Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Cmn057 438.444
Ó The Author 2008. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: [email protected]. doi:10.1093/fampra/cmn057
Family Practice Advance Access published on 3 October 2008
Patients’ view on screening for depression in generalpractice
K A Wittkampfa,b, M van Zwietenb, F Th Smitsb, A H Schenea, JHuysera and H C van Weertb
Wittkampf KA, van Zwieten M, Smits FTh, Schene AH, Huyser J, van Weert HC. Patients’ view onscreening for depression in general practice. Family Practice 2008; 25: 438–444.
Background. In general practice, depression is often not recognized. As treatment of depres-sion is effective, screening has been proposed as one solution to combat this ‘hidden morbidity’. The results of screening programmes for depression, however, are inconsistent and most stud-ies do not show a positive effect on patient outcomes. Patients do not always accept this diag-nosis and hence do not receive proper treatment. Nothing is known about the tendency ofthose patients who screen positive for depression to accept treatment for their ‘disclosed’ disor-der.
Objective. In this study, we aimed to better understand the views of patients who screened pos-itive in a screening programme for depression.
Methods. We performed a qualitative study with semi-structured in-depth interviews with 17patients. These adult patients (nine females), all suffering from major depressive disorder, weredisclosed by a screening programme for depression performed within 11 Dutch general practi-ces. The transcripts were independently analysed by two researchers using MAXqda2.
Results. All patients appreciated the active way in which they were approached for screening. Fifteen of the 17 patients recognized the depressive symptoms but nine of them did not acceptthe diagnosis. The first explanation for resistance to the diagnosis of depression is fear of stig-matization and scepticism about the usefulness of labelling. Secondly, patients experiencedtheir depressive symptoms as a normal and transitory reaction to adversity. Thirdly, patientshad doubts about the necessity and effectiveness of treatment. Depressive symptoms, such asfeelings of guilt, self-depreciation and fatigue, hamper help-seeking behaviour.
Conclusions. We conclude that some patients with undisclosed depression, who took the trou-ble of going through a complete screening programme, felt aversion to being diagnosed ashaving depression. In the context of screening for depression, we recommend that the patients’view on depression be elicited before diagnosing and offering treatment.
Keywords. Depressive disorder, primary health care, qualitative methods, screening pro-grammes.
participation is a cornerstone of successful screeningand as such one of the indispensable conditions
In primary care, depression often goes undiagnosed.1
described by the UK National screening committee.7
Some clinicians plead for screening to disclose this
A complete screening programme (test, diagnostic pro-
hidden morbidity.2 Conversely, others report that
cedures and treatment/intervention) has to be clini-
screening and disclosure of unrecognized depression
cally, socially and ethically acceptable to health
does not have a positive effect on patients’ out-
professionals as well as to the public. Gilbody4 has
come.1,3–6 So far, the patients’ view on screening for
reported that the acceptance of screening tests for
depression has been missing in this discussion. Patient
depression is generally low: 30–60% of patients in
Received 13 March 2008; Revised 21 August 2008; Accepted 26 August 2008.
aDepartment of Psychiatry, Programme for Mood Disorders and bDepartment of General Practice, Academic Medical Center,University of Amsterdam and Jellinenk Mentrum Mental Health Care, Amsterdam, The Netherlands. Correspondence toK A Wittkampf, Department of Psychiatry, Academic Medical Center, Meibergdreef 5, 1105 AZ Amsterdam, The Netherlands;Email: [email protected]
Patients’ view on screening for depression
primary care decline to participate in screening ques-
patients who fulfilled to the DSM-IV criteria for major
depressive disorder. The first 17 patients with undis-
Studies have shown that patients experience difficul-
closed depression were included in this study. We con-
ties with being diagnosed as having depression.8 A
tinued including patients until the data were saturated.
remarkable difference exists between the conventional
In accordance with the Medical Research Involving Hu-
medical view and the patients’ view of the concept of
man Subjects Act (WMO) and with a local Medical
depression.9 This probably has to do with patients’
Ethics Committee, formal approval for this research pro-
views that depression is not the right label for their
ject by the Medical Ethics Committee was not necessary.
