Levitra has a minimal amount of contraindications which has increased its popularity viagra uk You can buy quality certified medications from us at an affordable price.
Viagra deafnesssensorineural hearing loss and phosphodiesterase5 inhibitors
Rhinological and Otological Society, Inc.
Viagra Deafness—Sensorineural Hearing Loss andPhosphodiesterase-5 Inhibitors
Afroze Shah Khan, MRCS;* Zishan Sheikh, MBBS;* Shahnawaz Khan, MBBS; Raghav Dwivedi, MS;
Background: Viagra and PDE-5 inhibitors use has mushroomed since its launch over a decade ago. A growing body of
evidence indicates significant morbidity associated with the side effect profile of this class of drug. Hearing loss associatedwith PDE-5 inhibitor use has recently been reported, but few studies have evaluated the causal link.
Aim: To review and scrutinise the current literature on the subject and propose possible physiologic mechanisms and to
investigate the global reporting of this side effect.
Methods and Materials: Pharmacovigilance agencies around North America, Europe, and Australasia were contacted
requesting reports of hearing loss associated with PDE-5 inhibitors. Reports were scrutinised to exclude those where otherscauses of hearing loss existed.
Results: Forty-seven cases of sensorineural hearing loss with a temporal association with PDE-5 inhibitor ingestion
were obtained from both published literature and pharmacovigilance agencies. Cases had a mean age 56.6 years, male-to-female ratio of 7:1. Eighty-eight percent of reports were unilateral with an even left/right distribution. Hearing loss occurredwithin 24 hours of ingestion of PDE-5 inhibitor in 66.7% (n ¼ 18) of cases. Sildenafil accounted for over 50% of cases.
Conclusion: There is increasing evidence that PDE-5 inhibitors may induce sensorineural hearing loss via plausible
physiological mechanisms. There needs to be more awareness of this disabling side effect among healthcare professionalsresponsible for prescribing this drug.
Key Words: Hearing loss, deafness, sensorineural, sildenafil, viagra, phosphodiesterase inhibitors. Level of Evidence: N/A.
hearing loss with PDE-5 inhibitor use.7 Two successive
Phosphodiesterase-5 (PDE-5) inhibitors, originally
experimental studies also support a possible causal
developed for the treatment of angina, are the most com-
link.8,9 Most reports of PDE-5 inhibitor related SSHL
have come from the Food and Drug Agency (FDA) in the
dysfunction (ED). They are largely well tolerated in clin-
United States. To ascertain the global experience of this
ical practice and have recently also used proved useful
phenomenon we have surveyed pharmacovigilance agen-
in the treatment of pulmonary hypertension.1–3
cies across America, Europe, and Australasia.
Sudden sensorineural hearing loss (SSHL) is a dis-
tressing illness with up to one-third of patients left with
permanent hearing impairment. It has an estimated
In an effort to assess the number of suspected cases, phar-
incidence of 5–20 per 100,000 people per year. It is diag-
macovigilance agencies in Europe, the Americas, East Asia, and
nosed to be mostly idiopathic, but viral or microvascular
Australasia were contacted for adverse events of sudden hear-
aetiologies are thought to be responsible.4
ing loss in patients taking PDE-5 inhibitors as shown in Table
Recently, two authors have reported cases of SSHL
I. Cases were individually analyzed and those with other causes
occurring after PDE-5 inhibitor ingestion.5,6 An epide-
of hearing loss present were excluded from the series. In addi-
miologic study has also suggested a higher risk of
tion, the temporality, PDE-5 inhibitor ingested and laterality ofhearing loss was obtained.
From the Ear, Nose and Throat Department (A.S.K., E.B.), Charing
C r o s s H o s p i t a l , L o n d o n , U n i t e d K i n g d o m ; D e p a r t m e n t o fGastroenterology (Z.S.), Stoke Mandeville Hospital, Buckinghamshire,United Kingdom; Royal Marsden Hospital (S.K., R.C.D.), London, United
A total of 53 cases of hearing loss-associated with
Editor’s Note: This Manuscript was accepted for publication
PDE-5 inhibitor use were reported to various pharmaco-
vigilance agencies. After a review of individual case
The authors have no financial disclosures for this article.
histories five were deemed to be related to other estab-
The authors have no conflicts of interest to declare.
lished causes of hearing loss such as otitis media or
*A.S.K. and Z.S. are joint first authors.
