Levitra has a minimal amount of contraindications which has increased its popularity priligy uk You can buy quality certified medications from us at an affordable price.
Ma003clu.edis.at
I n fl u e n c e o f L e t r o z o l e a n d A n a s t r o z o l e o n T o t a l B o d y A r o m a t i z a t i o n a n d P l a s m a E s t r o g e n L e v e l s i n P o s t m e n o p a u s a l B r e a s t C a n c e r P a t i e n t s E v a l u a t e d i n a R a n d o m i z e d , C r o s s - O v e r S t u d y
By Ju¨rgen Geisler, Ben Haynes, Gun Anker, Mitch Dowsett, and Per Eystein Lønning
Purpose: To compare the effects of the two novel, treatment with anastrozole (mean percentage inhibi- potent, nonsteroidal aromatase inhibitors anastrozole tion in the whole group, 97.3%) but in none of the 12 and letrozole on total-body aromatization and plasma patients during treatment with letrozole (> 99.1% sup- estrogen levels. pression in all patients; Wilcoxon, P ؍ .0022, compar- Patients and Methods: Twelve postmenopausal ing the two drug regimens). Treatment with anastro- women with estrogen receptor–positive, metastatic zole suppressed plasma levels of E1, E2, and E1S by a breast cancer were treated with anastrozole 1 mg mean of 81.0%, 84.9%, and 93.5%, respectrively, orally (PO) and letrozole 2.5 mg PO once daily, each whereas treatment with letrozole caused a correspond- given for a time interval of 6 weeks in a randomized ing decrease of 84.3%, 87.8% and 98.0%, respectively. sequence. Total-body aromatization was determined The suppression of E1 and E1S was found to be signifi- before treatment and at the end of each treatment cantly better during treatment with letrozole compared period using a dual-label isotopic technique involving with anastrozole (P ؍ .019 and .0037, respectively). isolation of the metabolites with high-performance liq- Conclusion: This study revealed letrozole (2.5 mg uid chromatography. Plasma levels of estrone (E1), once daily) to be a more potent suppressor of total- estradiol (E2), and estrone sulfate (E1S) were deter- body aromatization and plasma estrogen levels com- mined in samples obtained before each injection using pared with anastrozole (1 mg once daily) in postmeno- highly sensitive radioimmunoassays. pausal women with metastatic breast cancer. Results: Pretreatment aromatase J Clin Oncol 20:751-757. 2002 by American from 1.68% to 4.27%. On-treatment levels of aro- Society of Clinical Oncology. matase were detectable in 11 of 12 patients during
AROMATASE INHIBITION is a well-established concentrations to stimulate tumor cell growth,7 indirectly
treatment modality for postmenopausal women with
supports the hypothesis that the degree of estrogen suppres-
hormone-sensitive metastatic breast cancer.1 Recently, sev-
sion may be of importance for clinical outcome. Clinical
eral new aromatase inhibitors shown to be more potent and
support for such clinical-pharmacologic relationships is
less toxic compared with the first and second generation
provided by the greater efficacy of letrozole 2.5 mg daily
aromatase inhibitors have become available.2
compared with aminoglutethimide 500 mg daily3 together
Anastrozole (Arimidex; Zeneca Pharmaceuticals [Astra-
with previous findings that letrozole8 inhibits whole-body
Zeneca], Macclesfield, United Kingdom) and letrozole (Fe-
aromatization by approximately 99% compared with an
mara; Novartis Pharmaceuticals, Basel, Switzerland) are
inhibition of approximately 90% recorded with aminoglu-
two third-generation, highly potent, nonsteroidal aromatase
inhibitors used for the treatment of advanced breast cancerin postmenopausal patients. Anastrozole and letrozole, aswell as the steroidal aromatase inactivator exemestane, haverevealed clinical superiority compared with megestrol ace-tate or aminoglutethimide as second-line therapy for meta-
From the Department of Oncology, Haukeland University Hospital,
static breast cancer in postmenopausal women.3-6 Currently,
Bergen, Norway; and the Academic Department of Biochemistry, Royal
all these drugs are under evaluation as first-line therapy for
Marsden Hospital, London, United Kingdom.Submitted September 18, 2000; accepted October 12, 2001.
metastatic disease and in the adjuvant setting. Supported in part by grants from the Norwegian Cancer Society,
Clinical studies have compared each of these novel
Oslo, Norway, and Novartis Pharmaceuticals, Basel, Switzerland.
aromatase inhibitors to conventional therapy, but so far, no
Presented in part at the Thirty-Sixth Annual Meeting of the American
study has compared the in vivo biochemical efficacy or
Society of Clinical Oncology, New Orleans, LA, May 20-23, 2000.
clinical effects of third-generation aromatase inhibitors head
Address reprint requests to P.E. Lønning, MD, PhD, Department ofOncology, Haukeland University Hospital, 5021 Bergen, Norway;
to head. The finding that these novel drugs show clinical
superiority compared with conventional treatment, together
2002 by American Society of Clinical Oncology.
with recent in vitro studies revealing estrogens in low
Journal of Clinical Oncology, Vol 20, No 3 (February 1), 2002: pp 751-757
Table 1. Patient Characteristics Fig 1. Study design.
zole 1 mg orally (PO) or 2.5 mg letrozole PO once daily in a
double-blind cross-over study (Fig 1). Each regimen was administered
for a period of 6 weeks. Six patients were randomly allocated to start
Abbreviations: BMI, body mass index; ER, estrogen receptor (either as
treatment with anastrozole followed by letrozole, whereas the other six
fmol/mg or staining by immunohistochemistry); Pos, positive; PGR, progester-
received letrozole upfront. The protocol was approved by the local
one receptor; Unk, unknown; N, lymph nodes; L, lung; B, bone; S, skin; T,
ethical committee, and every patient gave her written informed consent.
tamoxifen; D, droloxifene; A, aminoglutethimide; E, exemestane; M, megace.
