Levitra has a minimal amount of contraindications which has increased its popularity priligy uk You can buy quality certified medications from us at an affordable price.
Pii: s0006-3223(99)00229-2
Effective Neuroleptic Medication Removes PrepulseInhibition Deficits in Schizophrenia Patients
Almut I. Weike, Ulrike Bauer, and Alfons O. Hamm
Background: The magnitude of the startle eyeblink re-
in focussing their attention to relevant stimuli. This is
sponse is reduced if the startle eliciting stimulus is shortly
indicated by longer reaction times in cross-modal reaction
preceded by another stimulus. There is evidence that
time tasks or impairments in the Continuous Performance
schizophrenia patients exhibit impairments in this so-
Task (for reviews see Braff 1993; Braff et al 1991;
called prepulse inhibition. Our study investigated whether
Nuechterlein and Dawson 1984). Because schizophrenia
prepulse inhibition is affected by neuroleptic drug treat-
patients are unable to screen out irrelevant stimuli, they
ment as is suggested by animal research.
seem to be vulnerable to stimulus inundation, particularly
Methods: Prepulse inhibition was tested in five unmedi-
if external stimuli are presented in rapid succession. In
cated and 20 medicated inpatients with schizophrenia, and
such conditions the response to a second stimulus has to be
inhibited or attenuated to protect the processing of the first
Results: The unmedicated schizophrenia patients showed
stimulus. Schizophrenia patients reliably exhibit a deficit
a strong impairment of sensorimotor gating as indexed by
in effectively inhibiting the processing of a second disrup-
the absence of prepulse inhibition. By contrast, the med-
tive stimulus, as assessed by various tasks. These include
icated patients showed a pronounced prepulse inhibitionthat did not differ from that of the normal controls. There
visual backward-masking performance (Braff et al 1991;
was a substantial covariation between the rated severity of
Rund 1993) and the decline in amplitude of the P50
the positive syndrome and the amount of prepulse inhibi-
component of the event-related potential to the second of
tion—i.e., the patients whose positive symptoms were
a pair of clicks (Freedman et al 1987). The modulation of
rated as more severe showed less prepulse inhibition.
the startle response by weak prestimulation has also been
Conclusions: These data suggest that the impaired sen-
used to assess these deficits in information processing in
sorimotor gating of schizophrenia patients is not a stablevulnerability indicator, but may rather be related to the
The measurement of startle modulation to study these
positive syndrome and may be improved by treatments
dysfunctions has a number of advantages. First, the startle
with neuroleptic medication. Biol Psychiatry 2000;47:
reflex is relatively free from voluntary control and requires
61–70 1999 Society of Biological Psychiatry
minimal effort from the subject. Second, startle modula-tion is particularly amenable to animal modeling because
Key Words: Schizophrenia, prepulse inhibition, sensori-
it occurs in infrahuman species as well. Third, the neural
motor gating, startle eyeblink, neuroleptic medication,
circuits mediating evocation and modulation of the acous-
tic startle response are increasingly well understood(Davis 1997). Finally, startle modulation is influenced bypsychoactive drugs and by various manipulations of neu-
Introduction
rotransmitter systems (see Koch and Schnitzler 1997),
Dysfunctions in attention and information processing whichmayallowonetotentativelylinkstartlemodulation
have long been considered a hallmark of schizophre-
deficits in schizophrenia patients to underlying neurobio-
nia. By using a wide range of different experimental
techniques to quantify these dysfunctions, it has been
The magnitude of the startle response—a fast protective
demonstrated that schizophrenia patients have difficulties
reflex to an unexpected intense stimulus with rapid on-set—is reduced if weak sensory events (prepulses) arepresented at brief intervals (i.e., between 30 and 500 msec)
From the Department of Psychology, University of Greifswald, Greifswald (AIW,
prior to the startle-eliciting stimuli. This phenomenon is
AOH) and the Department of Psychiatry, University of Giessen, Giessen (UB),
called prepulse inhibition (PPI) and has been observed
Address reprint requests to Prof. Dr. Alfons Hamm, Ernst-Moritz-Arndt-Universi-
across a wide range of stimulus intensities and modalities
taet Greifswald, Institut fu¨r Psychologie, Franz-Mehring-Strasse 47, 17487
in animals (Hoffman 1997; Hoffman and Ison 1980, 1992)
Received March 5, 1999; revised July 28, 1999; accepted August 10, 1999.
and humans (see reviews by Anthony 1985; Filion et al
1998; Graham 1975). Prepulse inhibition is very robust
normal controls, there was no difference in PPI between
and occurs in 90 –100% of normal subjects who exhibit a
the groups, if an insignificant (to be ignored) tone stimulus
normal startle eyeblink response. Prepulse inhibition
preceded the startle-eliciting noise burst (Dawson et al
seems to be a rather automatic and low-level phenomenon,
1993). Reduced PPI in schizophrenia patients compared
since it can be obtained during sleep (Silverstein et al
with controls was only observed when individuals were
1980) and at the very first presentation of the lead
instructed to selectively attend to the prepulse stimulus.
stimulus. According to Graham (1975, 1992) and Braff
These findings were recently replicated by Hazlett and
and colleagues (Braff 1985; Braff et al 1991; Geyer and
coworkers comparing schizophrenia patients during the
Braff 1987), PPI may reflect the action of a sensorimotor
period of washout with normal volunteers; again, normal
gating system that operates to protect early preattentive
controls exhibited stronger PPI following the to-be-at-
processing of a weak stimulus (prepulse) by inhibiting or
tended tone, compared with the to-be-ignored tone, at the
attenuating the disruptive effects of the intense startle-
120-msec lead interval, while schizophrenia patients failed
to show such attentional modulation of startle inhibition
Braff and coworkers were the first to demonstrate that
schizophrenia patients have a deficit in this sensorimotor
One reason for the differences between the results of
gating mechanism (Braff et al 1978). In that study, a
Braff and collaborators and those obtained by Dawson et
continuous mild tone (71 dB) served as the prepulse and a
al might be that the instruction to ignore a prepulse
burst of white noise as the startle stimulus. Inpatients with
stimulus is not completely comparable to the condition
schizophrenia showed impaired PPI relative to normal
where individuals process the prepulse passively—i.e.,
controls, especially at the 60- and 120-msec lead intervals.
without any specific task to allocate their attention either
These findings were replicated and extended by two
towards or away from that stimulus. In addition to these
additional studies, showing that reduced PPI in inpatients
procedural differences, the severity of psychopathology
with schizophrenia can also be obtained with a tactile
and medication status of the schizophrenia patient samples
startle-eliciting stimulus (Braff et al 1992) and with
varied substantially across studies. Dawson and colleagues
different prepulse intensities, ranging from 75 to 90 dB
studied relatively asymptomatic schizophrenia outpatients
(Grillon et al 1992). Deficient PPI was also found for
who were either off all medication or on a low to moderate
inpatients and outpatients diagnosed as having a schizo-
dose of neuroleptic medication (Dawson et al 1993). By
typal personality disorder (Cadenhead et al 1993) and for
contrast, Braff and collaborators tested schizophrenia in-
college students scoring high on perceptual aberration
patients treated with relatively high doses of antipsychotic
(Simons and Giardina 1992). Moreover, Swerdlow and
medication (chlorpromazine equivalents varied in a range
coworkers found reduced PPI in individuals who were
of 1640 to 2245 mg between studies).