Send correspondence to Mr. Afroze Shah Khan, Ear, Nose and
Meniere’s and these were excluded. Of remaining 47
Throat Department, Charing Cross Hospital, Fulham Road, London SW3
cases, 43 were submitted by pharmacovigilance agencies
and four were from published literature (Table I). The
mean age at presentation was 56.6 years with a male-to-
Showing Details of All Reported Cases of PDE-5 Inhibitor-Associated Hearing Loss.
USA: United States of America, NR: Not recorded, d: Days, Y: Years.
female ratio of 7:1. Laterality was recorded in 70% (n ¼
dose dependent. More serious side effects are rare and
33) of reports and of these hearing loss was unilateral in
include temporary loss of vision, retinopathy, seizures,
88% (n ¼ 29) and bilateral in 22% (n ¼ 4). There was
myocardial infarction, ventricular arrhythmia, sudden
even distribution of hearing loss affecting the right and
cardiac death, cerebrovascular haemorrhage, and tran-
left sides. The interval between onset of hearing loss
sient ischaemic attacks.13,14 It was not until 2007 that a
and PDE-5 inhibitor ingestion was recorded in 57.4% (n
case of SSHL was reported as a potential side effect of
¼ 27) of reports. Hearing loss occurred within 24 hours
of PDE-5 inhibitor use in 66.7% (n ¼ 18) of reports. Only
SSHL has been defined as hearing loss of at least 30
38.3% (n ¼ 18) of the total reports confirmed the hearing
dB in three or more continuous frequencies that occurs
loss as sensorineural in nature. Sildenafil had the larg-
within 72 hours of symptoms onset. It is a disturbing dis-
est number of individual reports at 29 cases, followed by
order that is usually unilateral with a varied incidence,
tadalafil (n ¼ 10) and vardenafil (n ¼ 7).
with some authors estimating 15,000 cases diagnosed
In addition to the 47 cases mentioned, raw data
per year world wide.4 The true incidence is thought to be
from the FDA’s Adverse Events Reporting System
far higher than reported in the literature, as only a frac-
(AERS) index yielded an additional 223 logged reports
tion of cases present for medical assessment.
submitted after 2007 where hearing loss was reported
Its etiology is controversial and often labeled as idi-
with PDE-5 inhibitor ingestion. However, as there were
opathic, because a cause is found in as little as 10% of
no accompanying case histories these could not be
patients.15 Vascular disease, autoimmune conditions,
included in the final analysis. The FDA also noted that
labyrinthine membrane rupture, viral infection, and psy-
in clinical trials of PDE-5 inhibitors, of the nearly
chosomatic disorders are all contenders as potential
60,000 subjects across four trial studies, there were 17
causes.16 The treatment of SSHL is no less controversial
cases of temporally associated sudden hearing loss.
than its etiology and, in clinical practice, is often
Again, no further case histories existed for these, and
directed against a whole spectrum of possible causes. To
they were not included in final the analysis.
cover possible vascular pathology vasodilators and rheo-logic agents have been used to reverse tissue hypoxia. As a significant proportion of patients report a recent vi-
ral illness, antiviral agents such as Acyclovir are
PDE-5 inhibitors were first used to study cell and
frequently used despite uncertain hearing improvement.
vascular physiology in the 1970s. However, it was not
Hyperbaric oxygen has also been used and is thought to
until 1995 that their physiologic importance in regulat-
work by increasing oxygen tension in auditory tissue,
ing vascular smooth muscle tone was understood.9a
but its clinical benefit is uncertain at present. Repairs of
Sildenafil was the first drug in this class developed for
oval and round window perilymph fistulae can be per-
commercial use. Synthesized at Pfizer’s laboratories in
formed for cases of SSHL with positive fistula tests or a
Sandwich, Kent, it was initially studied for use in hyper-
history recent trauma, but diagnosis is difficult and the
tension and angina pectoris. Phase two clinical trials
benefit uncertain.17 Anti-inflammatory treatment with
showed that the drug had little effect on angina, but cru-
both oral and intratympanic corticosteroids has been
cially observed that it could induce marked penile
studied in cases of SSHL and was previously considered
erections. Sildenafil citrate was patented in 1996, and
as a gold standard in North America. However, a recent
approved for use by the FDA in 1998 as the first oral
Cochrane review has shown that their clinical value is
treatment for erectile dysfunction in the United States.
