Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients kamagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Interactions between masculinity-femininity and apparent health in face preferences
Interactions between masculinity-femininity and apparent health in face preferences
FG Smith1, BC Jones1, LM DeBruine1, AC Little2
1. Face Research Laboratory, School of Psychology, University of Aberdeen
2. Department of Psychology, University of Stirling
Corresponding author
Benedict C Jones, Face Research Laboratory,
School of Psychology, University of Aberdeen
Abstract
Consistent with Getty’s (2002) proposal that cues to long-term health and cues to
current condition are at least partly independent, recent research on human face
preferences has found divergent effects of masculinity-femininity, a cue to long-term
health, and apparent health, a cue to current condition. In light of this, we tested for
interactions between these two cues. Participants viewed composite images of opposite-
sex faces that had been manufactured in combinations of high and low apparent health
and masculinity-femininity. Preferences for masculinity in men’s faces and femininity in
women’s faces were stronger when judging the attractiveness of faces with high
apparent health than when judging the attractiveness of faces with low apparent health.
Similarly, preferences for high apparent health were stronger for judgments of masculine
men’s faces and feminine women’s faces than for judgments of feminine men’s faces
and masculine women’s faces, respectively. Interactions between apparent health and
masculinity-femininity when forming face preferences may function to optimize how
masculinity-femininity and apparent health are used to infer the quality of potential
mates and highlight the complexity and sophistication of the perceptual mechanisms
Keywords
masculinity; apparent health; faces; mate choice; integration; signal interactions
Introduction
Physical traits that are costly to develop and maintain may signal underlying quality (i.e.
long-term health), but may not necessarily signal current condition (i.e. absence of
disease, Getty, 2002). Because long-term health is associated with indirect benefits (e.g.
heritable immunity to infectious disease; Folstad and Karter, 1992), and absence of
disease is associated with direct benefits (e.g. reduced likelihood of contracting illness;
Welling et al., 2007a), both will be important for mate choice (Johnston et al., 1999;
Miller and Todd, 1998; Jones et al., 2005a). Interactions between these different signals
when forming face preferences may allow individuals to better infer the quality of
potential mates. Indeed, interactions among different signals of quality have been
reported in studies of non-human mate preferences and are thought to function to
provide more reliable information about the quality of potential mates (see Candolin,
Among men, facial masculinity is associated with good long-term health as assessed
from medical records (Rhodes et al., 2003) and incidence and duration of past illness
(Thornhill and Gangestad, 2006). Among women, feminine facial traits are also
associated with long-term health estimated from the incidence and duration of past
illness (Thornhill and Gangestad, 2006) and with indices of fertility (e.g. trait hormone
levels, Law Smith et al., 2006). Other facial cues, such as pallor, signal current condition
(Jones, et al., 2005b). Consistent with the proposal that preferences for these different
types of cues may be at least partly independent, preferences for apparent health and
masculinity in male faces are unrelated among women (Boothroyd et al., 2005).
Additionally, changes in women’s hormonal profiles during the menstrual cycle affect
preferences for apparent health and masculinity in different ways: aversions to facial
cues of illness are strongest during the luteal phase of the menstrual cycle (Jones et al.,
2005a, 2005b), while preferences for masculinity are strongest around ovulation
(Penton-Voak et al., 1999, Johnston et al., 2001, Jones et al., 2005a; Welling et al.,
2007b). Indeed, cyclic variation in women’s preferences for apparent health and
masculinity in men’s faces are independent (Jones et al., 2005a). Collectively, these
findings suggest that preferences for cues to long-term health and current condition are
at least partly independent, raising the possibility that masculinity-femininity and
apparent health signal different aspects of mate quality (see, e.g. Boothroyd et al., 2005
and Jones et al., 2005a for discussion).
