Levitra has a minimal amount of contraindications which has increased its popularity wellbutrin xl uk You can buy quality certified medications from us at an affordable price.
Microsoft word - sindoni_et_al_ht05_09 r2.doc
CASE REPORT COFFEE IMPAIRS INTESTINAL ABSORPTION OF LEVOTHYROXINE: REPORT OF ADDITIONAL CASES.
Alessandro Sindoni1, Roberto Vita1, Sergio Fusco1, Giovanna Saraceno1, Maria Angela
Pappalardo1, Oana-Ruxandra Cotta2, Silvana Grasso2, Francesco Trimarchi1, Salvatore Benvenga1,2,3.
1Sezione di Endocrinologia del Dipartimento Clinico Sperimentale di Medicina e Farmacologia, Università di Messina, Messina, Italy; 2Master on Children, Adolescent and Women’s Endocrine Health, University of Messina, Messina, Italy; 3Programma Infradipartimentale di Endocrinologia Molecolare e Clinica, A.O.U. Policlinico “G. Martino”, 98125 Messina, Italy. Reviewing Editor: Leonidas Duntas
The Authors declare no conflict of interest related to this work. Correspondence: Salvatore Benvenga Dipartimento Clinico Sperimentale di Medicina e Farmacologia Università di Messina A.O.U. Policlinico “G. Martino” 98125 Messina-Italy E-mail: [email protected] ABSTRACT
Several drugs inhibit the intestinal absorption of levothyroxine (L-T4) when taken simultaneously
with the thyroid hormone or shortly later. Recently, in a study on 8 women, coffee has been
reported to reduce the intestinal absorption of L-T4, so that L-T4 was added to the list of the
medications whose intestinal absorption is decreased by coffee. We report another six adult
patients, 5 women and 1 man, aged 38 to 62 years, who were observed during the last 18 months.
All patients were referred because of failure of serum TSH to be normalized or suppressed by
appropriate replacement (1.6-1.8 μg/Kg b.w.) or TSH-suppressive (2.0-2.2 μg/Kg b.w.) therapy with
L-T4. In each of the six patients, serum TSH failed to be normalized or suppressed if L-T4 was
swallowed simultaneously with coffee (or followed by coffee soon after). Correction of this habit, by
drinking coffee 60 minutes after having swallowed L-T4 with water, resulted in normalization or
Key-words: Thyroxine; Thyrotropin; TSH; Coffee; Intestinal absorption. Background.
L-T4 is widely used across the world; indeed, in 2007 it was one of the top 5 medications in the
United States by units sold (1). In adults, the mean daily dose of L-T4 is 1.6 µg/kg body weight for
replacement and 2.2 µg/kg b.w. for TSH suppression (2). As well known, L-T4 therapy is monitored
Recently, we have reported on the impaired intestinal absorption of L-T4 caused by drinking
coffee within 10 minutes of swallowing the L-T4 tablet (3). These cases (8 women) were collected
during a decade of clinical practise. Here we report six additional cases (5 women and 1 man),
who were observed during the last 18 months, which suggests the degree of underestimation of
the problem. None of the six patients was taking other known interferes of the intestinal absorption
Case reports.
Patient no. 1 had a 3-year history of multinodular goiter and had been treated with L-T4 at a
daily dose of 132 μg (1.8 μg/Kg b.w.). However her TSH was never below 0.80 mU/L. Careful
history taking disclosed that she used to ingest the L-T4 tablet with water, but followed by one full
cup of coffee within the next 5-10 minutes. We suggested her to drink coffee at least 60 minutes
after swallowing the L-T4 tablet. She returned to us six months later with a serum TSH of 0.20
mU/L, and after another six months with a serum TSH of 0.04 mU/L (Table 1).
Patient no. 2 had also been seen by other endocrinologists for multinodular goiter and was given
L-T4 at a dose of 2.0-2.2 μg/Kg b.w./day. However, within the next 3 years serum TSH was never
suppressed (1.1 to 1.7 mU/L). We found that she used to swallow the L-T4 tablet with a full tea-cup
of barley coffee. She was instructed to postpone drinking barley coffee. Three months later, during
which she took the L-T4 tablet with water 30 to 60 minutes prior to her barley coffee, serum TSH
dropped to 0.62 mU/L: however, within the next 12 months, serum TSH dropped to from 0.19 to
0.02 mU/L, when the lag-time was prolonged to 60-90 minutes (Table 1).