classified as psychosis-prone based on theoretically and
Evidence from animal experimentation suggests that it
empirically derived Minnesota Multiphasic Personality
is unlikely that neuroleptic medication might induce def-
Inventory (MMPI) criteria (Swerdlow et al 1995a). These
icits in PPI. By contrast, PPI deficits induced by apomor-
data suggest that the deficit in the sensorimotor gating
phine can be removed by haloperidol, which blocks the
mechanism might be a trait-linked vulnerability for devel-
dopamine D2 receptors (Koch and Bubser 1994; Mans-
oping thought disorders or cognitive fragmentation, symp-
bach et al 1988). Moreover, PPI deficits induced by the
toms characteristic of schizophrenia disorders (Braff 1993;
noncompetitive NMDA antagonist phencyclidine are re-
versed by clozapine (Bakshi et al 1994). These substances
The relationship between reduced PPI and psychosis
are frequently used as typical and atypical antipsychotic
proneness in “normal” volunteers, however, is not a
drugs in humans. Findings such as these have been
reliable finding. In three studies, no differences in PPI
incorporated into an animal model for PPI deficits which
were found for individuals scoring high or low on
states that the nucleus accumbens is the core structure in
perceptual aberration (Blumenthal and Creps 1994;
the regulation of PPI in the context of dopaminergic and
Cadenhead et al 1996; Lipp et al 1994). Strikingly,
glutamatergic dysregulations (for reviews see Geyer et al
although individuals scoring high on perceptual aberra-
1990; Koch and Schnitzler 1997; and Swerdlow et al
tion and magical ideation also scored higher on the
MMPI psychoticism subscale and showed more mild
These animal data suggest that neuroleptic drugs might
psychotic symptoms as assessed by clinical interview,
not induce but on the contrary remove deficits in PPI in
the PPI of these subjects did not differ from that of a
schizophrenia patients. To our knowledge, there is no
control group (Cadenhead et al 1996).
study that has systematically tested the influence of
Moreover, even when clinically diagnosed but relatively
antipsychotic medication on PPI in humans. Thus the
asymptomatic schizophrenia patients were compared with
purpose of the present experiment was to assess the
amount of PPI in schizophrenia patients who were either
Table 1. Unmedicated and Medicated Schizophrenia Patients’
without any medication or were treated with either typical
Scores on the Positive, Negative, and GeneralPsychopathology Scales of the Positive and Negative
or atypical antipsychotic drugs. In contrast to animal
experimentation, where the dose-dependent influence of asingle drug can be tested systematically, medication in the
clinic is predominantly used to reduce the patients’ psy-
chopathology. Generally, the dose and type of psychoac-
tive medication are adjusted to the severity of the patients’
symptoms. Therefore, the covariations between status of
medication, severity of symptoms, and PPI were assessedin an exploratory analysis in our sample of schizophreniapatients. Stimulus Materials and Physiological Recording
The acoustic startle-eliciting stimulus was a 50-msec burst of 105dB[A] white noise generated by a Coulbourn Instruments (Allen-town, PA) S81-02 and gated through a Coulbourn S82-24
Methods and Materials
amplifier. Prepulse stimuli were 1000-Hz tones with a duration
of 20 msec and an intensity of 85 dB[A], generated by a Belco(New Castle, DE) audio generator. Startle and prepulse stimuli
Twenty-seven schizophrenia inpatients (10 women) participated
were both presented binaurally through headphones (Steintron,
in the experiment. The patients were diagnosed as having
Conrad, Germany). The eyeblink component of the startle reflex
schizophrenia (in 15 cases a paranoid subtype was diagnosed; for
was measured by recording the electromyogram (EMG) from the
the other patients a disorganized subtype (n ϭ 2), a residual
orbicularis oculi muscle beneath the left eye using miniature
schizophrenia (n ϭ 5), and a schizoaffective disorder mainly
Ag/AgCl electrodes (Sensor Medics, Yorba Linda, CA) filled
schizophrenic (n ϭ 5) was diagnosed) according to criteria from
with Beckman electrolyte (Marquette, Milwaukee). The raw
the DSM-III-R (American Psychiatric Association 1987) or from
signal was amplified with a Coulbourn S75-01 bioamplifier,
the ICD-10 (World Health Organization 1992), respectively.
filtered through a bandpass of 90 –1000 Hz, and digitized at 1
Seven schizophrenia patients (three women) were tested imme-
kHz for 500 msec, beginning 100 msec before the onset of the
diately following their admission to the hospital before receiving
any neuroleptic medication. Five of these patients had their firstpsychotic episode and had not been medicated before. The othertwo patients were neuroleptic-free for at least 6 months. Patients
in a period of washout were explicitly not included in the study.
After the participant gave informed consent, the physiological
Twenty patients (seven women) were tested after being treated
sensors were attached while the participant reclined in a com-
with neuroleptic medication for 11 weeks on average (range:
fortable chair. Each person was instructed that a series of tones
2– 41). Eleven patients (five women, seven paranoid patients)
and noises heard over the headphones could be ignored. After the
received typical neuroleptic medication (i.e., haloperidol or
presentation of a single noise burst to familiarize the person with
fluphenazine), and the remaining nine patients (two women, four
the startle-eliciting stimulus, each 25-min test session consisted
paranoid patients) were treated with atypical neuroleptics such as
of 75 trials. In 60 of those trials, the onset of the prepulse stimuli
clozapine or zotepine. The mean daily doses were 20.2 (range:
preceded the onset of the startle-eliciting stimulus by 30, 60, 120,
5– 45) mg for typical and 311.1 (range: 175– 400) mg for atypical
or 240 msec. There were 15 presentations of each of these four
lead intervals. Fifteen startle probes were presented without
Psychopathology was assessed for 12 medicated and five
prestimulation to determine the control level of responsivity. The
unmedicated schizophrenia patients at the time of testing, using
intertrial intervals varied between 7 and 21 sec. The different
the Positive and Negative Syndrome Scale (PANSS; Kay et al
lead intervals and the probe-alone trials were presented in a
1987). The unmedicated patients showed a significantly more
severe positive syndrome compared with the medicated patients[t(15)ϭ 3.28, p Ͻ .01; d ϭ 1.38; power ϭ .67] (Table 1) . Data Reduction and Response Definition
Neither the negative syndrome severity nor the scores on thegeneral psychopathology scale differed between the unmedicated
Startle-response magnitude and latency were scored offline using
and medicated schizophrenia patients.
the rectified and boxcar-filtered EMG (11-msec time window;
Fourteen age-matched healthy controls (six women) were
Cook and Miller 1992). Responses starting 20 –100 msec after
recruited from the hospital and laboratory staff. Mean ages in
probe onset and reaching peak amplitude within 150 msec were
years (Ϯ SE) were 32.6 (Ϯ 2.4), 34.6 (Ϯ 2.5), and 37.6 (Ϯ 5.1)
identified as startle eyeblinks. Response magnitude was scored as
for healthy controls, medicated, and unmedicated patients, re-
the difference between onset and peak amplitude in microvolts
spectively. Gender was counterbalanced across groups (2 Ͻ 1).
(V). Onset latency was scored in msec. No detectable eyeblinks
Psychopathology scores were only obtained for schizophrenia
were scored as zero responses. Electromyogram baseline activity
was measured for 20 msec after startle-probe onset. Trials with
clear movement artifacts or excessive baseline activity were
rejected. Missing values were replaced by the average of thevalues of that condition from the preceding and following trials.