open to debate.18 In fact, a meta-analysis recently stated
Annual sales of Viagra in the period 1999–2001 exceeded
no treatment for SSHL has been validated by large
$1 billion. Since then, other PDE-5 inhibitors have been
high-quality randomized controlled trials, probably due
developed for use in ED with several countries produc-
Mukherjee et al.5 first reported a case of SSHL in
It is estimated that over 20 million men in the
a 44-year-old man occurring 15 days after taking Silde-
United States have used Sildenafil, and over 40 million
nafil, 50 mg daily, in 2007. The patient had taken the
prescriptions have been issued worldwide since its
drug for 12 days continuously before developing pro-
launch.10 In 2007, Sildenafil was the 65th most popular
found bilateral hearing loss that was preceded by
drug prescribed, exceeding such common drugs as Tyle-
tinnitus but no other symptoms. Sensorineural hearing
nol-codeine and albuterol in the United States. It is
loss was subsequently confirmed on audiometric test-
estimated that one in five men in the United States over
the age of 40 have tried sildenafil.11 In the United King-
treatment and eight cycles of carbogen therapy, there
dom, pilot ‘‘pharmacist led prescribing’’ schemes have
was no improvement in his symptoms. This resulted in
lead to increased availability of Sildenafil, and the drug
the FDA reviewing its postmarketing data on 113 cases
of SSHL in patients taking PDE-5 inhibitors. Out of
Sildenafil has proved to be an efficacious drug for
this, a total of 23 cases were deemed to have been
treating for ED.1 Its most common side effects are flush-
potentially due to PDE-5 inhibitors. The FDA has since
ing, headache, blocked nose, dyspepsia, and dizziness
added SSHL onto the list of potential side effects for
with some studies showing that up to one-third of men
all PDE-5 inhibitors and is negotiating with manufac-
taking the drug experience these with long-term use.1,2
turers to feature this effect more prominently on its
The frequency of these side effects appears to be fairly
Fig. 1. Diagram illustrating potential physiologic pathways for PDE-5 inhibitor-mediated hearing loss. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Maddox et al.5 subsequently combined these 23
high-dose Sildenafil during a 135-day period. Hearing
cases with two novel reports in a review and found a
loss was evaluated by recording auditory middle ear la-
strong temporal association between drug ingestion and
tency responses and otoacoustic emissions. High doses of
the development of SSHL. They found that 88% (n ¼ 15/
Sildenafil increased hearing thresholds as measured by
17) of patients in their series who reported developing
auditory brainstem responses. It also delayed the latency
SSHL had ingested a PDE-5 inhibitor 24 hours prior to
of both auditory brainstem responses and auditory mid-
the development of symptoms. Of these 15 patients, 87%
dle ear responses. This demonstrated that Sildenafil
(n ¼ 13/15) had symptoms beginning less than 12 hours
administration at high doses induces hearing impair-
In this current analysis we added a further 23
More recently, Okuyucu et al.8 have performed the
reports to the existing 26 in the literature. On further
only prospective observational study in humans to date.
review of FDA data analyzed by Maddox et al.,5 it was
Eighteen patients who had been using a PDE-5 inhibitor
found that four cases had comorbid otologic disease that
for ED were studied. Audiometric testing was carried out
would account for the hearing loss. The patient demog-
on all patients between frequencies 250 and 16,000 Hz
raphy in the current series was similar to those
prior to and after 1, 5, and 72 hours of 10 mg vardenafil
ingestion. Four patients demonstrated a statistically sig-
observed in 66.7% of cases, where hearing loss occurred
within 24 hours of PDE-5 inhibitor ingestion. This is
compatible with ototoxic criteria within 72 hours of drug
lower than that reported by Maddox et al. However, this
ingestion. In addition, all patients showed a significant
difference is removed if the four suspect cases of hearing
unilateral threshold decrease at 10,000 Hz. However, all
loss are excluded from the 15 cases they reported as
hearing loss resolved with discontinuation of the drug.