After completion of the study protocol period, treatment was continuedwith either anastrozole or letrozole until disease progression.
Although different studies have revealed anastrozole10 as
well as letrozole11 to be highly potent aromatase inhibitors,
in vitro potency may not be directly correlated to in vivo
In vivo aromatization was determined before therapy and at the end
efficacy because the latter will depend on drug disposition.
of each treatment period. On each occasion, the patient received a bolus
However, studies in nude mice model systems have sug-
injection of [3H]androstenedione (500 Ci) and [14C]estrone (5 Ci)dissolved in 50 mL of saline containing 8% ethanol (w/w) as described
gested a more potent antitumor efficacy of letrozole com-
elsewhere.16 All injections were administered between 08:00 and 09:00
pared with anastrozole.12 In addition, previous studies
AM after an overnight fast and before the daily intake of anastrozole
conducted by our groups8,13 revealed both drugs to inhibit in
vivo aromatization by 97% to 99% and suggested a some-
Blood Samples and Estrogen Measurements
what better efficacy of letrozole 2.5 mg compared withanastrozole 1 mg daily (the drug doses recommended for
Blood samples for hormone measurements were obtained into
clinical use). Because of interindividual variation in drug
heparinized vials (two vials containing 10 mL each) immediatelybefore each tracer injection after an overnight fast. Plasma was
response, firm conclusions could not be drawn from such an
separated by centrifugation and stored at Ϫ20°C until analyzed.
indirect comparison. The aim of the present study was to
Estradiol (E ) and estrone (E ) were determined by radioimmunoassay,
compare the biochemical efficacy of anastrozole and letro-
as reported elsewhere.17,18 Plasma levels of estrone sulfate (E S) were
zole in breast cancer patients by evaluating their influence
determined by a novel highly sensitive assay involving purification and
on total-body aromatization and plasma estrogen levels in
and radioimmunoassay analysis using E -6-
carboxy-methyloximine-[2-125I]iodohistamine as tracer ligand.19 The
the same patients using a randomized cross-over design.
sensitivity limits for plasma levels of E , E , and E S were 2.1, 6.3, and
Urine Collection for the Measurement of Total-Body
Twelve postmenopausal women (median age, 72 years; range, 54 to
79 years) with estrogen receptor–positive, metastatic breast cancer
Urine was collected for a period of 96 hours after each tracer
suitable for treatment with an aromatase inhibitor were enrolled (Table
injection, pooled, and kept frozen (Ϫ20°C) until analyzed. The estro-
1). Postmenopausal status was defined as amenorrhoea for the duration
gen fraction was isolated and purified through multiple chromato-
of 1 year or more, with luteinizing hormone and follicle-stimulating
graphic steps involving high-performance liquid chromatography, and
hormone levels in the postmenopausal range. Previous anticancer
the percentage aromatization was calculated from the 3H/14C isotope
treatment was terminated at least 4 weeks before commencing treat-
ratio in the intravenous vehicle and urine estrogen fractions, as
ment, and no other anticancer treatment was allowed during the study
described elsewhere.8,16 On formal assessment, this method was shown
period. Patients treated with any other drugs known to influence plasma
to allow detection of up to 99.1% inhibition of aromatization.8 The
estrogen levels (like antiepileptics)14,15 were ineligible.
96-hour urine collection was completed before any change of therapy.
All patients were treated at the Department of Oncology, Haukeland
Previous work by our group has shown plasma estrogen levels in
University Hospital, Bergen, Norway. Each patient received anastro-
postmenopausal women to be well fitted to a log-normal distribution.18
17.2 pmol/L (95% CI, 9.2 to 32.1 pmol/L), and 422.8pmol/L (95% CI, 182.4 to 980.4 pmol/L), respectively. Treatment with anastrozole suppressed plasma levels of E ,
E , and E S to a mean of 14.8 pmol/L (95% CI, 12.4 to 17.7
pmol/L), 2.6 pmol/L (95% CI, 1.9 to 3.5 pmol/L), and 27.6pmol/L (95% CI, 14.0 to 54.3 pmol/L), respectively, corre-sponding to a mean suppression among individuals of81.0%, 84.9%, and 93.5%, respectively. Letrozole treatmentsuppressed plasma levels of E , E , and E S to a mean of
12.3 pmol/L (95% CI, 11.2 to 13.5 pmol/L), 2.1 pmol/L(95% CI, 2.1 to 2.1 pmol/L), and 8.9 pmol/L (95% CI, 4.9
Fig 2. Percentage of pretreatment levels of E1, E2, and E1S, and aromatase (A: during treatment with anastrozole; L: during treatment with
to 16.0 pmol/L), respectively, corresponding to a mean
letrozole; geometric mean values with 95% CI of the mean). The P values
suppression of 84.3%, 87.8%, and 98.0%, respectively (Fig
refer to the differences between the two treatment regimens.