problems, a negative view of depression related to fearof stigmatization,8 doubts about the purpose of label-
ling, feelings of shame and scepticism about the bene-
The semi-structured in-depth interviews (n = 17) were
fits of therapy, in particular drug treatment.9–12
performed by one researcher (KAW) at the patients’
Additionally, patients may have difficulties in differen-
homes and each interview took about 40 minutes. The
tiating depression from understandable reactions to
aim of the interview was to provide an in-depth view-
adversity.9 Nothing is known about the tendency of
point based on personal experience, centred around
those patients who screen positive for depression to
the topic of the recent diagnosis of depressive disor-
seek treatment for their ‘disclosed’ disorder. A nega-
der. In the first six interviews, the following topics
tive view on being diagnosed with depression will
were explored; emotions and cognitions related to this
probably reduce the chance of acceptance of the diag-
diagnosis, previous experience of depression, conse-
quences of the diagnosis, acceptance of the diagnosis,
In this study, we aimed to better understand the
need for help, willingness to follow treatment and, if
views of patients in a screening programme for depres-
applicable, experience with different types of treat-
sion. We focused on primary care patients who were
willing to participate in such a programme, subse-
Initially collecting data was alternated with analy-
quently screened positive for depression, but who had
sing the transcripts i.e. sequential analysis or interim
not yet been diagnosed by their GP. In order to learn
analysis.16 The transcripts of the first six interviews
more about the views of these patients on screening
were read with a view to extracting topics that could
as well as on the diagnosis of depression, we per-
be missing from our primary topic list. Based on this
initial analysis, we added the topic ‘feelings about thescreening programme up to now’ because most of thepatients referred somehow to this topic. This adjusted
topic list was then used in successive interviews.
The questions were open-ended and the answers
were further explored by the interviewer. With the
This qualitative study was part of a larger project on
patients’ consent, interviews were recorded on audio
disease management for depression in which the first
tape and were fully transcribed. Patients were assured
step was to screen patients in 11 general practices.
that all views expressed would remain anonymous and
The population was ethnically mixed and consisted of
that their participation would be kept confidential.
three groups of adult primary care patients at risk for
Patients were also told that the outcome of the inter-
depression. The first group of patients were frequent
views would not have any effect on the post-screening
attenders; they had the 10% highest consultation rates
over the previous year adjusted for age and sex. Thesecond group of patients had presented with psychoso-cial problems and the third group had unexplained so-
matic symptoms, both during the previous 3 months.
The transcripts were analysed by two researchers
All patients known to be suffering from a depressive
(KAW and MvZ) using MAXqda2.17 The analysis
disorder, a psychotic disorder, a bipolar disorder,
consisted of multiple phases largely based on Pope’s
a cognitive disorder or who had major problems with
recommendations.16 First, to discover what the pa-
the Dutch or English language were excluded.
