, editors. Depression and mania: a
long-term study comparing the efficacy and adverse
comprehensive textbook. New York: Elsevier; 1988. p. 372 – 85.
reaction profiles of trazodone and of conventional
[13] Hamilton M. Development of a rating scale for primary depressive
hypnotics for antidepressant-associated insomnia is
illness. Br J Soc Clin Psychol 1967;6:278– 96.
[14] Buysse DJ, Reynolds III CF, Monk TH, et al. The Pittsburgh sleep
quality index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193 – 213.
[15] Vasar V, Appelberg B, Rimon R, Selvaratnam J. The effects of fluo-
xetine on sleep: a longitudinal, double-blind polysomnographic studyof healthy volunteers. Int Clin Psychopharmacol 1994;9(3):203 – 6.
[1] Kupfer DJ, Reynolds CF. Neurophysiologic studies of depression:
[16] Hendrickse WA, Roffward HP, Granneman BD, et al. The effects of
state of the art. In: Angst J, editor. The origins of depression: current
fluoxetine on the polysomnogram of depressed outpatients: a pilot
concepts and approaches. Berlin: Springer; 1983.
study. Neurophyschopharmacology 1994;10:85 – 91.
[2] Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances
[17] Triverdi MH, Hoffmann RF, Rush AJ, Armitage R. Effects of
and psychiatric disorders: an opportunity for prevention. J Am Med
fluoxetine on macro- and micro-analytic measures of sleep in patients
with major depression. Sleep Res 1997;26:304.
[3] Byerley WF, Reimherr FW, Wood DR, Grosser BJ. Fluoxetine, a
[18] Sharpley AL, Williamson DJ, Athenburrow ME, et al. The effects of
selective seretonin uptake inhibitor, for the treatment of outpatients
paroxetin and nefazadone on sleep: a placebo controlled trial.
with depression. J Clin Psychopharmacol 1988;8:112 – 5.
Psychopharmacology 1996;126(1):50 – 4.
[4] Kurz NM, Robinson DS. Monoamine oxidase inhibitors. In:
[19] Scharf MB, Sachais BA. Sleep laboratory evaluation of the effects and
Georgatos A, Cancro R, editors. Depression and mania: a compre-
efficacy of trazodone in depressed insomniac patients. J Clin
hensive textbook. New York: Elsevier; 1988.
Psychiatry 1990;51(Oct Suppl):13 – 17.
Audrey F. Saftlas Professor INSTITUTION AND LOCATION FIELD OF STUDY Positions and Employment 1979-1980 Research Associate, Michigan State Toxic Substance Control Commission, Lansing, MI Epidemiologist, Michigan Cancer Foundation Registry (SEER), Detroit, MI Epidemiologist (COSTEP), Occupational Studies Section, Environmental Epidemiology Branch, National Cancer Institute,
SAFETY DATA SHEET IDENTIFICATION OF THE PRODUCT AND OF THE MANUFACTURER Potassium tetrafluoroborate Registration number (ECHA) Classification categories / hazard indications Relevant identified uses of the substance or mixture and uses advised For the text of R-phrases/H-phrases and classification abbreviations Relevant identified uses of the substance or mixture: IDENTIFICATIO
 The effects of trazodone on sleep in patients treated
Hakan Kaynaka,*, Derya Kaynaka, Erbil Go¨zu¨kırmızıa, Christian Guilleminaultb
aDepartment of Neurology, Sleep Disorders Unit, Cerrahpasa Medical School, University of Istanbul, Cerrahpasa, 34303 Istanbul, Turkey
bStanford Sleep Disorders Clinic and Research Center, Stanford, CA, USA
Received 12 March 2003; received in revised form 25 June 2003; accepted 26 June 2003
Background and purpose: To evaluate the effects of trazodone on subjective and objective measures of sleep in depressed insomnia
patients treated with selective serotonin reuptake inhibitors (SSRIs). SSRIs can exacerbate or cause new insomnia while alleviating othersymptoms of depression. Trazodone has been reported to be an effective hypnotic for patients with antidepressant-associated insomnia.