2). Notably, nine and 12 patients had their plasma levels ofE suppressed below the sensitivity limit of the assay during
Thus, all plasma estrogen levels and the percentage of aromatization
obtained before therapy and during treatment with anastrozole or
treatment with anastrozole and letrozole, respectively, mak-
letrozole are given as their geometric mean values with 95% confidence
ing any comparison between on-treatment values of E2
intervals (CI) of the mean. Whenever estrogen levels below the
impossible. None of the patients had plasma E levels below
sensitivity limits of the assays were found, the corresponding sensitiv-
the sensitivity limit, whereas three patients had plasma E S
ity limit was used for statistical analysis. Considering measurement of
in vivo aromatization, a previous study revealed an inhibition of
suppressed below the sensitivity limit during treatment with
99.1%8 as the limit of detection, and this value was used for statistical
letrozole. The suppression of plasma E and E S levels was
comparisons whenever a value above this threshold was recorded. The
significantly greater during treatment with letrozole com-
Friedman test was used to compare three data groups, whereas data
pared with treatment with anastrozole (P ϭ .019 and P ϭ
obtained during treatment with anastrozole or letrozole were compared
.0037, respectively), with lower levels of plasma E and E S
using the Wilcoxon matched-pair signed rank test. In addition, we
performed a two-way analysis of variance to test for interaction
in nine and 11 patients during treatment with letrozole
between effects of sequence of administration on estrogen levels and
compared with anastrozole, respectively.
degree of aromatization. The mean percentage change was calculated
Pretreatment aromatization levels ranged from 1.68% to
as 100 Ϫ x, where x is the geometric mean value of the individual
4.27%. Although on-treatment levels of aromatase were
parameters in the on-treatment situation expressed as percentage ofpretreatment values.13
detectable in 11 of 12 patients during treatment withanastrozole, we found whole-body aromatization to be
suppressed below the detection limit (Ͼ 99.1% suppression)
The geometric mean pretreatment plasma levels of E , E ,
of the method in all 12 patients during treatment with
and E S were 78.1 pmol/L (95% CI, 56.1 to 108.7 pmol/L),
letrozole (Table 2 and Fig 3). Thus, inhibition of aromati-
Table 2. Influence of Letrozole and Anastrozole on Total-Body Aromatization
have previously been shown to be highly potent aromataseinhibitors causing profound suppression of plasma estrogenlevels in postmenopausal women.8,13
Indirect evidence suggests a dose-response relationship
between the degree of estrogen suppression and clinicaleffects in breast cancer. Drugs acting on adrenal steroidsynthesis as well as glucocorticoids have been reported tocause modest suppression of plasma estrogen levels and lowresponse rates in breast cancer patients.20 Several pilotstudies have confirmed the benefits of stepwise estrogensuppression in patients progressing after treatment withcastration, adrenalectomy, or an aromatase inhibitor.21-24Although the mechanism of action of progestins in highdoses in breast cancer is not fully understood, megestrolacetate given as 160 mg daily causes plasma estrogensuppression comparable with what has been recorded withthe first generation aromatase inhibitor aminoglutethim-ide.6,25,26 The degree of plasma estrogen suppressionachieved with aminoglutethimide as well as megestrolacetate is of a smaller magnitude compared with the degreeof suppression achieved with novel drugs like anastrozole,letrozole, and exemestane, which are all found to besuperior with respect to clinical effects.3,5,6,27 In particular,the large randomized trial demonstrating greater efficacy of2.5 mg letrozole in comparison with 500 mg aminoglute-thimide3 suggests a dose relationship within the limits ofaromatase inhibition achieved with these two drugs, ie,more than 99% and approximately 85%, respectively.
With several novel aromatase inhibitors at hand, an
important question is whether one drug may be superior to
Fig 3. Influence of the treatment with (A) anastrozole followed by
the others with respect to biochemical and clinical efficacy. letrozole (n ؍ 6) and (B) letrozole followed by anastrozole on the percentage
Although several studies have revealed lack of complete
of aromatization (n ؍ 6). Geometric mean values with 95% CI of the mean.
cross-resistance between different nonsteroidal aromataseinhibitors and steroidal so-called aromatase inactiva-
zation was demonstrably greater in 11 of 12 patients treated
tors,24,28-31 there may be several explanations to this obser-
with letrozole. The geometric mean suppression of aroma-
vation.32 Comparison of the biochemical and clinical effi-
tization was 97.3% during treatment with anastrozole and
cacy between different drugs of the same class, like
more than 99.1% during letrozole treatment (Wilcoxon P ϭ
anastrozole and letrozole, is interesting for several reasons.
First, any difference in clinical efficacy would select the
A two-way analysis of variance, taking account of the
appropriate drug for patient treatment. Second, any corre-
cross-over design of the study, confirmed a significant
lation (or lack of such) between the degree of estrogen
difference in the degree of aromatase inhibition (P Ͻ .001)
suppression and clinical outcome with the different drugs
as well as plasma levels of E (P ϭ .05) and E S (P ϭ .012)
would provide us with information about whether the
between treatment with letrozole and anastrozole but no
degree of estrogen deprivation is of clinical importance or
interaction between sequence of treatment and the two drug
there may be thresholds for estrogen levels with respect to
regimens for any of these parameters (P Ͼ .15 for each; Figs
clinical response. Data regarding a potential dose-response
effect with anastrozole33 or letrozole3,5 are conflicting. Interestingly, data from our previous investigations sug-
gested that letrozole, at its lower dose (0.5 mg once daily),
Anastrozole and letrozole are two third-generation aro-
achieved a greater aromatase inhibition compared with
matase inhibitors belonging to the triazole class. Both drugs
anastrozole at its higher dose (10 mg once daily).8,13 A
Fig 4. A. Influence of the cross-over (A) from anastrozole to letrozole (n ؍ 6) and (B) from letrozole to anastrozole on plasma E1S levels (n ؍ 6). Influence of the cross-over (C) from anastrozole to letrozole (n ؍ 6) and (D) from letrozole to anastrozole on plasma E1 levels (n ؍ 6). Geometric mean values with 95% CI of the mean.