tients had said about these topics, one researcher
Selected patients received a self-report screening in-
(KAW) worked through the interviews deductively
strument by mail, the Patient Health Questionnaire
using the primary topic list: this is also known as the
(PHQ).13 Patients with a positive score on the PHQ
familiarization phase. Later on, the analyses continued
module for depression were subsequently interviewed
in a more inductive way to include other aspects like
by telephone using the Structured Clinical Interview
the definition of depression and perceptions of and
for DSM-IV Disorders (SCID)14 and the Hamilton
experiences with depression, as these subjects were
Depression Rating Scale (HDRS).15 Following the in-
frequently brought up by the patients. In this phase,
terview, the diagnosis of depression was notified to the
Family Practice—an international journal
Secondly, recurrent themes within the transcripts
phobia, social phobia and alcohol dependence. Six of
were selected and text fragments were sorted accord-
the 17 patients had been treated for depression in the
ing to the thematic framework. This consisted of the
following themes: (i) patients’ definition of depression;(ii) acceptance of the diagnosis of depression; (iii)
Patients’ views on screening for depression
patients’ view of causes of the depressive disorder;
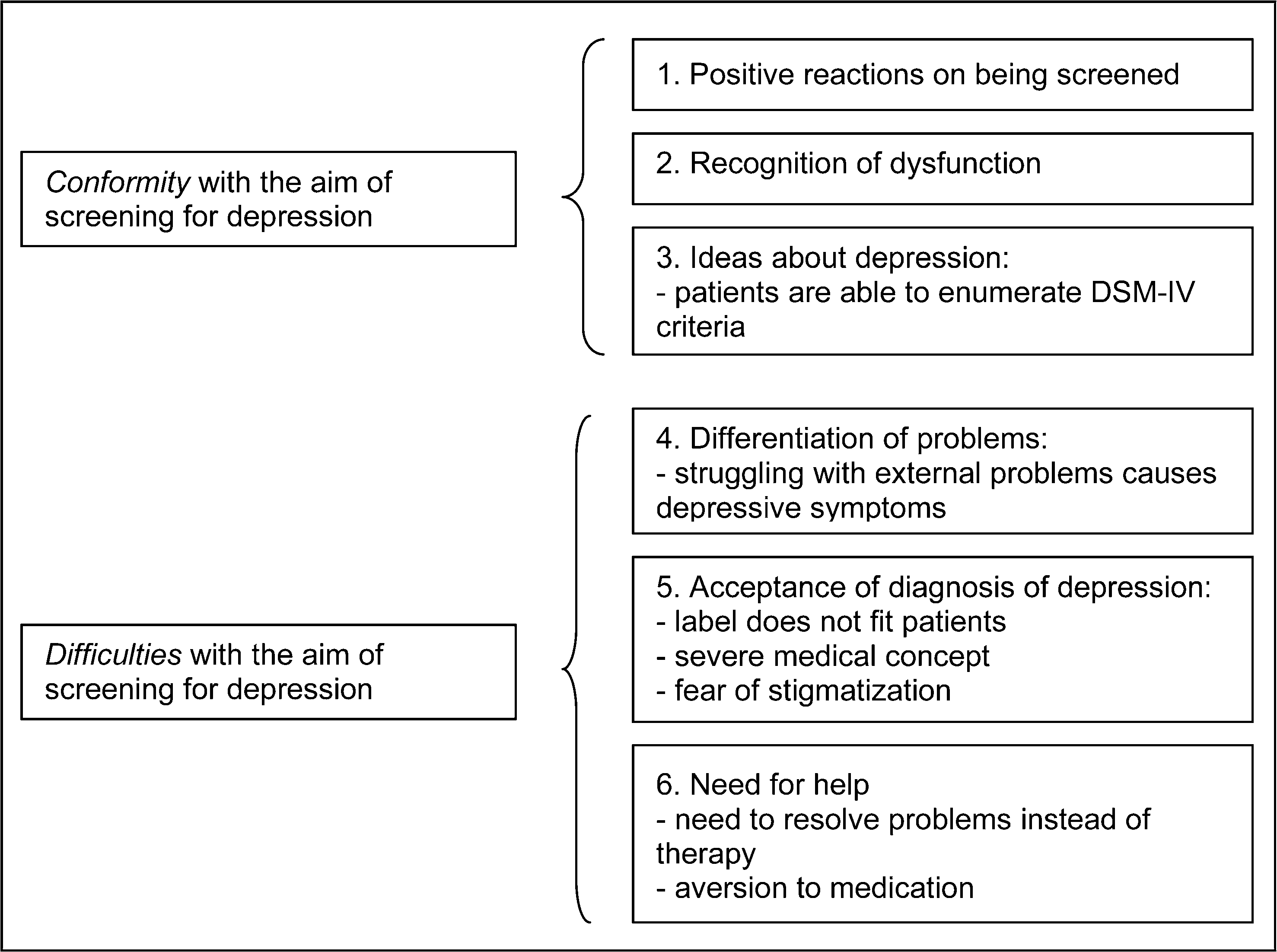
We identified six consecutive themes related to the
and (iv) physical symptoms and physical co-morbidity
main subject of our study: patients’ views on screening
related to the patients’ complaints. Next, the second
for depression. These six themes were (i) reaction to
author (MvZ) independently analysed all the inter-
being screened; (ii) recognition of dysfunction; (iii)
views and added the theme ‘reaction to being
ideas about depression; (iv) differentiation of prob-
screened’. Consensus meetings between all authors
lems; (v) acceptance of the diagnosis of depression;
led to the rearrangement of themes which is presented
and (vi) consequences of the diagnosis of depression
patients were positive about the process of beingscreened for depression. They appreciated the active
approach of their GP for screening, because it drew at-
The study group consisted of nine females and eight
tention to their problems. This positive reaction to be-
males with a mean age of 47 years (range 29–65) of
ing screened is important because it illustrated that
three different ethnic origins: Dutch (n = 10), Suri-
the patients did want attention. Some patients said
namese (n = 6) and Indian (n = 1). None of the
they were unsure about their GP being the right per-
patients invited declined to participate. According to
son to go to with mental problems. Others said that
the SCID, all patients were suffering from a major de-
they had difficulties in bringing up this subject during
pressive disorder. The severity of the depressive disor-
der expressed by the HDRS score varied between 13(mild) and 32 (severe), with a mean score of 21 (mod-erate depression). Six of the 17 patients had a recurrent
depressive disorder and the co-morbid psychiatric
reaction to being screened, patients said they knew
diagnoses in seven of the 17 patients were specific
something was wrong with them, i.e. they were aware
Patients’ view on screening for depression
Patients’ view on screening for depression
I believe the time is ripe for it; it has been long enough now that
I knew something was wrong with me. People told me I was
I’ve been letting this prey on my mind. I just needed this prod.