The effects of trazodone on sleep in patients treated
Hakan Kaynaka,*, Derya Kaynaka, Erbil Go¨zu¨kırmızıa, Christian Guilleminaultb
aDepartment of Neurology, Sleep Disorders Unit, Cerrahpasa Medical School, University of Istanbul, Cerrahpasa, 34303 Istanbul, Turkey
bStanford Sleep Disorders Clinic and Research Center, Stanford, CA, USA
Received 12 March 2003; received in revised form 25 June 2003; accepted 26 June 2003
Background and purpose: To evaluate the effects of trazodone on subjective and objective measures of sleep in depressed insomnia
patients treated with selective serotonin reuptake inhibitors (SSRIs). SSRIs can exacerbate or cause new insomnia while alleviating othersymptoms of depression. Trazodone has been reported to be an effective hypnotic for patients with antidepressant-associated insomnia.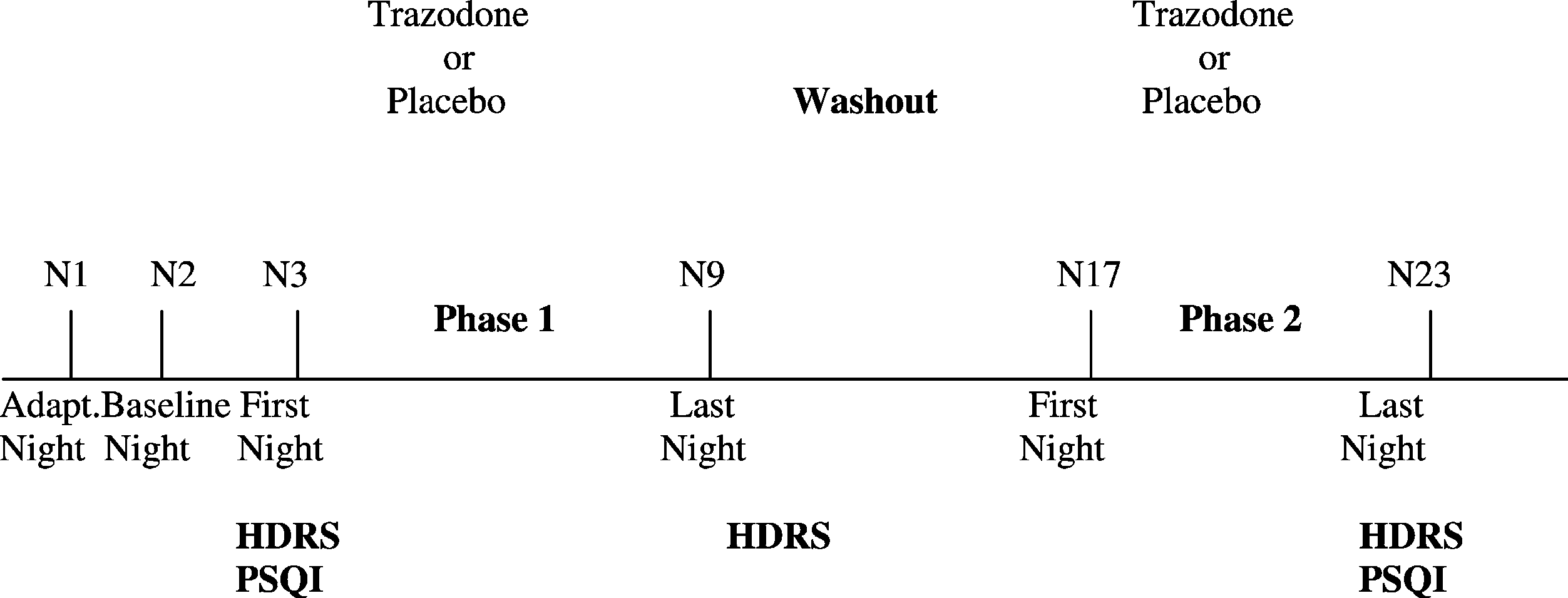 H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 1. Polysomnographic and clinical evaluation.