having significant temporality. The overwhelming major-ity of hearing loss appears to be unilateral, consistentwith both Maddox et al. as well as the FDA’s own analy-
sis of its postmarketing safety data. Sildenafil remains
Nitrous oxide–cyclic GMP pathway. The nitrous
the most commonly implicated PDE-5 inhibitor with
oxide (NO)/cyclic guanosine monophosphate (cGMP)
hearing loss, reflecting the fact that it is also the most
pathway is an established major regulatory system in
cochlear physiology and has been implicated in the
To date, only two studies have investigated the pos-
pathophysiology of hearing loss.20 It is this pathway
sibility of a direct causal association between PDE-5
that is regulated by the PDE-5 inhibitor class of drugs
inhibitor ingestion and hearing loss. A recent in vivo
(Fig. 1). It is the mechanism that induces smooth muscle
study assessed hearing thresholds in mice injected with
relaxation in endothelial cells. NO activates guanylate
cyclase, which converts guanosine triphosphate (GTP)
Nuclear factor-kappa beta (NF-jB) is another im-
into to guanosine monophosphate (GMP). This depletes
portant regulator of the inflammatory cellular stress
intracellar calcium stores to cause smooth muscle relax-
response, and apoptosis and is found in significant quan-
ation. Smooth muscle relaxation induces vasodilation in
tities in the cochlea. Based on this, it has been
the corpus cavernosum vessels to result in penile erec-
postulated as a possible etiologic agent in SSHL of all
tion. The production of cGMP is regulated by PDE-5,
causes.29 However, there are no physiologic studies that
which recycles cGMP to GTP. Sildenafil and other PDE-
corroborate a causal ototoxic link. Lang et al.30 (2006)
5 inhibitors act to inhibit the breakdown of cGMP and
showed that knock out mice lacking the gene for the p50
hence potentiate the smooth muscle relaxation that
subunit of NF-jB, suffered accelerated auditory nerve
degeneration induced by noise and aging. This suggests
NO and cGMP have been implicated in the litera-
that NF-jB may in fact be otoprotective rather than a
ture to exert ototoxic effects via secondary messengers.
Blasits et al.21 (2000) conducted an experimental studyinto the effect of NO donor sodium nitroprusside on gapjunction electrical coupling in Deiter’s cells (cells sup-
porting primary hair cells) in guinea pig cochlea. It was
In our review we found 47 reports implicating PDE-
found that the introduction of sodium nitroprusside
5 inhibitors as a cause for SSHL. However, there are at
induced uncoupling of the gap junctions, a function nec-
least a further 240 potential cases from clinical and
essary for maintaining normal cochlear sensory function.
recent FDA adverse events reports where PDE-5 inhibi-
It was likewise observed that a cGMP analogue 8-
tors may be related to hearing loss. However, due to
bromo-cGMP also uncouples Deiter’s cells, whereas an
incomplete data and case histories no further comment
NO-synthase inhibitor blocked this effect. Known oto-
can be made with respect to these. In the course of our
toxic drugs like gentamicin have also been known to
study we have noted a large variance in the detail and
cause uncoupling in Deiter cell gap junctions.22 Hence,
format of individual adverse event reports between the
as a potentiator of the NO/cGMP pathway PDE-5 inhibi-
various pharmacovigilance agencies contacted. Overall,
tors can may induce ototoxicity in a similar fashion.
there also was a poor response rate from national phar-
In an in vivo study Chung et al.23 (2007) studied
macovigilance agencies and transnational organizations
the effect of halothane and isolfurane, known NO-cGMP
such as the EMEA. The World Health Organization
pathway inhibitors, in mice exposed to broad band white
(WHO) Collaborating Centre for International Drug
noise designed to simulate noise induced hearing loss.
Monitoring based at Uppsala was also contacted. How-
After 1 week of exposure, it was found that both anaes-
ever, due to prohibitive administrative fees, in excess of
thetic agents had a protective effect, hence suggesting
£2,000 (Great British Pounds), this information could
the involvement of cGMP in mediating ototoxicity.