Most previous studies of facial attractiveness have manipulated faces along only single
dimensions (e.g. Rhodes et al., 2001; Perrett et al., 1998; Penton-Voak et al., 1999;
Jones et al., 2005a; DeBruine et al., 2006). However, recent research on face
perception has demonstrated that different types of facial cues can have effects on
attractiveness that interact. For example, fearful expressions are perceived as more
intense with averted gaze than direct gaze (Adams and Kleck, 2003) and preferences
for physically attractive faces are stronger for faces that are smiling at the viewer than
for faces that are smiling away from the viewer (Jones et al, 2006). While these studies
demonstrate interactions between social cues (e.g. gaze direction) and either physical
cues (e.g. physical attractiveness) or other social cues (e.g. emotional expressions), we
know of no studies of face preferences that have investigated interactions between
different physical cues. If cues to current health modulate preferences for masculinity-
femininity and vice versa, this would suggest that interactions between information from
different physical signals may function to optimize inferences about the quality of
In light of the above, we tested if women’s preferences for masculinity are stronger when
judging the attractiveness of male faces displaying cues associated with good current
condition (i.e. high apparent health) than when judging the attractiveness of male faces
displaying cues associated with current illness (i.e. low apparent health). We also tested
if women’s preferences for apparent health are stronger when judging the attractiveness
of masculine male faces than when judging the attractiveness of feminine male faces.
Additionally, we carried out equivalent tests for men’s preferences for femininity and
apparent health in female faces. Following previous studies of preferences for
masculinity-femininity (e.g. Perrett et al., 1998), cues of apparent health (Jones et al.,
2005a, 2005b), and interactions between physical attractiveness and facial expressions
(Jones et al., 2006), participants judged the attractiveness of composite (i.e. prototype)
faces that had been systematically manipulated using computer graphic methods.
Masculine and feminine versions of healthy and unhealthy male and female composite
faces were manufactured using well-established and validated computer graphic
methods for systematically varying the appearance of face images (Perrett et al., 1998,
Jones et al., 2005b). First, 60 male and 60 female full-color face images (19-24 years
old) were rated for apparent health on a scale of 1 (low health) – 7 (high health) by 20
raters (17-26 years old; 10 male, inter-rater agreement: Cronbach’s !=0.82). Next, a
‘high apparent health’ female composite face was manufactured by averaging the
shape, color and texture information from the 15 female face images with the highest
rated health. To do this, 179 facial landmarks were placed on each face image. The
computer algorithm then calculates the mean X and Y coordinates for each point (to
calculate the average face shape) and the mean RGB value for each pixel (to calculate
the average color information). A wavelet-based algorithm was then used to apply
representative realistic texture details to the image. For technical details about this
process, see Tiddeman, Perrett and Burt (2001). A ‘low apparent health’ female
composite face was then manufactured by averaging the shape, color and texture
information from the 15 female face images with the lowest rated health. High and low
apparent health male composite faces were then constructed using the same methods
that were used to manufacture female composites. Previous studies have shown that
high and low apparent health composites manufactured in this way differ reliably in
apparent health (Jones et al., 2004; Jones et al., 2005b).
Masculine versions of each of these high and low apparent health composites were then
manufactured by applying +50% of the vector differences in 2D shape between a male
and female prototype face. Feminine versions of each of these high and low apparent
health composites were then manufactured by applying -50% of the differences in 2D
shape between a male and female prototype face. Altering sexual dimorphism of 2D
face shape in this way does not alter other aspects of facial appearance (e.g. identity).
This method for manipulating sexual dimorphism of 2D shape in face images has been
widely used in studies of face preferences (e.g. Jones et al., 2007; Perrett et al., 1998;
Penton-Voak et al., 1999). Previous studies have also shown that faces masculinized
and feminized in this way differ reliably in perceived masculinity (DeBruine et al., 2006;
Welling et al., 2008) and produce preferences equivalent to those from faces
manipulated in masculinity using other methods (DeBruine et al., 2006).
Finally, all images were scaled and rotated to a standard interpupillary distance.