As in our previous experiments, results of various distribution
Startle response magnitudes elicited during the control con-
analyses suggested that startle should be standardized. Therefore,
dition did not differ between groups (F Ͻ 1, Eta2 ϭ 0, power
blink amplitudes were standardized to z scores individually for
ϭ .07) (means were 11.8, 14.0, and 12.8 V for the
unmedicated schizophrenia patients, medicated schizophre-
Following the criteria defined by Graham and Murray (1977), the
subjects were excluded from further analyses if 1) rejected trials
nia patients, and controls, respectively). As expected, the
exceeded 33% of all trials, 2) rejected trials exceeded 50% of the
control subjects showed a significant reduction of their blink
trials in any condition, or 3) less than 50% nonzero responses were
magnitudes relative to the control condition when prepulse
elicited in the control trials. According to the third criterion, two
stimuli preceded the startle-eliciting probe [Fs(1,11) ϭ 10.36,
unmedicated schizophrenia patients and one control subject had to
32.51, 28.94, and 8.62, p Ͻ .01; Eta2 ϭ .49, .75, .73, and .44;
be excluded from subsequent analyses. One further control subject
power ϭ .83, Ͼ.99, Ͼ.99, and .76 for the 30-, 60-, 120-, and
was excluded due to more than 50% missing values. Thus, five
240-msec lead intervals, respectively]. As predicted, this PPI
unmedicated and 20 medicated schizophrenia patients and 12
was strongest for the 60- and the 120-msec lead intervals
control subjects were included in the statistical analyses. The ratio of
[quadratic component: F(1,11) ϭ 11.27, p Ͻ .01; Eta2 ϭ .51;
discarded trials was overall 5.4% (150 out of 2775 trials) and was
power ϭ .86]. Medicated schizophrenia patients showed the
larger for the unmedicated schizophrenia patients (16.3%) than formedicated patients (4.5%) and controls (2.4%). The higher rate of
same effects [Fs(1,19) ϭ 10.6, 38.22, 33.65, and 11.04, p Ͻ
rejected trials in the group of unmedicated patients was due to
01; Eta2 ϭ .36, .67, .64, and .37; power ϭ .87, Ͼ.99, Ͼ.99,
higher EMG baseline level in this group, which deteriorates the
and .98 for the four different lead conditions]. Again, PPI was
strongest for the 60- and 120-msec lead intervals [quadraticcomponent: F(1,19) ϭ 23.88, pϽ .001; Eta2 ϭ .56; power ϭ
Ͼ.99]. By contrast, prestimulation did not affect startlemagnitudes in the unmedicated schizophrenia patients for
To assess the overall responsivity across groups, blink magnitudes
either lead condition (all Fs Ͻ 1, Eta2 Ͻ .13, power Ͻ .12).
were first analyzed for the probe-alone trials using a univariate
Between-group comparisons supported the specific deficit in
analysis of variance (ANOVA) with group (unmedicated vs. med-icated schizophrenia patients vs. controls) as a between factor. To
prepulse inhibition in the unmedicated schizophrenia pa-
test the overall effects of prestimulation, average startle-response
tients. An ANOVA comparing the amount of PPI in the 60-
magnitudes in the control condition were compared with the average
and 120-msec lead conditions among all three groups re-
blink magnitudes in each of the four prestimulus conditions. To
vealed a significant overall group effect [F(2,34) ϭ 5.44, p Ͻ
compare the amount of inhibition across the four lead intervals,
.01; Eta2 ϭ .24; power ϭ .81]. Post hoc group comparisons
mean standardized difference scores were computed between the
showed that while the amount of PPI in the medicated
blink magnitudes in the probe-alone control condition and the
patients did not differ from that in the controls (F Ͻ 1, Eta2 ϭ
blink-response magnitudes in each lead interval condition. These
.02, power ϭ .16), unmedicated schizophrenia patients
difference scores were analyzed within each group using the four
showed a significant deficit in prepulse inhibition relative to
lead conditions (30- vs. 60- vs. 120- vs. 240-msec lead intervals) asa repeated measures factor. According to previous research, stron-
both controls [Group: F(1,15) ϭ 11.42, p Ͻ .01; Eta2 ϭ .43;
gest PPI was expected for the 60- and 120-msec lead intervals (Braff
power ϭ .88] and medicated patients [Group: F(1,23) ϭ
et al 1992; Graham 1975). Therefore, between-group comparisons
8.62, p Ͻ .01; Eta2 ϭ .75; power ϭ .80]. These group
of the amount of PPI were carried out for these two lead intervals.
differences were stable throughout the entire experiment. A 3
For all correlational analyses between the amount of PPI and the
(group) ϫ 5 (blocks of three trials) ANOVA of the mean
patients’ symptomatic status, the difference scores were averaged
amount of PPI (mean differences between response magni-
across the 60- and 120-msec lead condition.
tudes in the control condition and those in the 60- and
The unmedicated schizophrenia patients showed a higher EMG
120-msec lead interval conditions) did not reveal any signif-
baseline level (3.7 V) relative to the medicated patients (2.1 V)
icant Group ϫ Trialblock interaction (F Ͻ 1, Eta2 ϭ .04,
and controls (2.0 V). Furthermore, there was a small positive
power ϭ .33). Figure 1 illustrates the mean startle-response
correlation (r ϭ .20) between the baseline level and responsemagnitudes. Therefore, additional analyses of covariance (AN-
magnitudes for the different lead intervals and the control
COVA) with the baseline level as the covariate were computed in all
between-group analyses. Results of these ANCOVAs are onlyreported if they differed from the findings in the ANOVAs.
Onset latencies of the startle response were analyzed using the
same analysis plan as for the magnitude data. Unlike the startle
As for magnitudes, the latencies of blink onset did not
magnitudes, between-group comparisons were carried out for the
differ across groups in the control condition [F(2,34) ϭ
30-msec lead condition (see Graham and Murray 1977).
1.66, ns; Eta2 ϭ .09; power ϭ .32] (mean latencies were
Figure 1. Mean (Ϯ SE) blink magnitudes tostartle probes presented at 30, 60, 120, or 240msec after the onset of acoustic prepulses forunmedicated and medicated schizophrenia pa-tients and healthy control subjects. The 0-mseclead interval corresponds to the control condi-tion—i.e., startle probes were presented with-out prestimulation. Blink magnitudes are ex-pressed as stardardized differences from thecontrol condition with negative values reflect-ing blink inhibition.
50.0, 53.3, and 49.0 msec for the unmedicated and
also exhibited a clear deficit in PPI [Group1: F(1,13) ϭ
medicated schizophrenia patients and the control subjects,
6.35, p Ͻ .05; Eta2 ϭ .33; power ϭ .64]. To test whether
respectively). Relative to the control condition there was a
the lack of startle inhibition was related to the severity of
clear facilitation of blink-onset latency if a prepulse
the positive syndrome, ANCOVAs were computed. Using
preceded the startle-eliciting stimulus by 30 msec in
the severity of the positive syndrome as a covariate, the
controls [F(1,11) ϭ 14.18, p Ͻ .01; Eta2 ϭ .56; power ϭ
difference in prepulse inhibition between the medicated
.93] and medicated schizophrenia patients [F(1,19) ϭ
and unmedicated schizophrenia patients was no longer
47.81, p Ͻ .001; Eta2 ϭ .56; power ϭ .93]. This latency
significant. By contrast, if the severity of the negative
modulation of the startle by prestimulation was absent in
syndrome or the general psychopathology was used as a
the unmedicated patients (F Ͻ 1, Eta2 ϭ .02, power ϭ
covariate, the group differences remained significant in
.06). This pattern of results was again supported by the
this comparison [F(1,12) ϭ 6.91, p Ͻ .05; Eta2 ϭ .37;
overall between-group analysis of the blink latencies in the
power ϭ .67 for the negative syndrome scale as covariate]
30-msec lead interval condition [Group: F(2,34) ϭ 6.59, p
[F(1,12) ϭ 5.81, p Ͻ .05; Eta2 ϭ .33; power ϭ .60 for
Ͻ .01; Eta2 ϭ .28; power ϭ .88]. Post hoc analyses
general psychopathology as covariate]. The relationship
revealed that the unmedicated schizophrenia patients
between severity of the positive syndrome and the deficit
showed a lack of response facilitation at the 30-msec lead
in PPI corresponded to a significant Spearman correlation
interval relative to both the controls [F(1,15) ϭ 5.67, p Ͻ
coefficient of r ϭ .66 (p Ͻ .01). The patients whose
.05; Eta2 ϭ .27; power ϭ .60] and the medicated patients
positive symptoms were rated as more severe showed less
[F(1,23) ϭ 11.86, p Ͻ .01; Eta2 ϭ .34; power ϭ .91].