Patient no. 3 had the nodular goiter variant of Hashimoto’s thyroiditis, for which she underwent
partial thyroidectomy 12 years prior to our observation. After thyroidectomy, she started taking L-
T4 at a daily dose of 1.6 μg/Kg b.w., that over the years was increased up to 2.0 μg/Kg b.w.,
because serum TSH remained high. Even though serum TSH decreased (from 8.1 to 4.7 mU/L), it
was still above normal. We found that she ingested L-T4 with one full cup of coffee. We instructed
her to postpone drinking coffee by 60 minutes, and left her under the last regimen of L-T4 (1.8
μg/Kg b.w./day). Three and seven months later serum TSH was, respectively, 2.2 and 1.9 mU/L.
She admitted, and her husband confirmed, that her compliance was partial (30 in lieu of 60
Patient no. 4 was a nurse. She had undergone right lobectomy 16 years earlier and was put on
a daily regimen of 1.7 μg/Kg b.w. of L-T4. In the last two years serum TSH had fluctuated between
0.94 and 2.0 mU/L. We found that two years prior to our observation, the patient bought an
espresso machine, and most of the time she used to ingest the L-T4 tablet with one or two cups of
espresso. We instructed her to postpone drinking espresso and, over the next six months,
postponing espresso by 60 minutes, TSH fluctuated between 0.06 and 0.37 mU/L (Table 1).
Patient no. 5 had been seen by other endocrinologists for a nodular goiter and was given L-T4 at
a daily dose of 1.6 μg/Kg b.w., but TSH was not suppressed (0.95 mU/L). We increased the dose
to 2.1 μg/Kg b.w. and instructed her to postpone drinking coffee by 60 minutes. Over the next year,
TSH decreased scantly (0.76 mU/L) when she persisted in her habit, but decreased substantially
(0.43 mU/L) when she postponed drinking coffee by 60 minutes (Table 1).
Patient no. 6 was a man, who five years earlier was thyroidectomized for a multinodular goiter.
After thyroidectomy, he started L-T4 treatment (2.1 μg/Kg b.w./day). The patient took the L-T4
tablet with water, but drunk a cup of coffee within the next 10 minutes. Serum TSH was 2.7 mU/L.
We asked the patient to postpone the cup of coffee by one hour. Three months later, TSH dropped
Table 1. Serum TSH levels in 6 patients under L-T4 replacement or TSH-suppressive therapy based on the modality of swallowing the L-T4 tablet.
Case number Age/Gender L-T4 tablet with coffee or soon after coffee L-T4 with water and drinking coffee postponed**
* Normal values of serum TSH (in mU/L) were, respectively, 0.4 – 4.0 (cases #1 and #6), 0.47 – 4.6 (case #2), 0.27 – 4.2
(cases #3 and #4) and 0.4 – 5.0 mU/L (case #5).
** Details on the lag-time (in minutes) are in the text.
Discussion.
In some circumstances, patients require greater daily doses of L-T4 to attain the desired fall in
serum TSH concentrations. Interference can be related to a) patient characteristics, dietary habits
and compliance with the drug; b) the pharmaceutical characteristics of L-T4 and c) the interference
of other medications (4). Several oral medications inhibit the intestinal absorption of L-T4 sodium
when taken simultaneously with thyroid hormone. In most of these cases, the malabsorption of L-
T4 is due to the binding of the hormone to medications, forming an insoluble or non-absorbable
complex: these include cholestyramine (5), ferrous sulphate (6), aluminium hydroxide (7), calcium
carbonate (8), sucralfate (9). Besides, L-T4 should be taken separately from food, since food
adsorbs thyroid hormone, decreasing its availability for intestinal absorption (10-12): in particular,
dietary fibres and herbal remedies reduce intestinal absorption of L-T4 (13,14).