study comparing the clinical efficacy of letrozole (2.5 mg
potential difference in the effect on plasma E could not be
daily) to anastrozole (1 mg daily) administered as second-
evaluated for technical reasons because of the fact that all
line endocrine therapy for metastatic breast cancer is ongo-
patients obtained plasma levels below the sensitivity limit of
ing. The results of that trial will be instrumental in assessing
the assay during treatment with letrozole and nine patients
whether suppression of aromatase to below 3% residual
had values below the limit on treatment with anastrozole.
activity is clinically important in that context.
Similar to other studies on aromatase inhibitors,13,34 we
This study revealed a significant difference in the bio-
found a better suppression of plasma E S compared with the
chemical efficacy of letrozole and anastrozole with regard to
other estrogen fractions and that this effect on E S more
in vivo aromatase inhibition as well as plasma estrogen
closely reflected differences in aromatase inhibition. It
suppression in postmenopausal breast cancer patients. The
should also be noted that the degree of plasma E S suppres-
results on inhibition of aromatase are closely similar to
sion has been found to correspond more closely to the
those which we have reported previously from separate
percentage in vivo aromatization than suppression of E and
studies of these inhibitors.8,13 A significant difference in
E also in other studies using the same methods as here.13
suppression of plasma E and E S in addition to a more
This is probably a result of technical difficulties measuring
effective inhibition of aromatization was recorded during
plasma E and E levels in the low range obtained during
therapy with letrozole compared with anastrozole. Any
therapy with these drugs, indicating the importance of
simultaneous measurements of several estrogen fractions in
inhibitor (aminoglutethimide) both reported an increase in
the same sample. The ratio between mean plasma hormone
plasma androgens37,38 and an increase in plasma estrone at
levels in untreated postmenopausal patients and the sensi-
time of progression.37 These results are consistent with a
tivity limit of the assay is about 1:10 for E and E but
nonspecific stress reaction causing elevated adrenal hor-
below 1:100 for E S. Use of alterations in plasma E S levels
mone secretion and do not suggest any escape from the
as a surrogate marker for alterations in plasma estrogens in
aromatase inhibitory effect. In a recently published study,
general is further supported by knowledge that plasma
patients progressing on different nonsteroidal aromatase
levels of E , E , and E S are at equilibrium provided no
inhibitors were treated with exemestane. Interestingly, pa-
interaction with interconverting enzymes occurs.35 Overall,
tients failing on novel nonsteroidal aromatase inhibitors
plasma E S seems to be the most reliable indicator of
were found to have consistently suppressed plasma estrogen
estrogen suppression in patients treated with potent aro-
levels.31 Thus, although our short-term data may not be
directly extrapolated to long-term treatment, currently there
The cross-over design of the present study was chosen to
is little evidence suggesting alterations in drug pharmacol-
avoid interindividual variation concerning aromatase inhi-
bition and plasma estrogen suppression in our comparison.
In conclusion, this study is the first head-to-head com-
The mean half-life of both letrozole and anastrozole is
parison evaluating potential endocrine differences between
approximately 40 to 50 hours. Thus, in theory, more than
third-generation aromatase inhibitors in vivo. We found
99.99% of the drugs will be eliminated over a time period of
letrozole to cause a significantly better inhibition of in vivo
4 weeks after the final dose. We used a time period of 6
aromatization and a better plasma estrogen suppression
weeks on each regimen to avoid any possible hang-over
compared with anastrozole. Together with clinical data
effects. A wash-out period without any treatment could have
from ongoing trials, we believe the results from this study
detrimental effects on the therapeutic outcome in this groupof patients with metastatic breast cancer. The finding of a
may provide important information not only to select
greater aromatase inhibition and estrogen suppression of
between two drugs for clinical use but to also understand the
letrozole when given either first- or second-line together
important relationship between degree of estrogen suppres-
with a negative test for interaction demonstrates that any