PPI2 in the 60- and 120-msec lead conditions (see Figure
Figure 2 illustrates the mean startle-onset latencies in msec
3). By contrast, no significant correlations were found
for the three groups and the different lead conditions.
between the amount of PPI and the severity of the negative
The type of neuroleptic medication did not affect the
syndrome (r ϭ .11, p ϭ .70) or the severity of general
modulation of the startle response magnitudes. The amount
psychopathology (r ϭ .49, p ϭ .06). Moreover, PPI was
of PPI did not differ for the patients receiving either typical oratypical neuroleptic medication. Accordingly, no such differ-
ences were observed for response latencies.
Twelve medicated and three unmedicated patients were included in this compar-
ison (the startle data of two unmedicated schizophrenia patients had to bediscarded due to nonresponsiveness).
2Prepulse inhibition is expressed as the mean standardized difference between the
Psychopathology and Startle Modulation
blink magnitudes in the control condition and those in the 60- and 120-mseclead intervals—i.e., less PPI corresponds to numerically higher values. The
The unmedicated schizophrenia patients showed a signif-
correlations between the amount of PPI and the psychopathology scores were
icantly severer positive syndrome compared with the
also significant, if the difference scores for each of the two lead intervals wereanalyzed (r ϭ .67, p Ͻ .01 for the 60-msec and r ϭ .62, p Ͻ .02 for the
medicated patients as assessed by the PANSS, and they
Figure 2. Mean (Ϯ SE) blink onset laten-cies to startle probes presented at 30, 60,120, or 240 msec after the onset of acousticprepulses for unmedicated and medicatedschizophrenia patients and healthy controlsubjects. The 0-msec lead interval corre-sponds to the control condition—i.e., star-tle probes were presented without pre-stimulation.
expressed as differences from the controlcondition in msec with negative valuesreflecting blink facilitation.
not significantly related to the dose ϫ duration interaction
could therefore be ignored. In these studies, differences
of neuroleptic medication as assessed by nonlinear regres-
between schizophrenia patients and healthy controls
sion analyses (R2 Ͻ 0 for typical and atypical medication,
were only obtained in the “active attention paradigm.”
In this paradigm, healthy controls exhibited a relativeenhancement of PPI when they were instructed to
Discussion
selectively attend to the prepulses, whereas schizophre-nia patients failed to show this attentional modulation of
Sensorimotor Gating and Schizophrenia
PPI (for review see Dawson et al 1997).
The unmedicated schizophrenia patients showed a clear
The findings in our experiment suggest that differ-
deficit in PPI relative to the control subjects, supported
ences in the type of paradigm might not be the main
by both between- and within-group comparisons. This
reason for the different findings of Braff et al and
reduced inhibition of the startle response after weak
Dawson and coworkers. Using the same experimental
prestimulation was not due to general deficits in startle
procedure in our study, the unmedicated schizophrenia
reactivity in these patients, since the normal controls
patients showed substantial impairment of PPI, while
and schizophrenia patients did not differ in startle-
the medicated patients did not differ from the controls.
response magnitudes to the probe-alone presentations.
These findings suggest that medication status might be
These data support the findings of Braff and collabora-
important in modulating the amount of PPI in schizo-
tors (Braff et al 1978, 1992; Grillon et al 1992)
phrenia patients when no explicit instructions are given
indicating that schizophrenia patients might have defi-
to either attend to or ignore the prepulse stimuli. On the
cits in automatic sensorimotor gating. On the other
other hand, Hazlett et al (1998) found no differences
hand, for the medicated schizophrenia patients, the
between unmedicated schizophrenia patients and nor-
blink magnitudes were substantially reduced if a tone
mal controls in a passive attention condition. However,
preceded the startle-eliciting stimulus at lead intervals
81% of the unmedicated patients had received neuro-
of 60 and 120 msec. The amount of PPI for these
leptic medication before with a substantial variation of
patients was identical to that obtained in the control
the periods of washout. Moreover, there were also
group. The findings in this patient group thus confirm
strong differences in the total psychopathology scores
the results from Dawson and collaborators (Dawson et
within the sample of schizophrenia patients in that
al 1993; Hazlett et al 1998) indicating that schizophre-
study. Thus, besides the medication status, specific
nia patients do show the same amount of PPI compared
patient characteristics might also be important in mod-
with controls in the so-called “passive attention para-
ulating the amount of PPI. The data from our study
digm”—i.e., when subjects were instructed that the
suggest that patients’ symptomatic status might be an
tones that served as prestimuli were task irrelevant and
Figure 3. Correlation between the amount of prepulseinhibition and the positive syndrome severity. Eachdata point represents one schizophrenia patient. Theamount of prepulse inhibition is expressed as the meanstandardized difference score of the blink magnitudesat the 60- and 120-msec lead intervals. Positive syn-drome severity relates to the individual score in thecorresponding subscale (range: 7– 49) of the Positiveand Negative Syndrome Scale (PANSS) for schizo-phrenia (Kay et al 1987). The dashed line reflects thelinear regression. Prepulse Inhibition and Psychopathology
induced deficits in PPI (Mansbach and Geyer 1989;
The differences in PPI between the medicated and un-
Mansbach et al 1988). While pretreatment with typical
medicated schizophrenia patients were no longer signifi-
neuroleptics restores amphetamine-induced PPI deficits,
cant if the severity of positive symptoms was used as a
these drugs are ineffective in restoring PCP-induced PPI
covariate in the statistical analyses—i.e., the correlation
deficits. Phencyclidine-induced deficits in PPI can, how-
between the amount of PPI and the rated severity of the
ever, be antagonized by the atypical antipsychotic cloza-
patients’ positive symptoms was significant. By contrast,
pine, which has blocking properties to multiple receptors
the general psychopathology scores and the negative
in various neurotransmitter systems (Bakshi et al 1994).
syndrome showed only a moderate relationship to the
These findings suggest that there is not a general effect of
amount of PPI in the entire group of schizophrenia
neuroleptic medication on PPI; rather, neuroleptic medi-
patients, which, however, was not significant. This was
cation is only effective if it acts on the system where the
also supported in a recent study by Volz et al (M. Volz et
al, unpublished data, 1999), who found no deficits in PPI
In our study the medicated schizophrenia patients
in a sample of 49 schizophrenia outpatients who exhibited
showed overall less positive symptoms compared with the
pronounced negative symptoms but showed virtually no
unmedicated patients. However, the severity of the posi-
florid psychopathology at the time of testing. Moreover, in
tive syndrome varied substantially within the group of
our study three patients who despite being medicated
medicated patients, indicating that some patients did not
exhibited the same amount of positive symptoms as
show an adequate clinical response to their medication.
unmedicated schizophrenia patients also showed the same
These patients also exhibited clear deficits in PPI. Al-
deficits in PPI as the unmedicated patients. This finding
though there were substantial differences in the duration of
suggests that in cases wherein the neuroleptic treatment is
treatment within the group of medicated patients, treat-
not effective in reducing the positive symptoms, schizo-
ment duration cannot completely explain the differences in
phrenia patients show an impairment of PPI.