stressed, but I didn’t know what it was exactly although I did feel
something was wrong. When I got the results of the test I knewthe test was right and now I hope it can be treated. (Pt 7)
Well, it was funny because the invitation arrived just at the time Iwas going through a bad period, and I felt things were developing
I read about depression on the Internet and it all seemed familiar
in the wrong direction. And exactly at that time the first envelope
to me. Symptoms like sleeplessness, agitation, concentration
arrived. My husband read the invitation as well and said ‘well,
problems and loss of interest I’m experiencing all this. (Pt 3)
somewhere somebody must have sensed this’, so that was quite
For the last three years I have been feeling worse and worse. I
don’t feel like doing anything and I don’t leave the house anymore except to go to work. Even when I’ve planned to potterabout the house, I just can’t get myself to do it. (Pt 6)
that they were dysfunctioning. Recognition of dysfunc-tion might make patients realize they were sufferingfrom a mental disorder like depression. In fact, all
patients were convinced they were dysfunctioning and15 of 17 patients did actually perceive themselves as
For me it’s like, when I’m depressed, I feel very sober and nega-
tive about everything. Things like shopping or being at home,everything’s negative, even the things that would normally cheerme up. Like my little nephew, normally he would cheer me up,but not when I’m depressed, like this weekend, I was feeling so
depressed that even he couldn’t get me out of this. (Pt 17)
ably influence patients’ recognition and acceptance of
Then I don’t have the energy to do anything, I’m forgetful and I
the diagnosis of depression and their need for help. In
feel life’s pointless when I’m depressed. (Pt 10)
general, most patients were well aware of the depres-sive symptoms and were able to enumerate most ofthe symptoms belonging to a depressive disorder. Thisis illustrated by the following answers to the inter-viewer’s question of how to define depression (see
My whole future has collapsed since all my investment plansfailed absolutely. Every single plan that I worked so hard for
The fact that these patients were able to enumerate
went wrong and the world around me is falling apart, and that’s
most of the criteria for depression might imply they
saw the similarity between their own symptoms and
It started after my first relationship ended, but it wasn’t that bad
the diagnosis of depression. However, in their causal
at the time. It only got worse after my last relationship broke
explanations for their symptoms, patients did not attri-
down; then I couldn’t handle it anymore, it was really too much.
I don’t think I can explain it, no, but I know what is bothering
me, I can explain that to you. What you want to call a depressionhas more to do with everything I went through before it all finally
view on being diagnosed with depression, patients
became too much for me. So really, it’s more a question of all the
started to talk about the problems they were strug-
things I didn’t deal with over the years catching up with me.
gling with, which had resulted in their dysfunctioning.
When you are trying to deal with everything at once and thenyet another setback occurs, well, that’s the last straw. (Pt 9)
They did not experience the disease depression as be-ing their main problem, but rather focused on the situ-ation either related to or causing their depressivesymptoms. Recurrent problems were difficulties in re-
Acceptance of the diagnosis of depression.
lationships with spouse or partner, loneliness, trouble
the vast majority of patients was positive about being
at work and physical problems. Other problems in-
screened and did recognize their own dysfunctioning,
cluded financial problems, parenting problems, di-
this did not automatically result in accepting the diag-
vorce, traumas in childhood (abuse, misuse and
nosis of depression. When we kept on asking about
betrayal), climacteric symptoms, bereavement, anxiety
their views on being diagnosed as depressed, nine of
and personality problems. Patients frequently ex-
17 patients said they felt some resistance to the diag-
pressed the need for help to resolve these ‘major’
nosis, as if it was going too far. Admitting to being
problems. They appeared to experience their depres-
depressed was seen as a failure and as the point of no
sive state as being a consequence of their struggle with
return. Patients also expressed a fear of stigmatization
these problems and not as the cause (see Box 4).
(see Box 5, Example 1). The last quote, like some of
Family Practice—an international journal
BOX 5. Acceptance of the diagnosis of depression
Example 1: Seeing that diagnosis in the letter makes me want to fight against it. (. . .) Not even for myself, but because of others. (. . .) I don’treally want to admit it, being afraid of others thinking ‘you see, she didn’t make it after all . . .’ (. . .) I’m afraid of becoming one of the peopleon that list at work, who have been ill, and can’t handle it. (Pt 8)
Example 2: I really don’t think that what I’m experiencing should be called a depression. People with a depression who I’ve seen just don’tknow what they’re doing anymore; they just give up, or else start drinking. I have to admit that I’ve been drinking more lately, but anyway. These people behave differently, stop going to work, stop looking after themselves, you know, these kinds of depression. For me it’s morea matter of ‘where will this end?’ It’s all useless, hopeless, helpless . . . (Pt 16)
Example 3: When I read the letter I thought it was referring to the depression I experienced in 2002. At that time I was suffering from real de-pression. I was feeling much worse then; I didn’t have any energy and didn’t feel like doing anything and slept the whole day through. Icouldn’t control my appetite. Now, I’m having some of these symptoms but not to the same extent as before. The word ‘depression’ reallydoesn’t suit the way I’m feeling today; that’s got more to do with the past. (Pt 4)
Example 4: Well, I think it’s something in my character, but yet I’m not sure about it. (. . .) But a depression, I don’t I know. I don’t think so,and I don’t want myself to stay like this. I feel like I’m going through a bad patch, a very bad patch. (Pt 13)
Example 5: Well, it depends what is meant by depression, but to me depression is something very severe. Last year I had burn out, that’s whatthe doctor said. That, I felt, was severe as well, but that was easier to accept. And also, I don’t feel that I should need to take antidepressivemedication yet. (Pt 8)
Example 6: It’s just a word you people have invented for people feeling like I do, and that’s what you call depression. They’ve just made upa name for it. (Interviewer: So do I understand you correctly that it doesn’t help you?) That’s right, I don’t feel connected to that word atall. I could never imagine myself, saying, ‘I’m depressed’. No, I just know for myself that I’ve not been feeling very well lately. (Pt 9)
the preceding ones, illustrates that depression is per-
ceived as a stigmatizing disorder. Patients also com-pared themselves with people suffering from more
In this study, we explored patients’ views on being
severe psychiatric symptoms (see Box 5, Example 2).