Masculine and feminine versions of both male and female high and low apparent health
In total, this method created four male composite faces (a healthy-looking masculine
male composite, a healthy-looking feminine male composite, an unhealthy-looking
masculine male composite, and an unhealthy-looking feminine male composite) and four
corresponding female composite faces (a healthy-looking masculine female composite,
a healthy-looking feminine female composite, an unhealthy-looking masculine female
composite, and an unhealthy-looking feminine female composite).
Participants in the lab sample were 354 women (mean age =21.1,SD=5.8) and 144 men
(mean age =21.1,SD=4.6). All participants in the lab sample were undergraduate
students at the University of Aberdeen who completed the experiment on individual
computers in the lab in groups of 4 to 40.
Additionally, 5564 women (mean age = 20.4, SD = 2.7) and 3632 men (mean age =
21.2, SD = 2.7) completed the experiment through an online interface. Previous studies
have shown that online and laboratory studies of face preferences have produced
consistent results (Jones et al., 2005b; Jones et al., 2007; Welling et al., 2007c; Wilson
and Daly, 2004). Responses from duplicate IP (internet protocol) addresses from the
In both the lab and web samples, participants were presented with four pairs of
opposite-sex faces that differed in either masculinity-femininity or apparent health, but
that were matched in other regards, and were asked to indicate which face is more
attractive in each image pair. Participants were also asked to indicate the strength of
their preference by choosing from the options ‘much more attractive’, ‘more attractive’,
‘somewhat more attractive’ and ‘slightly more attractive’. Thus, preferences for
masculinity versus femininity were assessed under two conditions: on one trial where
masculinized and feminized versions of a healthy-looking face were presented and on
another trial where masculinized and feminized versions of an unhealthy-looking face
were presented. Similarly, preferences for apparent health were also assessed under
two conditions: on one trial where high and low apparent health versions of a
masculinized face were presented and on another trial where high and low apparent
health versions of a feminized face were presented. Trial order and the side of the
screen on which any particular image was shown were fully randomized.
Following previous studies of face preferences (e.g. Buckingham et al., 2006; Jones et
al., 2005b; 2005c; Jones et al., 2007), responses on the face preference tests were
0 = feminine male, masculine female, or low apparent health was judged ‘much more attractive’
1 = feminine male, masculine female, or low apparent health was judged ‘more attractive’
2 = feminine male, masculine female, or low apparent health was judged ‘somewhat more attractive’
3 = feminine male, masculine female, or low apparent health was judged ‘slightly more attractive’
4 = masculine male, feminine female, or high apparent health was judged ‘slightly more attractive’
5 = masculine male, feminine female, or high apparent health was judged ‘somewhat more attractive’
6 = masculine male, feminine female, or high apparent health was judged ‘more attractive’
7 = masculine male, feminine female, or high apparent health was judged ‘much more attractive’
Thus, participants provided four preference scores: (1) preference for masculinity versus
femininity in faces with high apparent health, (2) preference for masculinity versus
femininity in faces with low apparent health, (3) preference for high versus low apparent
health in masculinized faces, and (4) preference for high versus low apparent health in
Following many previous studies that have used composite images to investigate face
preferences (e.g. Perrett et al., 1998; Perrett, May and Yoshikawa, 1994; Jones et al.,
2006), individual raters served as the unit of analysis in all analyses. Paired-samples t-
tests were used to compare preferences for high versus low apparent health in
masculinized and feminized faces and to compare preferences for masculinity versus
femininity in faces with high and low apparent health.
In both the lab and web samples, preferences for high apparent health were stronger
when judging masculinized male faces than when judging feminized male faces (lab:
t353=2.73, p=.007; web: t5563=11.28, p<.001) and when judging feminized female faces
than when judging masculinized female faces (lab: t143=4.42, p<.001; web: t3631=26.25,
p<.001). These data are summarized in Figure 2.
Next, health preference scores were compared to the chance value of 3.5 (indicating no
preference for either face in a pair) using one-sample t-tests. In both samples, male and
female participants preferred high apparent health in both masculinized and feminized
opposite-sex faces (lab: all t>23, p<.001; web: all t>87, p<.001).