the clinical response. For the three medicated patients
The data from our experiment suggest that PPI might be
showing enhanced psychopathology scores and clear PPI
a useful prescreening method for testing the clinical
deficits, the treatment durations were 2, 7, and 25 weeks.
potential of neuroleptics. Medication that effectively re-
These findings question the hypothesis that simple block-
duced positive symptoms also removed PPI deficits,
ade of the receptors is sufficient to reduce PPI deficits in
whereas drugs that were clinically less effective also failed
these patients. Future research should test more explicitly
to restore PPI. These data are in line with animal models
the time course of recovery of PPI with regard to treatment
of PPI deficits. In rats, a systemic administration of the
duration, the effects of different neuroleptics, and their
indirect dopamine agonist amphetamine as well as the
doses and interactions with the clinical drug response—
noncompetitive NMDA antagonist phencyclidine (PCP)
i.e., changes in psychopathology. Moreover, future studies
should also include more chronically ill schizophrenia
need to be replicated in a within-subjects design in future
patients to explore PPI in patients who are less responsive
research. Preliminary data of a single case yielded prom-
ising results. One unmedicated schizophrenia patient who
Supporting the findings from Dawson and his collabo-
showed no PPI (⌬z ϭ .15) in a first test session also
rators, symptomatic medicated schizophrenia patients did
exhibited severe positive symptoms (the positive syn-
not differ in their PPI relative to the controls in our
drome score was 19). When tested again 38 days later after
study—i.e., when participants were not instructed to se-
being treated with fluphenazine, the patient’s positive
lectively attend to or ignore the prepulse stimuli. These
symptom score was reduced to 14 and the same patient
results are also concordant with recent findings from
showed PPI (⌬z ϭ Ϫ.30) at the second test session.
Hazlett et al (1998), suggesting that deficits in automatic
Our data support the notion that deficits in sensorimotor
sensorimotor gating might not be a general trait-linked,
gating might be related to sensory overload, cognitive
stable vulnerability indicator for schizophrenia. The mixed
fragmentation, and thought disorder—i.e., characteristic
results regarding PPI deficits in psychosis-prone college
symptoms of an active episode of the disorder. However,
students support this notion (Cadenhead et al 1996). On
in the current sample of medicated and unmedicated
the other hand, one has to acknowledge that the lack of a
schizophrenia patients, the severity of positive symptoms
strong correlation between PPI deficits and schizotypy or
accounted for only about 39% of the variance of PPI,
psychosis proneness scales does not mean that PPI impair-
suggesting that factors other than psychopathology are
ment is not a trait marker, since PPI deficits might be
influencing the amount of PPI as well. It has been
associated with one gene and schizotypy or psychosis
demonstrated that gender accounts for differences in the
proneness might reflect another inherited trait, but both
amount of PPI. In three studies, Swerdlow and colleagues
markers might be related to schizophrenia. However,
found that men exhibited stronger PPI than women (Swerd-
before drawing any definite conclusions it would be
low et al 1993a, 1995a, 1997), a finding that was repli-
desirable to test PPI in a clinical group of schizophrenia
cated in the present study, but only for the healthy
patients and also to assess PPI in their first-degree rela-
controls. No gender effects occurred in the schizophrenia
tives. Moreover, it would also be interesting to relate PPI
patients. This finding must be interpreted cautiously be-cause we investigated only a small sample of female
to other psychophysiological variables that have been used
subjects and we did not assess the menstrual cycle for
to identify vulnerability markers for schizophrenia— e.g.,
these participants. It has been shown that PPI covaries
the eye-tracking performance (Iacono 1998). Although no
with the menstrual cycle (Swerdlow et al 1997).
relations were found between PPI and the suppression of
Reduced PPI has also been reported in other clinical
the P50 component of the evoked potential in a double-
populations as well, including patients with Huntington’s
click paradigm (Schwarzkopf et al 1993), the performance
disease (Swerdlow et al 1995b), obsessive– compulsive
in negative priming or the Stroop test (Swerdlow et al
disorder (Swerdlow et al 1993b), Tourette’s syndrome
1995a) in normal volunteers, a covariation between PPI
with attention-deficit/hyperactivity disorder (Castellanos
and behavioral measures of distractibility was observed in
et al 1996), and nocturnal enuresis (Ornitz et al 1992). As
a sample of chronic schizophrenia patients (Karper et al
revealed by animal research, a complex corticolimbic
striatopallidal circuitry modulates the primary PPI path-way via a projection to the pedunculopontine tegmental
nucleus, suggesting that a variety of neurophysiological
One caveat is that the effect of medication and psychopa-
dysregulations may result in deficits in PPI (Koch and
thology was tested in a relatively small sample of schizo-
Schnitzler 1997; Swerdlow et al 1992).
phrenia patients in a between-subject design. Therefore, it
In our study, clear deficits in PPI were obtained for
is difficult to determine whether medication effects or
patient characteristics were responsible for the PPI deficits
amount of PPI covaried with the severity of positive
or the lack thereof. This point is all the more important
symptoms. Those patients who did not respond very well
considering that PPI was tested in a quasi-experimental ex
to the antipsychotic medication also showed a clear deficit
post facto design, and patients were not assigned randomly
in PPI, suggesting that PPI might be used as a method to
to the different conditions due to clinical reasons. On the
assess the clinical potential of neuroleptic medication.
other hand, PPI deficits correlated significantly with theseverity of the patients’ positive symptoms, but not withthe negative syndrome and only moderately with the
This research was supported by grants from the Deutsche Forschungs-
general psychopathology. The present covariations be-
gemeinschaft (German Research Society) to Alfons Hamm (Ha 1593/6-2;Ha 1593/10-2).
tween medication, psychopathology, and PPI, however,
References
significance of human startle eyeblink modification: A re-view. Biol Psychol 47:1– 43.
American Psychiatric Association (1987): Diagnostic and Sta-
Freedman R, Adler EA, Gerhardt GA, Waldo M, Baker N, Rose
tistical Manual of Mental Disorders, 3rd ed rev. Washington,
GM, et al (1987): Neurobiological studies of sensory gating in
DC: American Psychiatric Assocation Press.
schizophrenia. Schizophr Bull 13:669 – 678.
Anthony BJ (1985): In the blink of an eye: Implications of reflex
Geyer MA, Braff DL (1987): Startle habituation and sensorimo-
modification for information processing. In: Ackles PK,
tor gating in schizophrenia and related animal models. Schizo-
Jennings JR, Coles MGH, editors. Advances in Psychophys-iology, Vol 1. Greenwich, CT: JAI Press, 167–218.
Geyer MA, Swerdlow NR, Mansbach RS, Braff DL (1990):
Bakshi VP, Swerdlow NR, Geyer MA (1994): Clozapine antag-
Startle response models of sensorimotor gating and habitua-
onizes phencyclidine-induced deficits in sensorimotor gating
tion deficits in schizophrenia. Brain Res Bull 25:485– 498.
of the startle response. J Pharmacol Exp Ther 271:787–794.
Graham FK (1975): The more or less startling effects of weak
Blumenthal T, Creps CL (1994): Normal startle responding in
prestimulation. Psychophysiology 12:238 –248.
psychosis-prone college students. Pers Individual Differences17:345–355.
Graham FK (1992): Attention: The heartbeat, the blink, and the
brain. In: Campbell BA, Hayne H, Richardson R, editors.
Braff D, Stone C, Callaway E, Geyer M, Glick I, Bali L (1978):
Attention and Information Processing in Infants and Adults:
Prestimulus effects on human startle reflex in normals and
Perspectives from Human and Animal Research. Hillsdale,
schizophrenics. Psychophysiology 15:339 –343.