In their case series Maddox et al.5 considered that
as SSHL is a relatively common condition and that, as
PDE-5 inhibitors like Sildenafil are frequently pre-
The NO driven accumulation of intracellular cGMP
scribed drugs, it is possible that reported cases simply
activates various protein kinases and nuclear factors that
reflect the normal incidence of SSHL in this patient pop-
act as secondary messengers, activating various cellular
processes. Of interest is the activation of various mitogen-
prescriptions of Sildenafil were issued in a year then
activated protein (MAP) kinases. These protein kinases
based on an incidence of 10 per 100,000 one would
respond to extracellular stimuli and regulate gene expres-
expect 440 cases of SSHL in this population group
sion, mitosis, cell differentiation, and apoptosis. MAP
yearly. They further asserted that if Sildenafil was taken
kinase c-Jun N-terminal (JNKs) and the p38 isoforms
once monthly then 15 cases of SSHL would occur within
have been shown to be involved in the cellular stress
24 hours of Sildenafil ingestion. However, this extrapola-
response.24,25 The JNK proteins in particular have been
tion is entirely speculative and based on assumptions
shown to be activated within cochlear hair cells during
about the true incidence of SSHL and PDE-5 inhibitor
cellular stress in vitro. Yilkoski et al.26 (2002) conducted
usage, both of which are poorly understood and recog-
experiments in guinea pigs by injecting one group with
nized. Also, adverse drug reactions are frequently
gentamicin and another with gentamicin and CEP-1347,
unrecognized and underreported. A recent systemic
a nonprotein inhibitor of the JNK pathway. They found
review estimated underreporting rates as high as 94%.31
that CEP-1347 inhibition of JNK attenuated aminoglyco-
Another important consideration is that although
side induced cochlear hair cell damage. Wang et al.27
the original case reported by Mukherjee et al.5 was of
(2003) reproduced these results with D-JNK-1, another
bilateral SSHL, 96% of subsequent cases of suspected
inhibitor of JNKs, injected into guinea pig cochlear cell
PDE-5 inhibitor-induced SSHL have been unilateral. It
cultures. Once again, JNK inhibition provided an otopro-
is counterintuitive that a drug that has a systemic dis-
tective effect against neomycin and noise-induced hair
tribution should affect hearing asymmetrically. However,
cell toxicity. Wei et al.28 (2005) used minocycline, an inhib-
gentamicin, an established ototoxic drug, has been
itor of MAP kinase p38, on rat cochlear explants treated
shown to induce unilateral and asymmetrical bilateral
with gentamicin. It was shown that p38 inhibition was
hearing loss.28 Furthermore, in the only prospective
otoprotective against cochlear hair cell death.
study to look at PDE-5 inhibitor ingestion and SSHL, a
unilateral threshold decrease was observed in all four
3. Montani D, Chaumais MC, Savale L, et al. Phosphodiesterase type 5
inhibitors in pulmonary arterial hypertension. Adv Ther 2009;26:
patients who suffered ototoxicity.8 This implies that lat-
erality of hearing loss may have little impact on
4. Byl FM. Sudden hearing loss: eight years’ experience and suggested prog-
excluding causality in drug induced ototoxicity.
nostic table. Laryngoscope 1984;94:647–661.
5. Mukherjee B, Shivakumar T. A case of sensorineural deafness following
The temporality between PDE-5 inhibitor ingestion
ingestion of sildenafil. J Laryngol Otol 2007;121:395–397.
and the onset of SSHL has been cited to support a
6. Maddox PT, Saunders J, Chandresekhar SS. Sudden hearing loss from
PDE-5 Inhibitors: a possible cellular stress etiology. Laryngoscope 2009;
causal relationship. In the aforementioned Korean study
in mice, high-dose Sildenafil induced a significant
7. McGwin G. Phosphodiesterase type 5 inhibitor use and hearing impair-
ment. Arch Otolaryngol Head Neck Surg 2010;136:488–492.
decrease in brainstem responses to auditory stimuli after
8. Okuyucu S, Guven OE, Akoglu E, Uc¸ar E, Dagli S. Effect of phosphodies-
15 days of continuous treatment. In humans this ototox-
terase-5 inhibitors on hearing. J Laryngol Otol 2009;123:718–722.