diagnosed as depressed in a screening programme byperforming a qualitative study. We conclude that
Another patient had suffered from a depression in
screening for depression detects a group of patients
the past. She mentioned that her former depressive
that appreciate the fact that they receive attention for
episode had been far more severe than it was this time
their problems, but who also show resistance to being
(see Box 5, Example 3). Furthermore, patients tend to
diagnosed as having depression. Three of the six
keep away from the diagnosis of depression by giving
themes that originated from the interviews are in ac-
their problems other names. They prefer to label it as
cordance with the aim of screening for depression.
a ‘bad patch’, a ‘big dip’, ‘burn out’ or ‘stress’ (see
First, patients in this study feel positive about being
Box 5, Examples 4 and 5). Some patients did not see
actively approached for screening. They express the
the purpose of labelling their symptoms as depression
need to talk about their problems but also describe
and mentioned that using the label ‘depression’ did
themselves as being hesitant to ask for help.
not clarify the situation (see Box 5, Example 6).
Secondly, patients recognize that there is something
wrong or that they are dysfunctioning or ill. This
awareness of dysfunctioning is probably one of the
the interviews was the need for help, the need for
main reasons why these patients participated in this
treatment and the kind of treatment preferred by these
screening programme. Third, patients were able to
patients. The patients’ needs differed greatly. Some
enumerate most of the DSM-IV criteria of depression
patients doubted whether they really needed treatment
and recognize these symptoms in themselves. This last
because their symptoms were not severe enough for
aspect could be accounted for by the process of
that. Others said that treatment would not help them.
screening itself, which probably stimulated their
Few patients wished to solve their problems them-
awareness of illness by exploring all the symptoms of
selves without any help. They believed asking for help
depression in a questionnaire and in the structured
would confirm their failure (see Box 6, Example 1).
We conclude that these patients, who were willing
Of the patients who appreciated receiving some
to be screened for depression and who screened posi-
help, the majority did not think positive about treat-
tive for depression, are aware of their dysfunctioning
ment that included medication (see Box 6, Example
and depressive symptoms. Feeling ashamed or doubt-
2). Taking medication was also not associated with an
ful and feeling guilty about their dysfunctioning, prob-
active approach they believed to be necessary for their
ably in combination with apathy, hampers discussion
of their problems with their GP. Therefore, screening
Patients’ view on screening for depression
Depressive disorder is, however, a syndromal diagnosis
and as such not a diagnosis with a gold standard. Itmight be possible that patients who rejected the label
Example 1: I’ve thought about contacting my former therapist,
are in fact correct, differ from the patients with a ‘true’
but this feels like a difficult step. It’s like admitting that I really
diagnosis of depressive disorder and have better out-
come.19 This standpoint suggests a rethinking of the val-
Example 2: No, I don’t believe that these pills that make you feel
idity of the clinical concept of depressive disorder in
like a zombie would be helpful, because it’s important to be
active, and enjoy things and that’s very hard when you feel numblike that. (Pt 15)
The last explanation for the difficulties being diag-
nosed with depression is based on the fact that pa-
Example 3: Well, of course I’m just a lay person, but as soon astreatments concern pills I stop believing in it. I think it’s you your-
tients linked the diagnosis of depression to treatment
self that has to solve it, pills are not the solution. (Interviewer:
and especially with medication. Patients seemed to be
‘Why not?’) Because whenever you get depressed again, you
less familiar with other therapies which target the res-
think, ‘well, the pills will solve this’. (Interviewer: ‘You mean, youbecome passive?’) It’s pure laziness you’ll get. I don’t feel good,
olution of problems at work and home like certain
so I’ll take a pill, while the problems are still there. You should
psychotherapy for depression (cognitive behaviour
deal with it yourself, and shouldn’t take pills for that. (Pt 17)
therapy and interpersonal therapy) and are as effec-tive as medication. As has been found before, patientsare not convinced of the necessity and effectiveness of
might help to make contact with these patients about
medical treatment.9–12 In fact, recent systematic re-
views have shown that medication effectiveness is
Our last three themes illustrate that depression is
overrated by drug manufacturers, researchers as well
seen as a medical concept that does not properly com-
as prescribers.20–22 It might also be possible that pa-
pare with patients’ view and experiences. In this study,
tients have former negative experiences with medica-
patients attribute their difficulties to external psycho-
tion. This probably hampers patients to accept
social problems. As a consequence, they find it diffi-
therapy for their problems based on the bio-psychiat-
cult to accept that they had been diagnosed with
depression, which they consider a disease-focused con-
The implications of our findings are that screening
cept. Patients seemed to disagree with one particular
programmes for depression are probably less success-
view on depression, namely the bio-psychiatric view.