Masculinity-femininity Preferences
In both the lab and web samples, preferences for masculinity were stronger when
judging male faces with high apparent health than when judging male faces with low
apparent health (lab: t353=4.87, p<.001; web: t5563=13.92, p<.001). Preferences for
femininity were stronger when judging female faces with high apparent health than when
judging female faces with low apparent health (lab: t143=8.41, p<.001; web: t3631=38.06,
p<.001). These data are summarized in Figure 3.
Next, these preference scores were compared to the chance value of 3.5 (indicating no
preference for either face in a pair) using one-sample t-tests. Male participants preferred
femininity in both healthy and unhealthy female faces (lab: both t>6, p<.001; web: both
t>33, p<.001). Female participants preferred masculinity only in healthy male faces (lab:
t=5.44, p<.001; web: t=13.1, p<.001). Female participants in the lab study showed no
significant preference for masculinity or femininity in unhealthy male faces (t=0.19,
p=.853), although female participants in the web sample tended to prefer masculinity in
unhealthy male faces (t=1.91, p=.056).
Note that all significant effects reported in our Results would be robust to Bonferroni
Discussion
In both the lab and web samples, preferences for masculinity in men’s faces and
femininity in women’s faces were stronger when judging the attractiveness of faces with
high apparent health than when judging the attractiveness of faces with low apparent
health. Similarly, in both samples, preferences for high apparent health were stronger
when judging the attractiveness of masculine male faces and feminine female faces
than when judging the attractiveness of feminine male faces and masculine female
faces, respectively. Consistent with our hypotheses, these findings show that apparent
health modulates preferences for exaggerated sex-typical features in opposite-sex faces
(and vice versa). Previous studies of face preferences have shown interactions between
information from changeable social cues, such as gaze direction and expression, and
physical characteristics, such as physical attractiveness (Jones et al., 2006) and sex of
face (Conway et al., 2008). Complementing these findings, here we show interactions
between information from different physical cues when forming face preferences.
It is important to note that participants could not use the masculinity-femininity
dimension to discriminate between faces on trials where they were choosing between
healthy and unhealthy faces, since the healthy and unhealthy faces were matched in
terms of masculinity-femininity (i.e. were healthy and unhealthy versions of the same
face image). Similarly, participants could not use apparent health to discriminate
between faces on trials where they were choosing between feminine and masculine
faces, since the feminine and masculine faces were matched in terms of apparent
health. Consequently, stronger preferences for masculinity (in men’s faces) and
femininity (in women’s faces) on trials where the faces possessed high apparent health
than on trials where the faces possessed low apparent health and stronger preferences
for apparent health on trials where the faces were masculinized male faces or feminized
female faces demonstrate interactions between apparent health and masculinity-
femininity when forming face preferences. Furthermore, additive effects of these cues
cannot explain differences in the strength of such preferences between conditions.
Getty (2002) proposed that traits signaling underlying condition (i.e. long-term health) do
not necessarily signal current condition, and vice versa. Subsequent studies of face
preferences have suggested that preferences for these different types of facial cues are
also, at least partly, independent (Jones et al., 2005a, 2005b; Boothroyd et al., 2005).
Since both underlying and current condition are important for mate choice, however,
interactions between information about both types of health may allow people to
optimize the possible benefits of their mate choices. Indeed, our findings complement
those for interactions among multiple signals of quality in non-human mate preferences,
which are thought to function to increase the reliability of the information that is available
about the quality of potential mates (see Candolin, 2003 for a review of this issue). For
example, the sex hormones that influence masculinity-femininity of face shape can also
be immunosuppressants (Thornhill and Gangestad, 1999). Thus, modulating the
strength of preferences for masculinity-femininity according to the current condition of
the target individual may promote mating with individuals who are able to maintain good
current condition despite this immunosuppression. In other words, considering the
extent to which individuals appear able to maintain good current condition despite the
immunosuppressive effects of sex hormones may be important for inferring mate quality.