Drugs are absorbed after oral administration as a consequence of interactions between the
drug, its formulation and the gastrointestinal tract. Based on the in vitro studies described in ref. 3,
at least one mechanism for the interference of coffee is physical sequestration of L-T4; however,
we cannot exclude other possibilities. These possibilities should not include changes in gastric
empting, intestinal transit or pH, because these parameters have been reported to be unaffected
by coffee (15,16). Coffee has been reported to impair the intestinal absorption of a number of
medications and other substances (17-24) (Table 2), and very recently we added L-T4 to the list
based on the said 8 cases observed and in vitro studies suggesting a sequestering effect (3).
Table 2. Impaired absorption of the most common drugs or substances caused by coffee*. DRUG/SUBSTANCE Anticancer drugs Camptothecin, Topotecan Bisbosphonates Antipsycothics
Amitriptyline, Imipramine, Phenothiazines
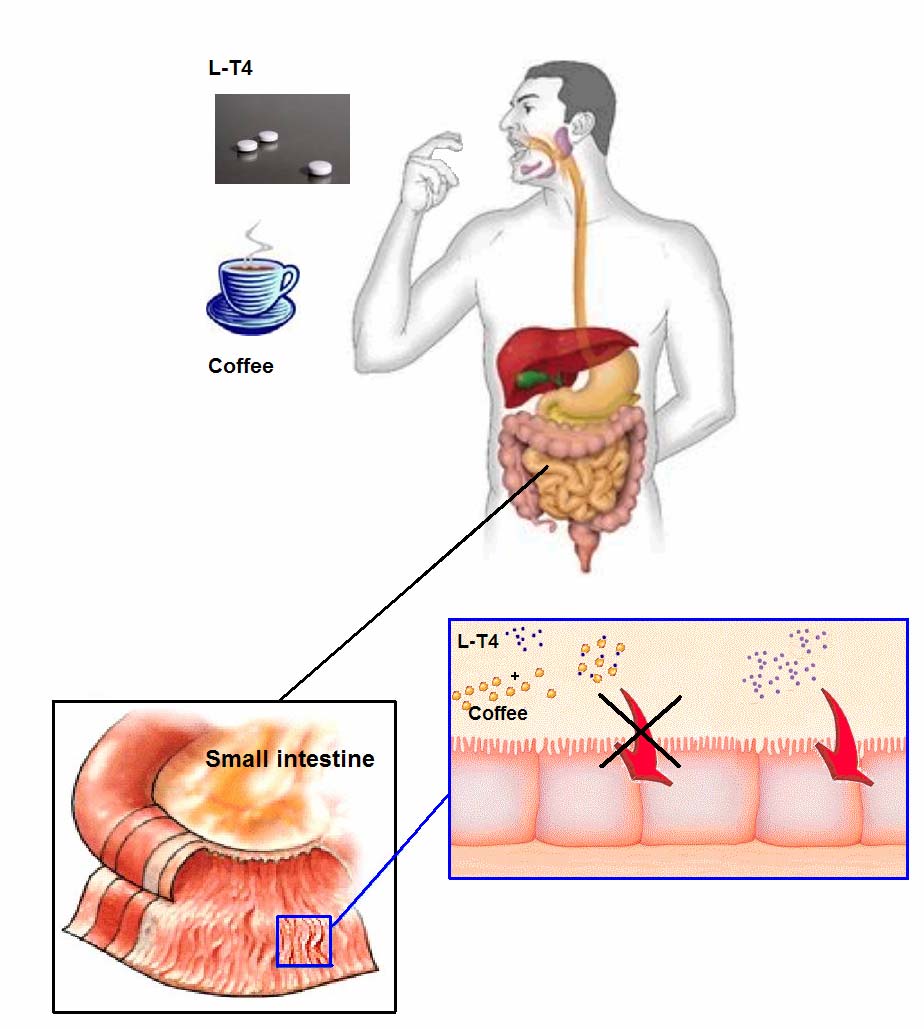
Thus, regardless of type, coffee should act in vivo by sequestering L-T4 and reducing hormone
availability for uptake by the intestinal epithelium (Fig. 1).