ful because of the labelling of depression more by the
This outcome is supported by earlier studies which
psychosocial causes than by the syndromal symptom-
found that patients with a depressive disorder or anxi-
atology, the nature of the target disorder, the course
ety disorder are focused on external problems and
of symptoms, the validity of depressive disorder in pri-
their own reaction to these external problems, regard-
mary care and the limited effectiveness of (biological)
ing this as the main cause of their depressive state.9,11
treatment, which hamper the acceptance of the conse-
In their causal way of thinking it are psychosocial
problems that cause depression and not vice versa.
Four explanations for difficulties with being diag-
nosed as having depression emerge from our study.
First, the characteristics of the illness itself. Depressivesymptoms, such as guilt, feelings of failure and fatigue,
This is the first study on attitudes and views about de-
do hamper help-seeking behaviour. Furthermore,
pression of patients who recently screened positive for
patients are not able to handle external problems because
major depressive disorder. Our recruitment strategy
of depression. In fact, patients regard this as a weakness
enabled us to interview patients who accepted the di-
instead of a consequence of the depression.
agnosis as well as those who rejected the diagnosis.
For the second explanation, the course of depressive
None of the patients, diagnosed as being depressed de-
symptoms must be considered. Most patients in this
clined to participate in this study. As far as we are
study had already experienced that depressive symp-
concerned, the ethnic variation within our sample did
toms are self-limiting and a normal reaction to life
not influence the results because we could not find
stress. Depressive disorder on the other hand is more
any recurrent themes that were specific to ethnic ori-
and more considered to be a severe, chronic medical
gin. Our results are valid for patients that cooperate
disorder. Patients could be afraid that labelling symp-
with screening programmes for depression and who
toms as a depressive disorder would imply that their
screen positive. They do not relate to all primary care
symptoms are not self-limiting but chronic instead.
patients and are probably too optimistic about the
We assessed the diagnosis depressive disorder ac-
positive attitude towards screening for depression.
cording to the DSM-IV criteria by a structured inter-
The response rate to the screening programme was
view, the SCID I, which is an accepted reference
about 50%, which is not unusual in psychiatric pro-
standard to set the diagnosis in clinical settings.
grammes.23–25 One limitation was our decision to use
Family Practice—an international journal
convenience recruitment of consecutive patients rather
3 Coyne JC, Klinkman MS, Gallo SM, Schwenk TL. Short-term out-
than try to achieve maximal variation. On the other
comes of detected and undetected depressed primary care pa-tients and depressed psychiatric patients. Gen Hosp Psychiatry
hand, the main implication is that the design was less
efficient than if maximal variation were sought,
4 Gilbody S, Sheldon T, Wessely S. Should we screen for depression?
because the data were collected until saturation oc-
curred. For this reason, this is not a major limitation.
Gilbody SM, House AO, Sheldon TA. Routinely administered
questionnaires for depression and anxiety: systematic review. BMJ 2001; 322: 406–409.
6 Pignone MP, Gaynes BN, Rushton JL et al. Screening for depres-
sion in adults: a summary of the evidence for the U.S. Preven-tive Services Task Force. Ann Intern Med 2002; 136: 765–776.
7 National Screening Committee. The UK National Screening Com-
From this study, we conclude that patients with undis-
mittee’s Criteria for Appraising the Viability, Effectiveness and
closed depression, detected by our screening pro-
Appropriateness of a Screening Programme. London: HMSO,
gramme, are experiencing difficulties in accepting the
diagnosis of depression. Explanations for this are the
Dinos S, Stevens S, Serfaty M, Weich S, King M. Stigma: the feel-
ings and experiences of 46 people with mental illness. Qualita-
nature of the target disorder depression and the nega-
tive study. Br J Psychiatry 2004; 184: 176–181.