Previous studies have found wide variation in the strength of preferences for masculinity
in male faces (see DeBruine et al., 2006 and Rhodes, 2006 for reviews). While some
researchers have suggested differences among studies can be attributed to differences
in the methods used to manipulate masculinity in face images (see DeBruine et al., 2006
and Rhodes, 2006 for reviews), DeBruine et al. (2006) found that different methods
produce the same preferences for masculinity in men’s faces. Other researchers have
attributed these differences to systematic variation among women in the extent to which
masculinity is considered attractive (DeBruine et al., 2006; Little et al., 2002). The
current study demonstrates that characteristics of the faces being judged, such as
apparent health, can also influence the extent to which masculinity is considered
attractive and highlights the complexity and sophistication of the perceptual mechanisms
Acknowledgments
Anthony Little is supported by a Royal Society University research Fellowship.
References
Adams, R. B., & Kleck, R. E. (2003). Perceived gaze direction and the processing of
facial displays of emotion. Psychological Science, 141, 644-647.
Boothroyd, L. G., Jones, B. C., Burt, D. M., Cornwell, R. E., Little, A. C., Tiddeman, B. P.
& Perrett, D. I. (2005). Facial masculinity is related to perceived age but not
perceived health. Evolution and Human Behavior, 26, 417-431.
Candolin, U. (2003). The use of multiple cues in mate choice. Biological Review, 78,
Conway, C. A., Jones, B. C., DeBruine, L. M., & Little, A. C. (2008). Evidence for
adaptive design in human gaze preference. Proceedings of the Royal Society of London B, 275, 63-69.
DeBruine, L. M., Jones, B. C., Little, A. C., Boothroyd, L. G., Perrett, D. I., Penton-Voak,
I. S., Cooper, P. A., Penke, L., Feinberg, D. R. & Tiddeman, B. P. (2006). Correlated
preferences for facial masculinity and ideal or actual partner’s masculinity.
Proceedings of the Royal Society of London B, 273, 1355-1360.
Folstad, I., & Karter, A. J. (1992). Parasites, bright males and the immunocompetence
handicap. American Naturalist, 139, 603 – 622.
Getty, T. (2002). Signaling health versus parasites. The American Naturalist, 159, 363-
Johnston, V. S., Hagel, R., Franklin, M., Fink, B., & Grammer, K. (2001). Male facial
attractiveness: evidence for a hormone-mediated adaptive design. Evolution and Human Behavior, 22, 251-267.
Jones, B. C., DeBruine, L. M., Little, A. C., Conway, C. A., Welling, L. L. M. & Smith, F.
G. (2007). Sensation seeking and men's face preferences. Evolution and Human Behavior, 28, 439-446.
Jones, B. C., DeBruine, L. M., Little, A. C., Conway, C. A., & Feinberg, D. R. (2006).
Integrating gaze direction and expression in preferences for attractive faces.
Psychological Science, 17, 588-591.
Jones, B. C., DeBruine, L. M., Little, A. C., Conway, C. A., Welling, L. L. M., & Smith,
F. G. (2007). Sensation seeking and men’s face preferences. Evolution and Human Behavior, 28, 439-446.
Jones, B. C., Little, A. C., Boothroyd, L. G., DeBruine, L. M., Feinberg, D. R., Law Smith,
M. J., Cornwell, R. E., Moore, F. R. & Perrett, D. I. (2005a). Commitment to
relationships and preferences for femininity and apparent health in faces are
strongest on days of the menstrual cycle when progesterone level is high.
Hormones and Behavior, 48, 283-290.
Jones, B. C., Perrett, D. I., Little, A. C., Boothroyd, L. G., Cornwell, R. E., Feinberg, D.
R., Tiddeman, B. P., Whiten, S., Pitman, R. M., Hillier, S. G., Burt, D. M., Stirrat, M.
R., Law Smith, M. J. & Moore, F. R. (2005b). Menstrual cycle, pregnancy and oral
contraceptive use alter attraction to apparent health in faces. Proceedings of the Royal Society of London B, 272, 347-354.