sion and clinical efficacy of estrogen suppressors in breast
hang-over effects are unlikely in this study. Notably, the
design of this study required a short-term course with eachdrug for valid comparison. Although we may not exclude
the possibility of alterations in drug disposition over time
We thank H. Berntsen and D. Ekse at the Department of Oncology,
during treatment with these compounds, the two studies
Haukeland University Hospital, Bergen, Norway, for their technical
addressing long-term endocrine effects of an aromatase
1. Lønning PE: Pharmacology of new aromatase inhibitors. Breast
6. Kaufmann M, Bajetta E, Dirix LY, et al: Exemestane is superior
to megestrol acetate after tamoxifen failure in postmenopausal women
2. Hamilton A, Piccart M: The third-generation non-steroidal aro-
with advanced breast cancer: Results of a phase III randomized
matase inhibitors: A review of their clinical benefits in the second-line
double-blind trial. J Clin Oncol 18:1399-1411, 2000
hormonal treatment of advanced breast cancer. Ann Oncol 10:377-384,
7. Masamura S, Santner SJ, Heitjan DF, et al: Estrogen deprivation
causes estradiol hypersensitivity in human breast cancer cells. J Clin
3. Gershanovich M, Chaudri HA, Campos D, et al: Letrozole, a new
oral aromatase inhibitor: Randomised trial comparing 2.5 mg daily, 0.5
8. Dowsett M, Jones A, Johnston SRD, et al: In vivo measurement
mg daily and aminoglutethimide in postmenopausal women with
of aromatase inhibition by letrozole (CGS 20267) in postmenopausal
advanced breast cancer. Ann Oncol 9:639-645, 1998
patients with breast cancer. Clin Cancer Res 1:1511-1515, 1995
4. Buzdar A, Jonat W, Howell A, et al: Anastrozole, a potent and
9. MacNeill FA, Jones AL, Jacobs S, et al: The influence of
selective aromatase inhibitor, versus megestrol acetate in postmeno-
aminoglutethimide and its analogue rogletimide on peripheral aroma-
pausal women with advanced breast cancer: Results of overview
tisation in breast cancer. Br J Cancer 66:692-697, 1992
analysis of two phase III trials. J Clin Oncol 14:2000-2011, 1996
10. Dukes M, Edwards PN, Large M, et al: The preclinical phar-
5. Dombernowsky P, Smith I, Falkson G, et al: Letrozole, a new
macology of Arimidex (anastrozole; ZD1033): A potent, selective
oral aromatase inhibitor for advanced breast cancer: Double-blind
aromatase inhibitor. J Steroid Biochem Mol Biol 58:439-445, 1996
randomized trial showing a dose effect and improved efficacy and
11. Bhatnagar AS, Hausler A, Schieweck K: Inhibition of aromatase
tolerability compared to megestrol acetate. J Clin Oncol 16:453-
in vitro and in vivo by aromatase inhibitors. J Enzyme Inhib 4:179-186,
12. Brodie A, Lu Q, Liu Y, et al: Aromatase inhibitors and their
sulphate in postmenopausal breast cancer patients. J Steroid Biochem
antitumor effects in model systems. Endocr Rel Cancer 6:205-210,
27. Buzdar AU, Jonat W, Howell A, et al: Anastrozole versus
13. Geisler J, King N, Dowsett M, et al: Influence of anastrozole
megestrol acetate in the treatment of postmenopausal women with
(Arimidex), a selective, non-steroidal aromatase inhibitor, on in vivo
advanced breast carcinoma: Results of a survival update based on a
aromatisation and plasma oestrogen levels in postmenopausal women
combined analysis of data from two mature phase III trials. Cancer
with breast cancer. Br J Cancer 74:1286-1291, 1996
14. Geisler J, Engelsen B, Berntsen H, et al: Differential influence of
28. Murray R, Pitt P: Aromatase inhibition with 4-OH-androstenedi-
carbamazepine and valproate monotherapy on plasma levels of oes-
one after prior aromatase inhibition with aminoglutethimide in women
trone sulphate and dehydroepiandrosterone sulphate in male epileptic
with advanced breast cancer. Breast Cancer Res Treat 35:249-253,
15. Lønning PE, Bakke P, Thorsen T, et al: Plasma levels of
29. Harper-Wynne C, Coombes RC: Anastrozole shows evidence of
estradiol, estrone, estrone sulfate and sex hormone binding globulin in
activity in postmenopausal patients who have responded or stabilised
patients receiving rifampicin. J Steroid Biochem 33:631-635, 1989
on formestane therapy. Eur J Cancer 35:744-746, 1999
16. Jacobs S, Lønning PE, Haynes B, et al: Measurement of
30. Thu¨rlimann B, Paridaens R, Serin D, et al: Third-line hormonal
aromatisation by a urine technique suitable for the evaluation of
treatment with exemestane in postmenopausal patients with advanced
aromatase inhibitors in vivo. J Enzyme Inhib 4:315-325, 1991
breast cancer progressing on aminoglutethimide: A phase II multicentre
17. Dowsett M, Goss PE, Powles TJ, et al: Use of the aromatase