Braff DL (1985): Attention, habituation, and information pro-
Graham FK, Murray GM (1977): Discordant effects of weak
cessing in psychiatric disorders. In: Michels R, Cavenar JO,
prestimulation on magnitude and latency of the reflex blink.
Brodie HK, Cooper AM, Guze SB, Judd LL, et al, editors. Physiol Psychol 5:108 –114. Psychiatry, Vol 3. Philadelphia: Lippincott, 1–13.
Grillon C, Ameli R, Charney DS, Krystal J, Braff D (1992):
Braff DL (1993): Information processing and attention dysfunc-
Startle gating deficits occur across prepulse intensities in
tions in schizophrenia. Schizophr Bull 19:233–259.
schizophrenic patients. Biol Psychiatry 32:939 –943.
Braff DL, Grillon C, Geyer MA (1992): Gating and habituation
Hazlett EA, Buchsbaum MS, Haznedar MM, Singer MB, Ger-
of the startle reflex in schizophrenic patients. Arch Gen
mans MK, Schnur DB, et al (1998): Prefrontal cortex glucose
metabolism and startle eyeblink modification abnormalities in
Braff DL, Saccuzzo DP, Geyer MA (1991): Information process-
unmedicated schizophrenia patients. Psychophysiology 35:
ing dysfunctions in schizophrenia: Studies of visual backward
masking, sensorimotor gating, and habituation. In: Steinhauer
Hoffman HS (1997): Attentional factors in the elicitation and
SR, Gruzelier JH, Zubin J, editors. Handbook of Schizophre-
modification of the startle reaction. In: Lang PJ, Simons RF,
nia, Vol 5. Amsterdam: Elsevier, 303–334.
Balaban MT, editors. Attention and Orienting: Sensory and
Cadenhead K, Kumar C, Braff D (1996): Clinical and experi-
Motivational Processes. Hillsdale, NJ: Erlbaum, 185–204.
mental characteristics of “hypothetically psychosis prone”
Hoffman HS, Ison JR (1980): Reflex modification in the domain
college students. J Psychiatr Res 30:331–340.
of startle: I. Some empirical findings and their implications
Cadenhead KS, Geyer MA, Braff DL (1993): Impaired startle
for how the nervous system processes sensory input. Psychol
prepulse inhibition and habituation in patients with schizo-
typal personality disorder. Am J Psychiatry 150:1862–1867.
Hoffman HS, Ison JR (1992): Reflex modification and the
Castellanos FX, Fine EJ, Kaysen D, Marsh WL, Rapoport JL,
analysis of sensory processing in developmental and compar-
Hallett M (1996): Sensorimotor gating in boys with
ative research. In: Campbell BA, Hayne H, Richardson R,
Tourette’s syndrome and ADHD: Preliminary results. Biol
editors. Attention and Information Processing in Infants andAdults: Perspectives from Human and Animal Research.
Cook EW, Miller GA (1992): Digital filtering: Background and
tutorial for psychophysiologists. Psychophysiology 29:350 –
Iacono WG (1998): Identifying psychophysiological risk for
psychopathology: Examples from substance abuse and
Davis M (1997): The neurophysiological basis of acoustic startle
schizophrenia research. Psychophysiology 35:621– 637.
modulation: Research on fear motivation and sensory gating.
Karper LP, Freeman GK, Grillon C, Morgan CA III, Charney
In: Lang PJ, Simons RF, Balaban MT, editors. Attention and
DS, Krystal JH (1996): Preliminary evidence of an associa-
Orienting: Sensory and Motivational Processes. Hillsdale,
tion between sensorimotor gating and distractability in psy-
chosis. J Neuropsychiatry Clin Neurosci 8:60 – 66.
Dawson ME, Hazlett EA, Filion DL, Nuechterlein KH, Schell
Kay SR, Fiszbein A, Opler LA (1987): The positive and negative
AM (1993): Attention and schizophrenia: Impaired modula-
syndrome scale (PANSS) for schizophrenia. Schizophr Bull
tion of the startle reflex. J Abnorm Psychol 102:633– 641.
Dawson ME, Schell AM, Swerdlow NR, Filion DL (1997):
Koch M, Bubser M (1994): Deficient, sensorimotor gating after
Cognitive, clinical, and neurophysiological implications of
6-hydroxydopamine lesion of the rat medial prefrontal cortex
startle modification. In: Lang PJ, Simons RF, Balaban MT,
is reversed by haloperidol. Eur J Neurosci 6:1837–1845.
editors. Attention and Orienting: Sensory and Motivational
Koch M, Schnitzler HU (1997): The acoustic startle response in
Processes. Hillsdale, NJ: Erlbaum, 257–279.
rats: Circuits mediating evocation, inhibition, and potentia-
Filion DL, Dawson ME, Schell AM (1998): The psychological
tion. Behav Brain Res 89:35– 49.
Lipp OV, Siddle DAT, Arnold SL (1994): Psychosis proneness
Simons RF, Giardina BD (1992): Reflex modification in psycho-
in a non-clinical sample II: A multi-experimental study of
sis-prone young adults. Psychophysiology 29:8 –16.
“attentional malfunctioning.” Pers Individual Differences 17:
Swerdlow NR, Auerbach P, Monroe SM, Hartston H, Geyer MA,
Braff DL (1993a): Men are more inhibited than women by
Mansbach RS, Geyer MA (1989): Effects of phencyclidine and
weak prepulses. Biol Psychiatry 34:253–260.
phencyclidine biologs on sensorimotor gating in the rat.
Swerdlow NR, Benbow CH, Zisook S, Geyer MA, Braff DL
Neuropsychopharmacology 2:299 –308.
(1993b): A preliminary assessment of sensorimotor gating in
Mansbach RS, Geyer MA, Braff DL (1988): Dopaminergic
patients with obsessive compulsive disorder. Biol Psychiatry
stimulation disrupts sensorimotor gating in the rat. Psycho-
Swerdlow NR, Caine SB, Braff DL, Geyer MA (1992): The
Nuechterlein KH, Dawson ME (1984): Information processing
neural substrates of sensorimotor gating of the startle reflex:
and attentional functioning in the developmental course of
A review of recent findings and their implications. J Psycho-
schizophrenic disorders. Schizophr Bull 10:160 –203.
Ornitz EM, Hanna GL, de Traversay J (1992): Prestimulation-
Swerdlow NR, Filion D, Geyer MA, Braff DL (1995a): “Nor-
induced startle modulation in attention-deficit hyperactivity dis-
mal” personality correlates of sensorimotor, cognitive, and
order and nocturnal enuresis. Psychophysiology 29:437– 451.
visuospatial gating. Biol Psychiatry 37:286 –299.
Rund B (1993): Backward-masking performance in chronic and
nonchronic schizophrenics, affectively disturbed patients, and
Swerdlow NR, Hartman PL, Auerbach PP (1997): Changes in
normal control subjects. J Abnorm Psychol 102:74 – 81.
sensorimotor gating across the menstrual cycle: Implicationsfor neuropsychiatric disorders. Biol Psychiatry 41:452– 460.
Schwarzkopf SB, Lamberti JS, Smith DA (1993): Concurrent
assessment of acoustic startle and auditory P50 evoked
Swerdlow NR, Paulsen J, Braff DL, Butters N, Geyer MA,
potential measures of sensory inhibition. Biol Psychiatry
Swenson MR (1995b): Impaired prepulse inhibition of acous-
tic and tactile startle response in patients with Huntington’sdisease. J Neurol Neurosurg Psychiatry 58:192–200.