Jones, B. C., Little, A. C., Boothroyd, L. G., Feinberg, D. R., Cornwell, R. E., DeBruine,
L. M., Roberts, S. C., Penton-Voak, I. S., Law Smith, M. J., Moore, F. R., Davis, H.
P. & Perrett, D. I. (2005c). Women’s physical and psychological condition
independently predict their preference for apparent health in faces. Evolution and Human Behavior, 26, 451-457.
Jones, B. C., Little, A. C., Burt, D. M. & Perrett, D. I. (2004). When facial attractiveness
is only skin deep. Perception, 33, 569-576.
Law Smith, M. J., Perrett, D. I., Jones, B. C., Cornwell, R. E., Moore, F. R., Feinberg, D.
R., Boothroyd, L. G., Durrani, S. J., Stirrat, M. R., White, S. R., Pitman, R. M. &
Hillier, S. G. (2006). Facial appearance is a cue to oestrogen levels in women.
Proceedings of the Royal Society of London B, 10, 1-6.
Little, A. C., Jones, B. C., Penton-Voak, I. S., Burt, D. M., & Perrett, D. I. (2002).
Partnership status and the temporal context of relationships influence human female
preferences for sexual dimorphism in male face shape. Proceedings of the Royal Society of London B, 269, 1095-1103.
Miller, G. F., & Todd, P. M. (1998). Mate choice turns cognitive. Trends in Cognitive Sciences, 2, 190-198.
Penton-Voak, I. S., Perrett, D. I., Castles, D. L., Kobayashi, T., Burt, D. M., Murray, L. K.
& Minamisawa, R. (1999). Menstrual cycle alters face preference. Nature, 399, 741-
Perrett, D. I., Lee, K. J., Penton-Voak, I. S., Rowland, D. R., Yoshikawa, S., Burt, D. M.,
Henzi, S. P., Castles, D. L. & Akamatsu, S. (1998). Effects of sexual dimorphism on
facial attractiveness. Nature, 394, 884-887.
Perrett, D. I., May, K. A., & Yoshikawa, S. (1994). Facial shape and judgments of female
attractiveness. Nature, 368, 239-242.
Rhodes, G. (2006). The evolutionary psychology of facial beauty. Annual Review of Psychology, 57, 199-226.
Rhodes, G., Chan, J., Zebrowitz, L. A., & Simmons, L. W. (2003). Does sexual
dimorphism in human faces signal health? Proceedings of the Royal Society of London B, 270, S93-S95.
Rhodes, G., Zebrowitz, L., Clark, A., Kalick, S. M., Hightower, A., & McKay, R. (2001).
Do facial averageness and symmetry signal health? Evolution and Human
Thornhill, R., & Gangestad, S. W. (1999). Facial attractiveness. Trends in Cognitive Sciences, 3, 452-460.
Thornhill, R. & Gangestad, S. W. (2006). Facial sexual dimorphism, developmental
stability, and susceptibility to disease in men and women. Evolution and Human Behavior, 27, 131-144.
Tiddeman, B. P., Perrett, D. I., & Burt, D. M. (2001). Prototyping and transforming facial
textures for perception research. IEEE Computer Graphics and Applications, 21, 42-
Welling, L. L. M., Conway, C. A., DeBruine, L. M., & Jones, B. C. (2007a). Perceived
vulnerability to disease predicts variation in preferences for apparent health in faces.
Journal of Cultural and Evolutionary Psychology, in press.
Welling, L. L. M., Jones, B. C., DeBruine, L. M., Conway, C. A., Law Smith, M. J., Little,
A. C., Feinberg, D. R., Sharp, M. & Al-Dujaili, E. A. S. (2007b). Raised salivary
testosterone in women is associated with increased attraction to masculine faces.
Hormones and Behavior, 52, 156-161.
Welling, L. L. M., Jones, B. C. & DeBruine, L. M. (2008). Sex drive is positively
associated with women's preferences for sexual dimorphism in men's and women's
faces. Personality and Individual Differences, 44, 161-170.