9. Hong BN, Yi TH, Kim SY, Kang TH. High dosage sildenafil induces hear-
icity appears to manifest far earlier. In the case series
ing impairment in mice. Biol Pharm Bull 2008;31:1981–1984.
by Maddox et al. 88% of patients developed SSHL within
9a. Coste H, Grondin P. Characterization of a novel potent and specific inhibi-
24 hours of PDE-5 inhibitor ingestion. This may be an
overestimation, as our analysis showed only 62% of
10. CNN online (2007). Impotence drugs may increase risk for sudden hearing
loss. Available at: http://edition.cnn.com/2007/HEALTH/10/18/hearin-
patients developing hearing loss within this time. In
g.loss/. CNN site. Accessed: November 6, 2009.
support of this temporality, Okuyucu et al.8 showed a
11. The Wall Street Journal Online. Viagra is misunderstood despite name
recognition. [online]. Urological Sciences Research Foundation site.
significant decrease in hearing thresholds within 24
http://www.usrf.org/breakingnews/bn_111202_viagra/bn_
hours of drug ingestion in all affected patients.
111202_viagra.html. Accessed on May 22, 2010.
It has to be acknowledged that there is a lack of
12. Mayor S. UK pilot allows pharmacists to supply sildenafil without pre-
direct causal evidence for SSHL induced by PDE-5 inges-
13. Christiansen E, Guirguis WR, Cox D, Osterloh IH, Sildenafil Multicentre
tion and the mechanisms by which they cause ototoxicity
Study Group. Long-term efficacy and safety of oral ViagraV
citrate) in men with erectile dysfunction and the effect of randomised
at the cellular level. However, drug-induced ototoxicity is
treatment withdrawal. Int J Impotence Res 2000;12:177–182.
poorly understood, and no one physiological pathway has
14. U.S. Food and Drug Administration (2009). Information for Healthcare
Professionals: Sildenafil (marketed as Viagra and Revatio), Vardenafil
been proven to be involved. The NO/cGMP pathway has
(marketed as Levitra), Tafdalafil (marketed as Cialis) [online]. FDA site.
been shown to mediate ototoxicity and regulate normal
Available from: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrug-SafetyInformationforPatientsandProviders/ucm124841.htm. Accessed on
cochlear hair cell function. It is postulated that this occurs
through the induction of specific MAP kinases such as
15. Loughan S. Management of sudden sensorioneural hearing loss: a consul-
tant survey. J Olaryngol Otol 2000;114:837–839.
JNKs and p38, which we have discussed (Fig. 1). However,
16. Suckfull M. Perspectives on the pathophysiology and treatment of sudden
there is no experimental study that demonstrates NO/
idiopathic sensorineural hearing loss. Dtsch Arztebl 2009;106:669–676.
17. Grundfast KM, Bluestone CD. Sudden or fluctuating hearing loss and ver-
cGMP potentiates ototoxicity via these mediators or that
tigo in children due to perilymph fistula. Ann Otol Rhinol Laryngol
PDE-5 inhibitors significantly induce NO/cGMP and its
18. Wei BPC, Mubiru S, O’Leary S. Steroids for idiopathic sudden sensorineu-
secondary messengers in the auditory apparatus.
ral hearing loss. Cochrane Database Syst Rev 2006;CD003998. DOI:10.1002/14651858.CD003998.pub2.
19. Conlin AE, Parnes LS. Treatment of sudden sensorineural hearing loss.
Arch Otolaryngol Head Neck Surg 2007;113:582–586.