multinational trial. Eur J Cancer 33:1767-1773, 1997
inhibitor 4-hydroxyandrostenedione in postmenopausal breast cancer:
31. Lønning PE, Bajetta E, Murray R, et al: Activity of exemestane
Optimization of therapeutic dose and route. Cancer Res 47:1957-1961,
(Aromasin) in metastatic breast cancer after failure of nonsteroidal
aromatase inhibitors: A phase II trial. J Clin Oncol 18:2234-2244, 2000
18. Lønning PE, Helle SI, Johannessen DC, et al: Relations between
32. Lønning PE: Cross-resistance to different aromatase inhibitors
sex hormones, sex hormone binding globulin, insulin-like growth
in breast cancer treatment. Endocrine Rel Cancer 6:251-257, 1999
factor-I and insulin-like growth factor binding protein-1 in post-
33. Buzdar AU, Jonat W, Howell A, et al: Anastrozole versus
menopausal breast cancer patients. Clin Endocrinol 42:23-30, 1995
megestrol acetate in the treatment of postmenopausal women with
19. Lønning PE, Ekse D: A sensitive assay for measurement of
advanced breast carcinoma: Results of a survival update based on a
plasma estrone sulphate in patients on treatment with aromatase
combined analysis of data from two mature phase III trials. Cancer
inhibitors. J Steroid Biochem Mol Biol 55:409-412, 1995
20. Lønning PE: New endocrine drugs for treatment of advanced
34. Geisler J, King N, Anker G, et al: In vivo inhibition of
breast cancer. Acta Oncol 29:379-386, 1990
aromatization by exemestane, a novel irreversible aromatase inhibitor,
21. Dowsett M, Stein RC, Coombes RC: Aromatization inhibition
in postmenopausal breast cancer patients. Clin Cancer Res 4:2089-
alone or in combination with GnRH agonists for the treatment of
premenopausal breast cancer patients. J Steroid Biochem Mol Biol43:155-159, 1992
35. Lønning PE, Dowsett M, Powles TJ: Postmenopausal estrogen
22. Samojlik E, Santen RJ, Worgul TJ: Suppression of residual
synthesis and metabolism: Alterations caused by aromatase inhibitors
estrogen production with aminoglutethimide in women following
used for the treatment of breast cancer. J Steroid Biochem 35:355-366,
surgical hypophysectomy or adrenalectomy. Clin Endocrinol 20:43-51,
36. Lønning PE, Geisler J, Johannessen DC, et al: Plasma estrogen
23. Lønning PE, Dowsett M, Jones A, et al: Influence of aminoglu-
suppression with aromatase inhibitors evaluated by a novel, sensitive
tethimide on plasma estrogen levels in breast cancer patients on
assay for estrone sulphate. J Steroid Biochem Mol Biol 61:255-260,
4-hydroxyandrostenedione treatment. Breast Cancer Res Treat 23:57-
37. Dowsett M, Harris AL, Smith IE, et al: Endocrine changes
24. Geisler J, Johannessen DC, Anker G, et al: Treatment with
associated with relapse in advanced breast cancer patients on amin-
formestane alone and in combination with aminoglutethimide in
oglutethimide therapy. J Clin Endocrinol Metab 58:99-104, 1984
heavily pretreated cancer patients: Clinical and endocrine effects. Eur
38. Santen RJ: Overall experience with aminoglutethimide in the
management of advanced breast cancer, in Elsdon-Dew RW, Jackson
25. Lundgren S, Helle SI, Lønning PE: Profound suppression of
IM, Birdwood GFB (eds): International Symposium at the Royal
plasma estrogens by megestrol acetate in postmenopausal breast cancer
College of Obstreticians and Gynaecologists: Aminoglutethimide—An
patients. Clin Cancer Res 2:1515-1521, 1996
Alternative Endocrine Therapy for Breast Cancer. Regents Park,
26. Geisler J, Lien EA, Ekse D, et al: Influence of aminoglutethim-
London, United Kingdom, The Royal Society of Medicine, Academic
ide on plasma levels of estrone sulphate and dehydroepiandrosterone
Press, Grune & Stratton, 1982, pp 3-7
Poster Session IV Wednesday, June 20 Presenter’s name is in bold and is subject to change. electric field. In particular, cell displacement rate was higher for cells culturedonto hydrogel substrate and myotubes contraction rate increased as a conse- THE ROLE OF EPHB/EPHRIN-B INTERACTIONS IN CELL quence of the frequency increasing. This frequency-dependent response of ATTACHMENT AND
Eular On-line Course on Rheumatic Diseases – module °42a Clodoveo Ferri, Marco Sebastiani, Patrice Cacoub, David Saadoun CRYOGLOBULINEMIA AND SYSTEMIC MANIFESTATIONS OF HEPATITIS C VIRUS IN-DEPTH-DISCUSSION II Antiviral therapy in Mixed Cryoglobulinemia Vasculitis With the discovery of HCV as the etiologic agent for most cases of mixed cryoglobulinemia new opportunities
 Table 1. Patient Characteristics
Table 1. Patient Characteristics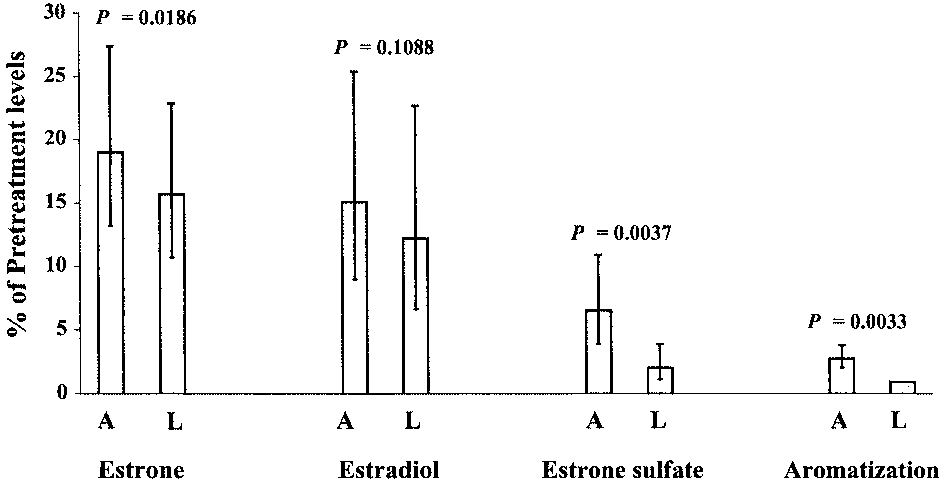 17.2 pmol/L (95% CI, 9.2 to 32.1 pmol/L), and 422.8pmol/L (95% CI, 182.4 to 980.4 pmol/L), respectively.