Wilson, M., & Daly, M. (2004). Do pretty women inspire men to discount the future?
Proceedings of the Royal Society of London B, 271, S177-S179. Figure 1: Face stimuli used in the experiment. Masculine male and feminine female
faces with high apparent health (a), feminine male and masculine female faces with high
apparent health (b), masculine male and feminine female faces with low apparent health
(c), and feminine male and masculine female faces with low apparent health (d) were
presented in combinations such that each face pair differed on only one aspect (health
Figure 2: Preferences for apparent health when masculinity-femininity is varied in male
and female faces. Bars show means and SEMs. In both the lab (a) and web (b)
samples, preferences for high apparent health were stronger for judgments of masculine
male and feminine female faces, compared to feminine male and masculine female
faces. Male faces were judged by female participants and female faces were judged by
male participants. Note that SEMs for the lab sample are extremely small because of the
Figure 3: Preferences for masculinity-femininity when apparent health is varied in male
and female faces. Bars show means and SEMs. In both the lab (a) and web (b)
samples, preferences for masculinity in male faces and femininity in female faces were
stronger for judgments of faces with high apparent health, compared to faces with low
apparent health. Male faces were judged by female participants and female face were
judged by male participants. Note that SEMs for the lab sample are extremely small
Martina Lambert Head of Marketing and Communications LBBW Bank CZ a.s. Telephone +420 224 406 233 Telefax +420 224 406 483 [email protected] www.LBBW.cz LBBW offers IQ Account for Entrepreneurs LBBW enhances its product portfolio with product especially designed for SME’s – IQ Account for Entrepreneurs IQ Account for Entrepreneurs is a package of com
Uma guerra entre os dois países, além de massacrar, possivelmente, milhares de árabes e israelenses, bem como norte-americanos, elevaria o preço do gás e do petróleo a um nível inimaginável, catapultado para uma cifra superior a US$ 250, ou mesmo chegar US$ 500 o barril, interrompendo o comércio e causando um cataclismo na economia mundial, já abalada e deprimida, desde 2007-2008, pel
 Figure 1: Face stimuli used in the experiment. Masculine male and feminine female
Figure 1: Face stimuli used in the experiment. Masculine male and feminine female 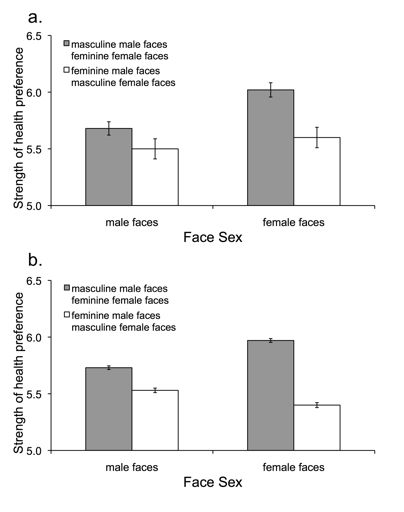 Figure 2: Preferences for apparent health when masculinity-femininity is varied in male
Figure 2: Preferences for apparent health when masculinity-femininity is varied in male 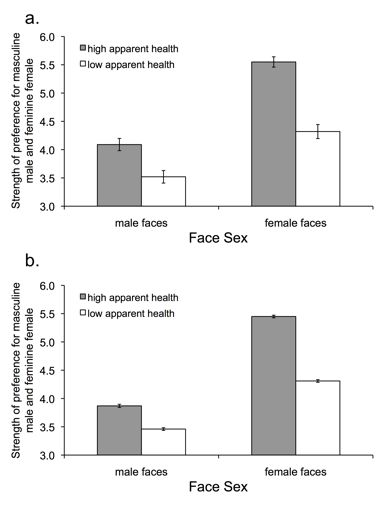 Figure 3: Preferences for masculinity-femininity when apparent health is varied in male
Figure 3: Preferences for masculinity-femininity when apparent health is varied in male