tive views about the diagnosis and treatment of de-
9 Cornford CS, Hill A, Reilly J. How patients with depressive symp-
pression. We conclude that one important criterion
toms view their condition: a qualitative study. Fam Pract 2007;
for the viability of screening programmes, the com-
10 Angermeyer MC, Beck M, Dietrich S, Holzinger A. The stigma of
plete screening programme (test, diagnostic proce-
mental illness: patients’ anticipations and experiences. Int J Soc
dures and treatment/intervention) is clinically, socially
and ethically acceptable to the target population, is
Kadam UT, Croft P, McLeod J, Hutchinson M. A qualitative study
of patients’ views on anxiety and depression. Br J Gen Pract
hard to comply within screening programmes for
depression. In this context, we recommend that the
12 Maxwell M. Women’s and doctors’ accounts of their experiences of
patients’ view about depression should be elicited be-
depression in primary care: the influence of social and moral
fore diagnosing and offering treatment for depression.
reasoning on patients’ and doctors’ decisions. Chronic Illn2005; 1: 61–71.
Aversion to being labelled as being depressed can
13 Spitzer RL, Kroenke K, Williams JB. Validation and utility of
have a deterrent effect on the willingness of patients
a self-report version of PRIME-MD: the PHQ primary care
to accept help, even though they might benefit from
study. Primary care evaluation of mental disorders. Patient
health questionnaire. JAMA 1999; 282: 1737–1744.
14 First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clin-
ical Interview for DSM-IV Axis I Disorders Patient Edition(SCID-I/P version 2.0). Translated in Dutch by Groenestijn,
MAC, Akkerhuis, GW, Kupka, RW, Schneider, N and Nolen,WA. 1999. Lisse, The Netherlands: Swets & Zeitlinger.
According to the Medical Research Involving Human
Hamilton M. A rating scale for depression. J Neurol Neurosurg
Subjects Act (WMO), formal approval for this re-
16 Pope C, Ziebland S, Mays N. Qualitative research in health care.
search project by a Medical Ethics Committee was
Analysing qualitative data. BMJ 2000; 320: 114–116.
not necessary. KAW had full access to all the data in
17 MAXqda2: Software for Qualitative Data Analysis. Berlin: VERBI
the study and takes responsibility for the integrity of
Software. Consult Sozialforschung GmbH, 2004.
18 Ritchie J, Spencer L, O’Connor W. Carrying out qualitative anal-
the data and the accuracy of the data analysis.
ysis. In Ritchie J, Lewis J (eds). Qualitative Research Practice,London: SAGE Publications Ltd, 2003: 219–225.
19 Aragones E, Pinol JL, Labad A. The overdiagnosis of depression in non-
depressed patients in primary care. Fam Pract 2006; 23: 363–368.
20 Barbui C, Furukawa TA, Cipriani A. Effectiveness of paroxetine in
the treatment of acute major depression in adults: a systematic
Funding: The Netherlands Organization for Health
re-examination of published and unpublished data from ran-
domized trials. CMAJ 2008; 178: 296–305.
21 Kirsch I, Deacon BJ, Huedo-Medina TB, Scoboria A, Moore TJ,
Mental Health (# 100.003.005 and # 100.002.021).
Johnson BT. Initial severity and antidepressant benefits:
a meta-analysis of data submitted to the Food and Drug Ad-
ministration. PLoS Med 2008; 5: e45.
22 Turner EH, Matthews AM, Linardatos E, Tell RA, Rosenthal R.
Selective publication of antidepressant trials and its influenceon apparent efficacy. N Engl J Med 2008; 358: 252–260.
23 Angst J, Bech P, Bruinvels J et al. Report on the fifth consensus
conference: methodology of long-term clinical trials in psychi-
1 Dowrick C, Buchan I. Twelve month outcome of depression in
atry. Pharmacopsychiatry 1994; 27: 101–107.
general practice: does detection or disclosure make a differ-
24 Greil W, Ludwig-Mayerhofer W, Steller B et al. The recruitment pro-
cess for a multicenter study on the long-term prophylactic treat-
2 Williams JW Jr, Pignone M, Ramirez G, Perez SC. Identifying
ment of affective disorders. J Affect Disord 1993; 28: 257–265.
depression in primary care: a literature synthesis of case-finding
25 Zullino D, Conus P, Borgeat F, Bonsack C. Readiness to partici-
instruments. Gen Hosp Psychiatry 2002; 24: 225–237.
pate in psychiatric research. Can J Psychiatry 2003; 48: 480–484.