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 1. Polysomnographic and clinical evaluation.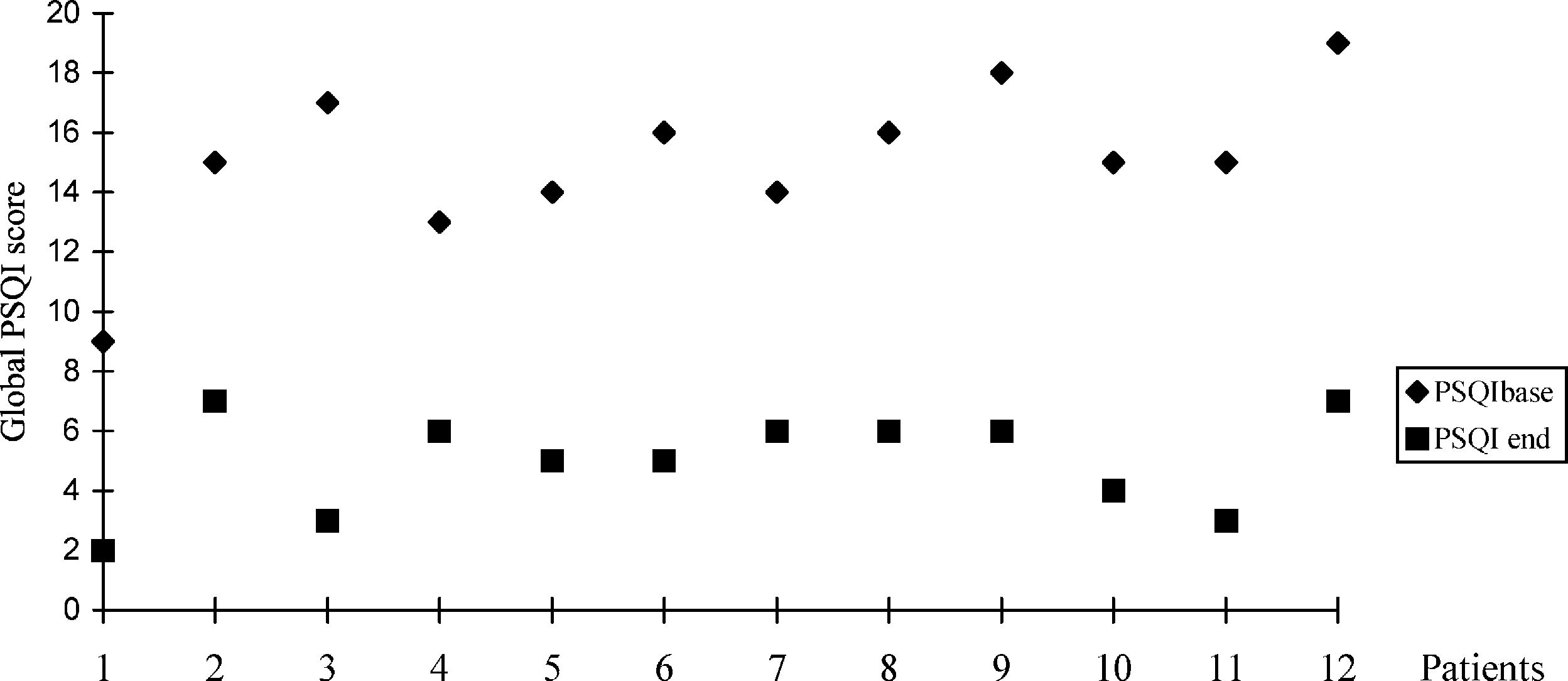 H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 2. Global PSQI scores of patients at the beginning and at the end of the study.
H. Kaynak et al. / Sleep Medicine 5 (2004) 15–20
Fig. 2. Global PSQI scores of patients at the beginning and at the end of the study.