Silverstein LD, Graham FK, Calloway JM (1980): Precondition-
ing and excitability of the human orbucularis oculi reflex as a
World Health Organization (1992): Manual of the International
function of state. Electroencephalogr Clin Neurophysiol 48:
Statistical Classification of Diseases, Injuries, and Causes ofDeath, 10th ed. Geneva: World Health Organization.
Disposable Plungers MADE IN GERMANY For pressing dental ceramics and Lithium Disilicate Ideal for pressing all ceramic ingots, includingLithium Disilicate. No need for cleaning or preheating. Discardafter use. No need for a separator when pressingLithium Disilicate. Consistent results when pressing LithiumDisilicate■ prevents transfer of heat from the plunger to the ceramic
DC Términos y condiciones de venta para operaciones realizas en MX VA-82560-12 Términos y Condiciones de Venta DCMX Tabla de contenido Objetivo Definir los términos y condiciones de venta para DCMX Alcance DCMX Terminología y abreviaciones DCMX: Bosch Rexroth S.A: de C.V. Responsabilidades Descripción Términos y Condiciones de Venta para operaciones
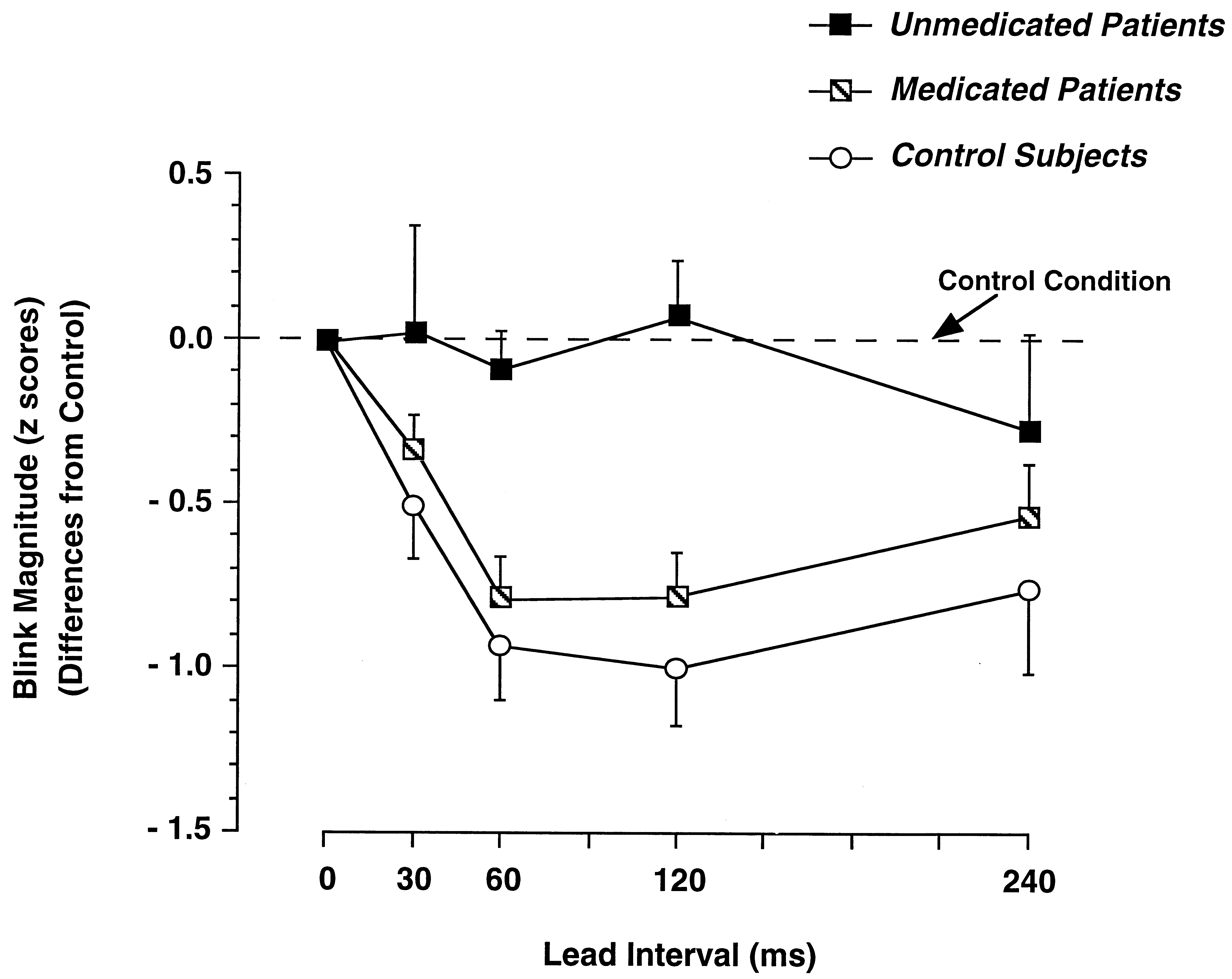 Figure 1. Mean (Ϯ SE) blink magnitudes tostartle probes presented at 30, 60, 120, or 240msec after the onset of acoustic prepulses forunmedicated and medicated schizophrenia pa-tients and healthy control subjects. The 0-mseclead interval corresponds to the control condi-tion—i.e., startle probes were presented with-out prestimulation. Blink magnitudes are ex-pressed as stardardized differences from thecontrol condition with negative values reflect-ing blink inhibition.