MODELO DE BULA DO PACIENTE IDENTIFICAÇÃO DO MEDICAMENTO COVERSYL 4mg perindopril 4mg APRESENTAÇÕES: Embalagem contendo 15 ou 30 comprimidos de 4mg. USO ORAL USO ADULTO ACIMA DE 18 ANOS COMPOSIÇÃO: Cada comprimido de COVERSYL (perindopril) 4mg contém: perindopril, sal de terc-butilamina. 4,00 mg. correspondente a 3,338 mg de perindopril(DCB 06994). excipiente
The Rap Sheet Legal News for Law Enforcement in Brevard and Seminole Counties June 2002 Volume XVIII, Issue 1 Message from Once again, I am pleased to provide you with State Attorney this issue of the Rap Sheet devoted to a Norm Wolfinger summary review of the legislation passed during the 2002 regular session of the Florida legislature. I hope that this review w
 Family Practice—an international journal
Secondly, recurrent themes within the transcripts
phobia, social phobia and alcohol dependence. Six of
were selected and text fragments were sorted accord-
the 17 patients had been treated for depression in the
ing to the thematic framework. This consisted of the
following themes: (i) patients’ definition of depression;(ii) acceptance of the diagnosis of depression; (iii)
Patients’ views on screening for depression
patients’ view of causes of the depressive disorder;
We identified six consecutive themes related to the
and (iv) physical symptoms and physical co-morbidity
main subject of our study: patients’ views on screening
related to the patients’ complaints. Next, the second
for depression. These six themes were (i) reaction to
author (MvZ) independently analysed all the inter-
being screened; (ii) recognition of dysfunction; (iii)
views and added the theme ‘reaction to being
ideas about depression; (iv) differentiation of prob-
screened’. Consensus meetings between all authors
lems; (v) acceptance of the diagnosis of depression;
led to the rearrangement of themes which is presented
and (vi) consequences of the diagnosis of depression
patients were positive about the process of beingscreened for depression. They appreciated the active
approach of their GP for screening, because it drew at-
The study group consisted of nine females and eight
tention to their problems. This positive reaction to be-
males with a mean age of 47 years (range 29–65) of
ing screened is important because it illustrated that
three different ethnic origins: Dutch (n = 10), Suri-
the patients did want attention. Some patients said
namese (n = 6) and Indian (n = 1). None of the
they were unsure about their GP being the right per-
patients invited declined to participate. According to
son to go to with mental problems. Others said that
the SCID, all patients were suffering from a major de-
they had difficulties in bringing up this subject during
pressive disorder. The severity of the depressive disor-
der expressed by the HDRS score varied between 13(mild) and 32 (severe), with a mean score of 21 (mod-erate depression). Six of the 17 patients had a recurrent
depressive disorder and the co-morbid psychiatric
reaction to being screened, patients said they knew
diagnoses in seven of the 17 patients were specific
something was wrong with them, i.e. they were aware
Patients’ view on screening for depression
Patients’ view on screening for depression
I believe the time is ripe for it; it has been long enough now that
I knew something was wrong with me. People told me I was
I’ve been letting this prey on my mind. I just needed this prod.
Family Practice—an international journal
Secondly, recurrent themes within the transcripts
phobia, social phobia and alcohol dependence. Six of
were selected and text fragments were sorted accord-
the 17 patients had been treated for depression in the
ing to the thematic framework. This consisted of the
following themes: (i) patients’ definition of depression;(ii) acceptance of the diagnosis of depression; (iii)
Patients’ views on screening for depression
patients’ view of causes of the depressive disorder;
We identified six consecutive themes related to the
and (iv) physical symptoms and physical co-morbidity
main subject of our study: patients’ views on screening
related to the patients’ complaints. Next, the second
for depression. These six themes were (i) reaction to
author (MvZ) independently analysed all the inter-
being screened; (ii) recognition of dysfunction; (iii)
views and added the theme ‘reaction to being
ideas about depression; (iv) differentiation of prob-
screened’. Consensus meetings between all authors
lems; (v) acceptance of the diagnosis of depression;
led to the rearrangement of themes which is presented
and (vi) consequences of the diagnosis of depression
patients were positive about the process of beingscreened for depression. They appreciated the active
approach of their GP for screening, because it drew at-
The study group consisted of nine females and eight
tention to their problems. This positive reaction to be-
males with a mean age of 47 years (range 29–65) of
ing screened is important because it illustrated that
three different ethnic origins: Dutch (n = 10), Suri-
the patients did want attention. Some patients said
namese (n = 6) and Indian (n = 1). None of the
they were unsure about their GP being the right per-
patients invited declined to participate. According to
son to go to with mental problems. Others said that
the SCID, all patients were suffering from a major de-
they had difficulties in bringing up this subject during
pressive disorder. The severity of the depressive disor-
der expressed by the HDRS score varied between 13(mild) and 32 (severe), with a mean score of 21 (mod-erate depression). Six of the 17 patients had a recurrent
depressive disorder and the co-morbid psychiatric
reaction to being screened, patients said they knew
diagnoses in seven of the 17 patients were specific
something was wrong with them, i.e. they were aware
Patients’ view on screening for depression
Patients’ view on screening for depression
I believe the time is ripe for it; it has been long enough now that
I knew something was wrong with me. People told me I was
I’ve been letting this prey on my mind. I just needed this prod.