17.2 pmol/L (95% CI, 9.2 to 32.1 pmol/L), and 422.8pmol/L (95% CI, 182.4 to 980.4 pmol/L), respectively.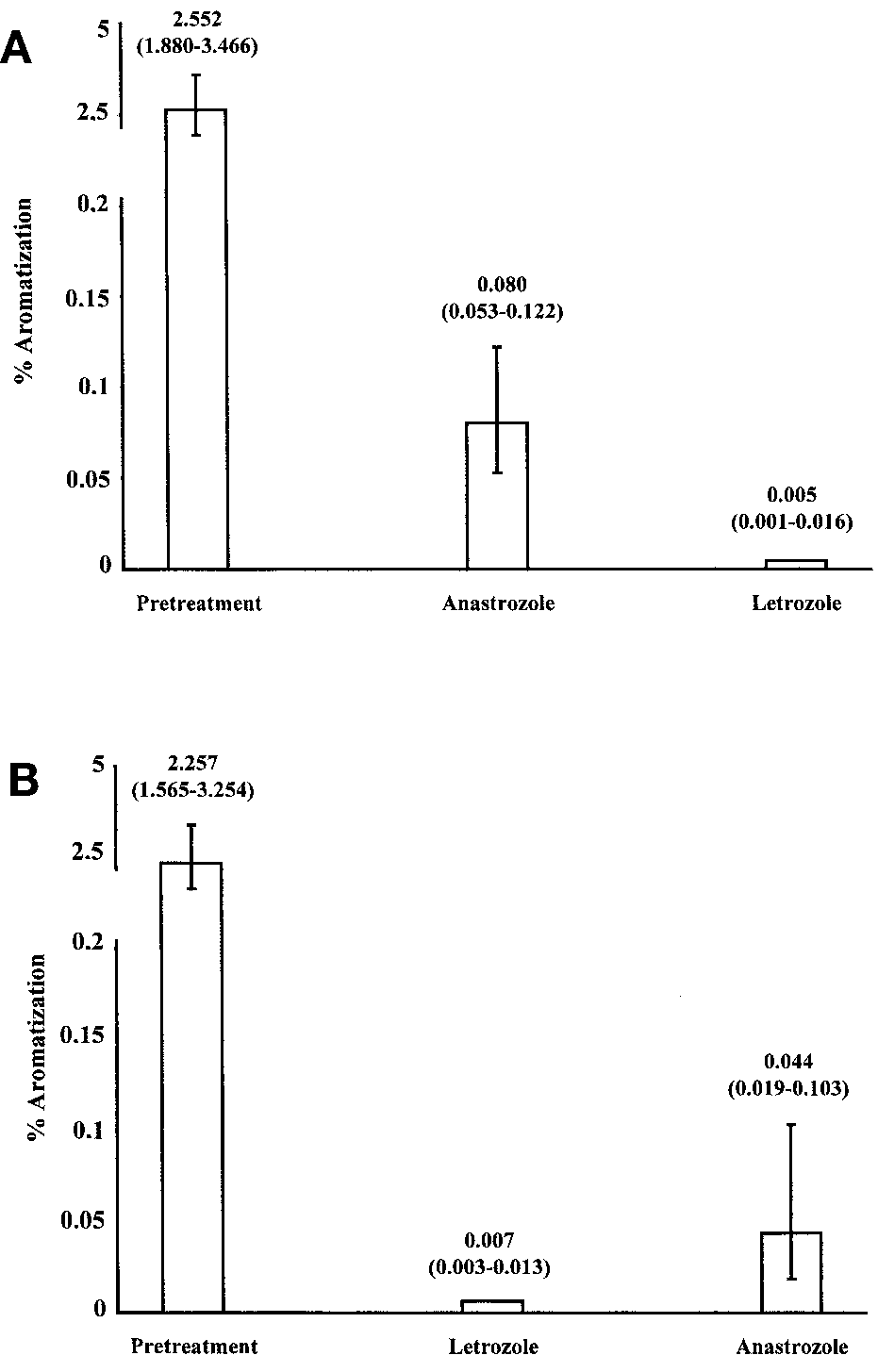 have previously been shown to be highly potent aromataseinhibitors causing profound suppression of plasma estrogenlevels in postmenopausal women.8,13
Indirect evidence suggests a dose-response relationship
between the degree of estrogen suppression and clinicaleffects in breast cancer. Drugs acting on adrenal steroidsynthesis as well as glucocorticoids have been reported tocause modest suppression of plasma estrogen levels and lowresponse rates in breast cancer patients.20 Several pilotstudies have confirmed the benefits of stepwise estrogensuppression in patients progressing after treatment withcastration, adrenalectomy, or an aromatase inhibitor.21-24Although the mechanism of action of progestins in highdoses in breast cancer is not fully understood, megestrolacetate given as 160 mg daily causes plasma estrogensuppression comparable with what has been recorded withthe first generation aromatase inhibitor aminoglutethim-ide.6,25,26 The degree of plasma estrogen suppressionachieved with aminoglutethimide as well as megestrolacetate is of a smaller magnitude compared with the degreeof suppression achieved with novel drugs like anastrozole,letrozole, and exemestane, which are all found to besuperior with respect to clinical effects.3,5,6,27 In particular,the large randomized trial demonstrating greater efficacy of2.5 mg letrozole in comparison with 500 mg aminoglute-thimide3 suggests a dose relationship within the limits ofaromatase inhibition achieved with these two drugs, ie,more than 99% and approximately 85%, respectively.