20. Fessenden JD, Schacht J. The nitric oxide/cyclic GMP pathway: a
Sildenafil and other PDE-5 inhibitors are commonly
potential major regulator of cochlear physiology. Hear Res 1998;118:
prescribed drugs for the treatment of a nonlife-threaten-
21. Blasits S, Maune S, Santos-Sacchi J. Nitric oxide uncouples gap junctions
ing condition. Although side effects are commonly mild
of supporting Deiters cells from Corti’s organ. Eur J Physiol 2000;440:
and transient, serious adverse reactions have been
22. Santos-Sacchi J. Isolated supporting cells from the organ of Corti: some
described. Sildenafil has been implicated as a causative
whole cell electrical characteristics and estimates of gap junctional con-
agent in SSHL. There is a strong temporal association
23. Chung JW, Ahn JH, Kim JY, et al. The effect of isoflurane, halothane and
and plausible physiologic mechanisms described in the
pentobarbital on noise-induced hearing loss in mice. Int Anesth Res Soc
literature to account for this. Medical practitioners
involved in the prescription of these drugs need to be
24. Zuo Z, Tichotsky A, Johns R. Halothan and isoflurane inhibit vasodilation
due to constitute but not inducible nitric oxide synthase: implications
vigilant about this potential side effect and its disabling
for the site of anesthetic inhibition of the nitric oxide/guanylyl cyclase
consequences. Patients must be counseled appropriately
signaling pathway. Anaesthesiology 1996;84:1156–1165.
25. Wang J. A peptide inhibitor of c-Jun N-terminal kinase protects against
before starting treatment. With patents for Sildenafil
both aminoglycoside and acoustic trauma-induced auditory hair cell
expiring between 2011–2013, cheaply available generic
death and hearing loss. J Neurosci 2003;23:8596–8607.
26. Ylikoski J. Blockade of c-Jun N-terminal kinase pathway attenuates gen-
versions are likely to result in a significant increase in
tamicin-induced cochlear and vestibular hair cell death. Hear Res 2002;
the usage of these drugs. The FDA in the Untied States
27. Wei X, Zhao L, Liu J, Dodel RC, Farlow MR, Du Y. Minocycline pervents
has already taken steps to have this risk more promi-
nently advertised. Healthcare professionals and organi-
phosphorylation and caspase 3 activation. Neuroscience 2005;131:–513–521.
zations in the United Kingdom need to follow suit.
28. Fausti SA. Detection of aminoglycoside ototoxicity by high-frequency au-
ditory evaluation: selected case studies. Am J Otol 1984;5:177–182.
29. Lang H, Schultz BA, Zhou D, Smythe N, Spicer SS, Schmiedt RA. Nu-
clear factor-jB deficiency is associated with auditory nerve degenera-tion and increased noise-induced hearing loss. J Neurosci 29;26:
1. McMahon C, Samali R, Johnson H. Efficacy, safety and patient acceptance
of sildenafil citrate as treatment for erectile dysfunction. J Urol 2000;
30. Hazell L, Shakir SA. Under-reporting of adverse drug reactions: a system-
atic review. Drug Safety 2006;29:385–396.
2. Sergio G, Brannigan RE, Spitz A, Orejuela FJ, Lipshultz LI, Kim ED.
31. Merchant SN, Adams JC, Nadol JB. Pathology and pathophysiology of idi-