Figure 1. Mean (Ϯ SE) blink magnitudes tostartle probes presented at 30, 60, 120, or 240msec after the onset of acoustic prepulses forunmedicated and medicated schizophrenia pa-tients and healthy control subjects. The 0-mseclead interval corresponds to the control condi-tion—i.e., startle probes were presented with-out prestimulation. Blink magnitudes are ex-pressed as stardardized differences from thecontrol condition with negative values reflect-ing blink inhibition.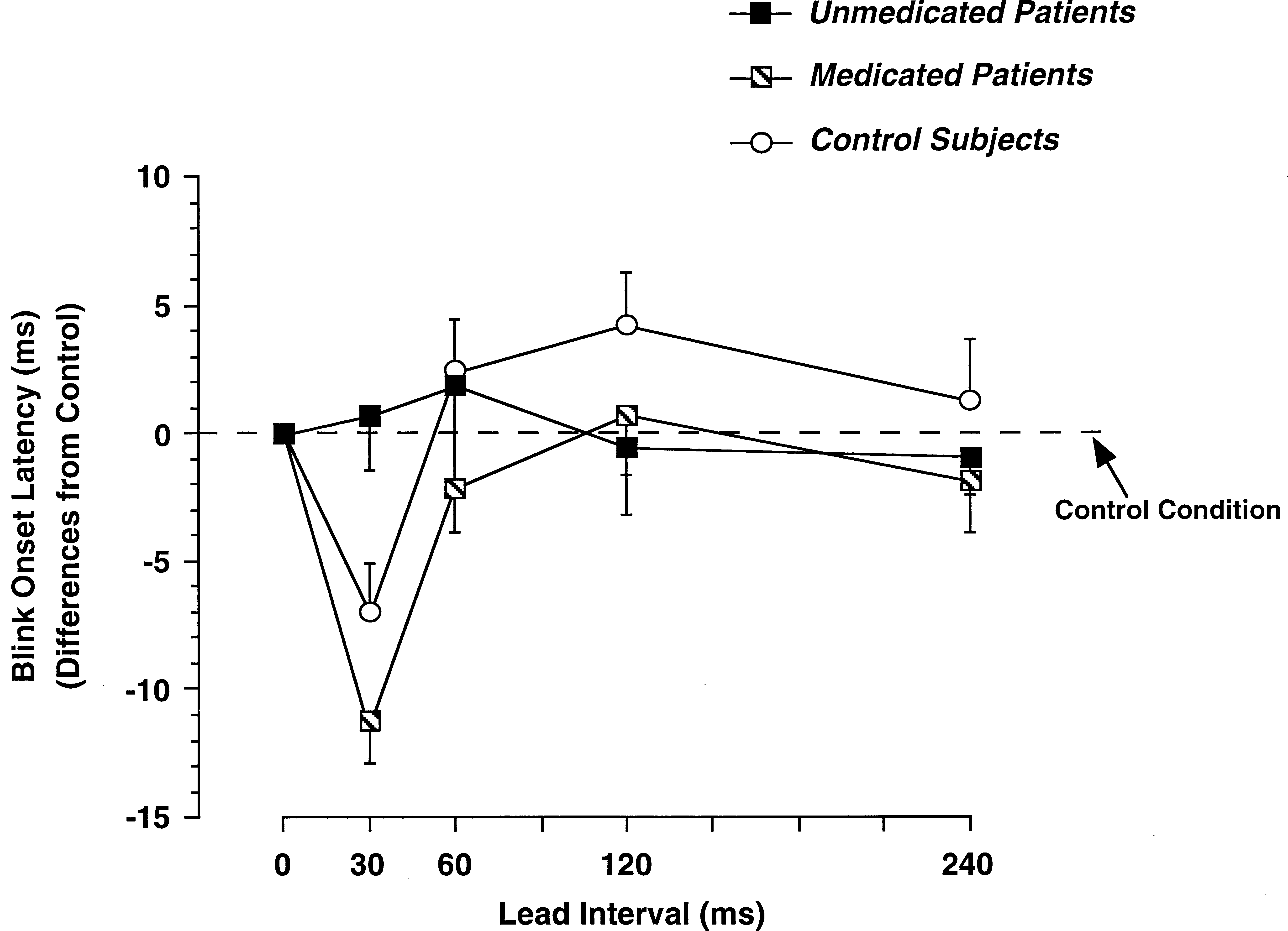 Figure 2. Mean (Ϯ SE) blink onset laten-cies to startle probes presented at 30, 60,120, or 240 msec after the onset of acousticprepulses for unmedicated and medicatedschizophrenia patients and healthy controlsubjects. The 0-msec lead interval corre-sponds to the control condition—i.e., star-tle probes were presented without pre-stimulation.
Figure 2. Mean (Ϯ SE) blink onset laten-cies to startle probes presented at 30, 60,120, or 240 msec after the onset of acousticprepulses for unmedicated and medicatedschizophrenia patients and healthy controlsubjects. The 0-msec lead interval corre-sponds to the control condition—i.e., star-tle probes were presented without pre-stimulation.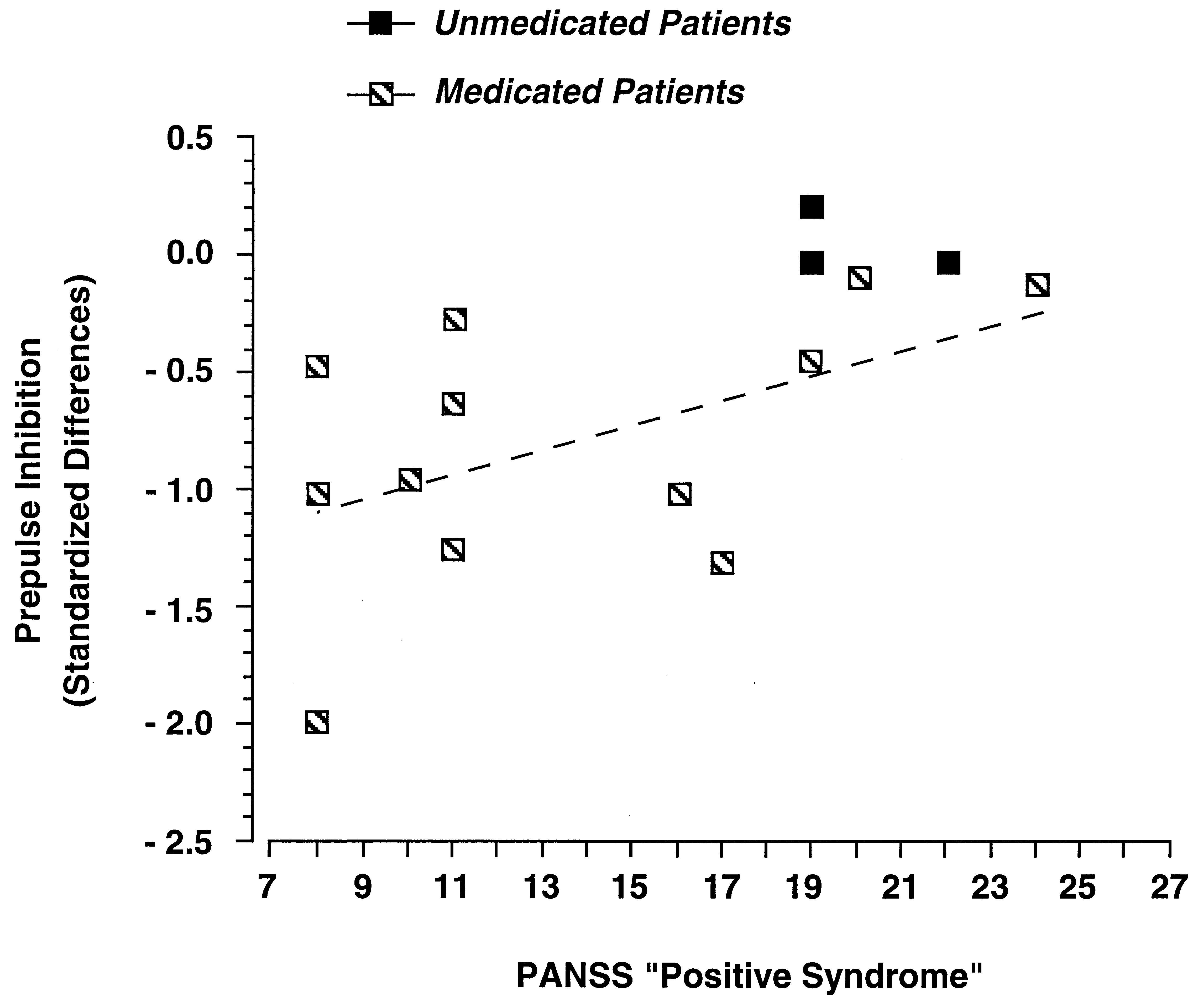 Figure 3. Correlation between the amount of prepulseinhibition and the positive syndrome severity. Eachdata point represents one schizophrenia patient. Theamount of prepulse inhibition is expressed as the meanstandardized difference score of the blink magnitudesat the 60- and 120-msec lead intervals. Positive syn-drome severity relates to the individual score in thecorresponding subscale (range: 7– 49) of the Positiveand Negative Syndrome Scale (PANSS) for schizo-phrenia (Kay et al 1987). The dashed line reflects thelinear regression.
Figure 3. Correlation between the amount of prepulseinhibition and the positive syndrome severity. Eachdata point represents one schizophrenia patient. Theamount of prepulse inhibition is expressed as the meanstandardized difference score of the blink magnitudesat the 60- and 120-msec lead intervals. Positive syn-drome severity relates to the individual score in thecorresponding subscale (range: 7– 49) of the Positiveand Negative Syndrome Scale (PANSS) for schizo-phrenia (Kay et al 1987). The dashed line reflects thelinear regression.