Fig. 1 Sequestering activity of coffee reduces intestinal absorption of L-T4. Conclusion.
Here, we have reported that patients with impaired L-T4 absorption due to coffee are also men,
and we have also reported the first patient in whom the interferer is barley coffee.
In conclusion, considering the wide consumption of coffee and the frequent prescription of L-T4
for either replacement or TSH-suppressive purposes, patients with inappropriately high or non-
suppressed serum TSH should be questioned routinely about the possible impairment of L-T4
absorption caused by coffee drinking. Accordingly, patients should be instructed to take coffee at
least one hour following the intake of L-T4 tablets. Furthermore, it would be desirable that the
leaflet contained in pharmaceutical packaging be sufficiently informative about the reduced
References.
1. Drug Topics – Pharmacy and clinical news for Pharmacists. Top 200 generic drugs by units
in 2007. Available at http://drugtopics.modernmedicine.com/ (accessed January 2009).
2. Mandel SJ, Brent GA, Larsen PR. Levothyroxine therapy in patients with thyroid disease.
3. Benvenga S, Bartolone L, Pappalardo MA, Russo A, Lapa D, Giorgianni G, Saraceno G,
Trimarchi F. Altered intestinal absorption of L-thyroxine caused by coffee. Thyroid 18: 293-
4. Centanni M, Santaguida M, Gargano L. Malabsorption of T4:new insights on oral thyroxine
5. Northcutt RC, Stiel JN, Hollifield JW, Stant EG Jr. The influence of cholestyramine on
thyroxine absorption. JAMA 208: 1857-1861, 1969.
6. Campbell NRC, Hasinoff BB, Stalts H, Rao B, Wong NCW. Ferrous sulfate reduces
thyroxine efficacy in patients with hypothyroidism. Ann Intern Med 117:1010-1013, 1992.
7. Liel Y, Sperber AD, Shany S. Nonspecific intestinal adsorption of levothyroxine by
aluminum hydroxide. Am J Med 97: 363-365, 1992.
8. Singh N, Singh PN, Hershman JM. Effect of calcium carbonate on the absorption of
levothyroxine. JAMA 283: 2822-2825, 2000.
9. Havrankova J, Lahaie R. Levothyroxine binding by sucralfate. Ann Intern Med 117:445-
10. Benvenga S, Bartolone L, Squadrito S, Lo Giudice F, Trimarchi F. Delayed intestinal
absorption of levothyroxine. Thyroid 5: 249-253, 1995.
11. Hays MT. Thyroid hormone and the gut. Endocr Res 14:203-224, 1988.
12. Wenzel KW, Kirschsieper HE. Aspects of the absorption of oral l-thyroxine in normal man.
13. Woeber KA. Treatment of hypothyroidism. In: Braverman LE, Utiger RD (eds) Werner and
Ingbar’s The Thyroid, 9th edition. Lippincott Williams & Wilkins, Philadelphia, 2005. pp 864-
14. Centanni M, Gargano L, Canettieri G, Viceconti N, Franchi A, Delle Fave G, Annibale A.
Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis. N Engl J Med 354:
15. Ehrlich A, Basse H, Henkel-Ernst J, Hey B, Menthe J, Lucker PW. Effect of differently
processed coffee on the gastric potential difference and intragastric pH in healthy
volunteers. Methods Find Exp Clin Pharmacol 20:155-161, 1998.
16. van Nieuwenhoven MA, Brummer RM, Brouns F. Gastrointestinal function during exercise:
comparison of water, sports drink, and sports drink with caffeine. J Appl Physiol 89:1079-
17. Traganos F, Kapuscinski J, Gong J, Ardelt B, Darzynkiewicz RJ, Darzynkiewicz Z. Caffeine
prevents apoptosis and cell cycle effects induced by camptothecin or topotecan in HL-60
18. Gertz BJ, Holland SD, Kline WF, Matuszewski BK, Freeman A, Quan H, Lasseter KC,
Mucklow JC, Porras AG. Studies of the oral bioavailability of alendronate. Clin Pharmacol
19. Drugs interactions: factors affecting response to drugs: Merck Manual home edition.
Available at: http://www.merck.com/mmhe/sec02/ch013/ch013c.html (accessed January
20. Cabrera Forneiro J, Chamorro Merino G, González Alfonso M, Ramón Jarne FJ.
Bioavailability of haloperidol in nutritive solutions: clinical implications. Arch Neurobiol
21. Lasswell WL Jr, Weber SS, Wilkins JM. In vitro interaction of neuroleptics and tricylic
antidepressants with coffee, tea, and gallotannic acid. J Pharm Sci 73:1056-1058, 1984.