Side effect profile of sildenafil citrate (Viagra) in clinical practice. Adult
opathic sudden sensorineural hearing loss. Otol Neurotol 2005;26:
1. Title of Proposal: Anthropogenic Influence on Tetracycline Resistance in a Rapidly Urbanizing Texas Stream 2. Focus Category: NON POINT POLLUTION ; SURFACE WATER ; WATER QUALITY 3. Keywords: antibiotic resistant genes, central Texas, gene transfer, water quality 4. Duration: March 1, 2010 through February 28, 2011 5. Federal Funds Requested. $5,000 6. Non-Federal (mat
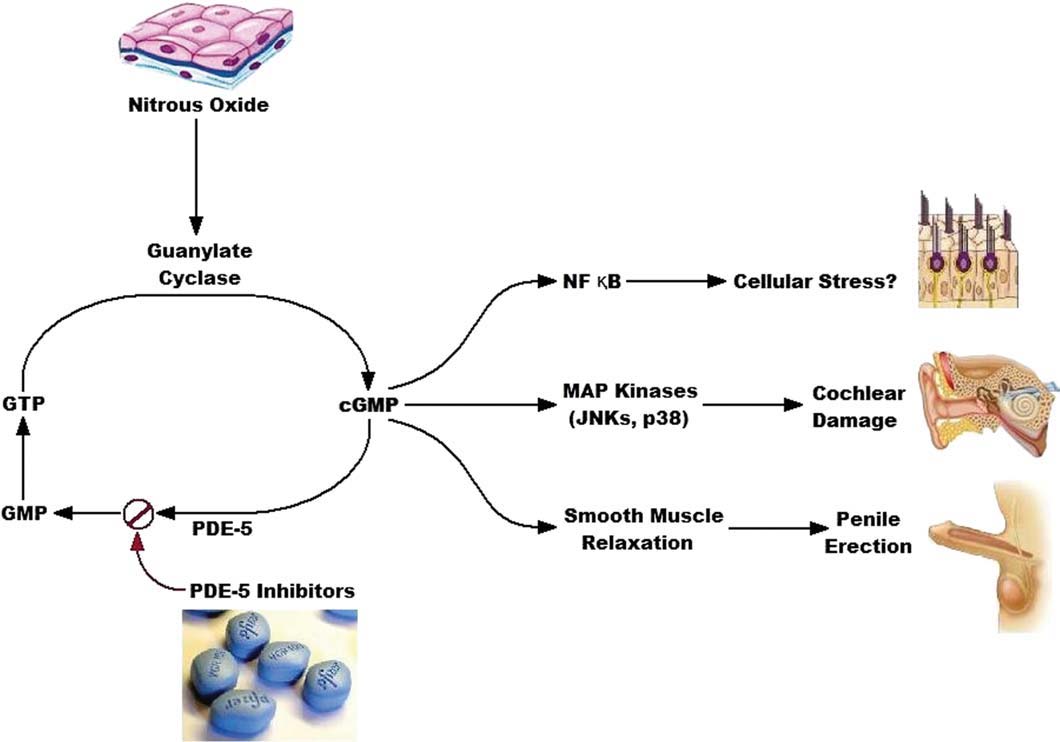 Fig. 1. Diagram illustrating potential physiologic pathways for PDE-5 inhibitor-mediated hearing loss. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Maddox et al.5 subsequently combined these 23
high-dose Sildenafil during a 135-day period. Hearing
cases with two novel reports in a review and found a
loss was evaluated by recording auditory middle ear la-
strong temporal association between drug ingestion and
tency responses and otoacoustic emissions. High doses of
the development of SSHL. They found that 88% (n ¼ 15/
Sildenafil increased hearing thresholds as measured by
17) of patients in their series who reported developing
auditory brainstem responses. It also delayed the latency
SSHL had ingested a PDE-5 inhibitor 24 hours prior to
of both auditory brainstem responses and auditory mid-
the development of symptoms. Of these 15 patients, 87%
dle ear responses. This demonstrated that Sildenafil
(n ¼ 13/15) had symptoms beginning less than 12 hours
administration at high doses induces hearing impair-
In this current analysis we added a further 23
More recently, Okuyucu et al.8 have performed the
reports to the existing 26 in the literature. On further
only prospective observational study in humans to date.
Fig. 1. Diagram illustrating potential physiologic pathways for PDE-5 inhibitor-mediated hearing loss. [Color figure can be viewed in theonline issue, which is available at wileyonlinelibrary.com.]
Maddox et al.5 subsequently combined these 23
high-dose Sildenafil during a 135-day period. Hearing
cases with two novel reports in a review and found a
loss was evaluated by recording auditory middle ear la-
strong temporal association between drug ingestion and
tency responses and otoacoustic emissions. High doses of
the development of SSHL. They found that 88% (n ¼ 15/
Sildenafil increased hearing thresholds as measured by
17) of patients in their series who reported developing
auditory brainstem responses. It also delayed the latency
SSHL had ingested a PDE-5 inhibitor 24 hours prior to
of both auditory brainstem responses and auditory mid-
the development of symptoms. Of these 15 patients, 87%
dle ear responses. This demonstrated that Sildenafil
(n ¼ 13/15) had symptoms beginning less than 12 hours
administration at high doses induces hearing impair-
In this current analysis we added a further 23
More recently, Okuyucu et al.8 have performed the
reports to the existing 26 in the literature. On further
only prospective observational study in humans to date.