have previously been shown to be highly potent aromataseinhibitors causing profound suppression of plasma estrogenlevels in postmenopausal women.8,13
Indirect evidence suggests a dose-response relationship
between the degree of estrogen suppression and clinicaleffects in breast cancer. Drugs acting on adrenal steroidsynthesis as well as glucocorticoids have been reported tocause modest suppression of plasma estrogen levels and lowresponse rates in breast cancer patients.20 Several pilotstudies have confirmed the benefits of stepwise estrogensuppression in patients progressing after treatment withcastration, adrenalectomy, or an aromatase inhibitor.21-24Although the mechanism of action of progestins in highdoses in breast cancer is not fully understood, megestrolacetate given as 160 mg daily causes plasma estrogensuppression comparable with what has been recorded withthe first generation aromatase inhibitor aminoglutethim-ide.6,25,26 The degree of plasma estrogen suppressionachieved with aminoglutethimide as well as megestrolacetate is of a smaller magnitude compared with the degreeof suppression achieved with novel drugs like anastrozole,letrozole, and exemestane, which are all found to besuperior with respect to clinical effects.3,5,6,27 In particular,the large randomized trial demonstrating greater efficacy of2.5 mg letrozole in comparison with 500 mg aminoglute-thimide3 suggests a dose relationship within the limits ofaromatase inhibition achieved with these two drugs, ie,more than 99% and approximately 85%, respectively.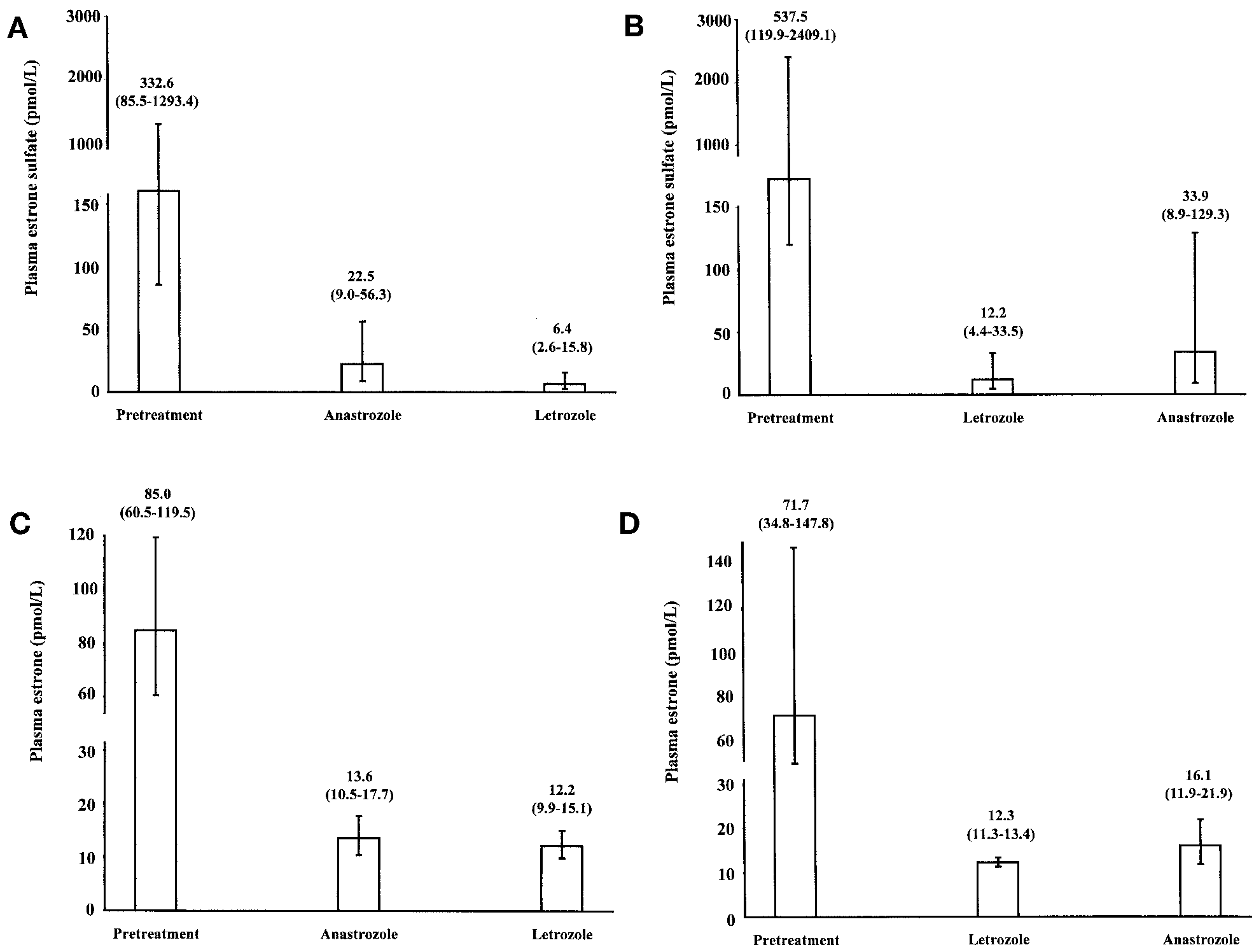 Fig 4. A. Influence of the cross-over (A) from anastrozole to letrozole (n ؍ 6) and (B) from letrozole to anastrozole on plasma E1S levels (n ؍ 6). Influence
Fig 4. A. Influence of the cross-over (A) from anastrozole to letrozole (n ؍ 6) and (B) from letrozole to anastrozole on plasma E1S levels (n ؍ 6). Influence