22. Kiel DP, Felson DT, Hannan MT, Anderson JJ, Wilson PW. Caffeine and the risk of hip
fracture: the Framingham Study. Am J Epidemiol 132: 675-684, 1990.
23. Morck TA, Lynch SR, Cook JD. Inhibition of food iron absorption by coffee. Am J Clin Nutr
24. FMI – Mechanisms of food medications interactions. Available at:
http://www.foodmedinteractions.com/mechs.html (accessed January 2009).
Asian-Aust. J. Anim. Sci. Vol. 22, No. 5 : 756 - 764 Perinatal Nutrition of the Calf and Its Consequences for Lifelong Productivity* P. C. Wynn1, ** , H. M. Warriach1, 2, A. Morgan3, D. M. McGill1, S. Hanif1, 2, M. Sarwar4 A. Iqbal5, P. A. Sheehy3 and R. D. Bush3 1 EH Graham Centre for Agricultural Innovation (Charles Sturt University and NSW Department of Primary Industries)
HEART FOR AFRICA PACKING LIST Packing for your trip to Africa can be an intimidating task. To help you out, Heart for Africa has prepared a recommended packing list. Please use this list to help you pack for your trip. AIRPLANE: • Neck pil ow • Earplugs • Warm socks • Sleep Aids/ ALL needed Medication • Books/journal/Magazines • CD player, headphones, playing cards, etc. �

 CASE REPORT
CASE REPORT 


 Patient no. 4 was a nurse. She had undergone right lobectomy 16 years earlier and was put on
a daily regimen of 1.7 μg/Kg b.w. of L-T4. In the last two years serum TSH had fluctuated between
0.94 and 2.0 mU/L. We found that two years prior to our observation, the patient bought an
espresso machine, and most of the time she used to ingest the L-T4 tablet with one or two cups of
espresso. We instructed her to postpone drinking espresso and, over the next six months,
postponing espresso by 60 minutes, TSH fluctuated between 0.06 and 0.37 mU/L (Table 1).
Patient no. 5 had been seen by other endocrinologists for a nodular goiter and was given L-T4 at
a daily dose of 1.6 μg/Kg b.w., but TSH was not suppressed (0.95 mU/L). We increased the dose
to 2.1 μg/Kg b.w. and instructed her to postpone drinking coffee by 60 minutes. Over the next year,
TSH decreased scantly (0.76 mU/L) when she persisted in her habit, but decreased substantially
(0.43 mU/L) when she postponed drinking coffee by 60 minutes (Table 1).
Patient no. 6 was a man, who five years earlier was thyroidectomized for a multinodular goiter.
After thyroidectomy, he started L-T4 treatment (2.1 μg/Kg b.w./day). The patient took the L-T4
tablet with water, but drunk a cup of coffee within the next 10 minutes. Serum TSH was 2.7 mU/L.
We asked the patient to postpone the cup of coffee by one hour. Three months later, TSH dropped
Table 1. Serum TSH levels in 6 patients under L-T4 replacement or TSH-suppressive therapy
Patient no. 4 was a nurse. She had undergone right lobectomy 16 years earlier and was put on
a daily regimen of 1.7 μg/Kg b.w. of L-T4. In the last two years serum TSH had fluctuated between
0.94 and 2.0 mU/L. We found that two years prior to our observation, the patient bought an
espresso machine, and most of the time she used to ingest the L-T4 tablet with one or two cups of
espresso. We instructed her to postpone drinking espresso and, over the next six months,
postponing espresso by 60 minutes, TSH fluctuated between 0.06 and 0.37 mU/L (Table 1).
Patient no. 5 had been seen by other endocrinologists for a nodular goiter and was given L-T4 at
a daily dose of 1.6 μg/Kg b.w., but TSH was not suppressed (0.95 mU/L). We increased the dose
to 2.1 μg/Kg b.w. and instructed her to postpone drinking coffee by 60 minutes. Over the next year,
TSH decreased scantly (0.76 mU/L) when she persisted in her habit, but decreased substantially
(0.43 mU/L) when she postponed drinking coffee by 60 minutes (Table 1).
Patient no. 6 was a man, who five years earlier was thyroidectomized for a multinodular goiter.
After thyroidectomy, he started L-T4 treatment (2.1 μg/Kg b.w./day). The patient took the L-T4
tablet with water, but drunk a cup of coffee within the next 10 minutes. Serum TSH was 2.7 mU/L.
We asked the patient to postpone the cup of coffee by one hour. Three months later, TSH dropped
Table 1. Serum TSH levels in 6 patients under L-T4 replacement or TSH-suppressive therapy 
 and compliance with the drug; b) the pharmaceutical characteristics of L-T4 and c) the interference
of other medications (4). Several oral medications inhibit the intestinal absorption of L-T4 sodium
when taken simultaneously with thyroid hormone. In most of these cases, the malabsorption of L-
T4 is due to the binding of the hormone to medications, forming an insoluble or non-absorbable
complex: these include cholestyramine (5), ferrous sulphate (6), aluminium hydroxide (7), calcium
carbonate (8), sucralfate (9). Besides, L-T4 should be taken separately from food, since food
adsorbs thyroid hormone, decreasing its availability for intestinal absorption (10-12): in particular,
dietary fibres and herbal remedies reduce intestinal absorption of L-T4 (13,14).
Drugs are absorbed after oral administration as a consequence of interactions between the
drug, its formulation and the gastrointestinal tract. Based on the in vitro studies described in ref. 3,
at least one mechanism for the interference of coffee is physical sequestration of L-T4; however,
we cannot exclude other possibilities. These possibilities should not include changes in gastric
empting, intestinal transit or pH, because these parameters have been reported to be unaffected
by coffee (15,16). Coffee has been reported to impair the intestinal absorption of a number of
medications and other substances (17-24) (Table 2), and very recently we added L-T4 to the list
based on the said 8 cases observed and in vitro studies suggesting a sequestering effect (3).
and compliance with the drug; b) the pharmaceutical characteristics of L-T4 and c) the interference
of other medications (4). Several oral medications inhibit the intestinal absorption of L-T4 sodium
when taken simultaneously with thyroid hormone. In most of these cases, the malabsorption of L-
T4 is due to the binding of the hormone to medications, forming an insoluble or non-absorbable
complex: these include cholestyramine (5), ferrous sulphate (6), aluminium hydroxide (7), calcium
carbonate (8), sucralfate (9). Besides, L-T4 should be taken separately from food, since food
adsorbs thyroid hormone, decreasing its availability for intestinal absorption (10-12): in particular,
dietary fibres and herbal remedies reduce intestinal absorption of L-T4 (13,14).
Drugs are absorbed after oral administration as a consequence of interactions between the
drug, its formulation and the gastrointestinal tract. Based on the in vitro studies described in ref. 3,
at least one mechanism for the interference of coffee is physical sequestration of L-T4; however,
we cannot exclude other possibilities. These possibilities should not include changes in gastric
empting, intestinal transit or pH, because these parameters have been reported to be unaffected
by coffee (15,16). Coffee has been reported to impair the intestinal absorption of a number of
medications and other substances (17-24) (Table 2), and very recently we added L-T4 to the list
based on the said 8 cases observed and in vitro studies suggesting a sequestering effect (3).


 Thus, regardless of type, coffee should act in vivo by sequestering L-T4 and reducing hormone
availability for uptake by the intestinal epithelium (Fig. 1).
Fig. 1 Sequestering activity of coffee reduces intestinal absorption of L-T4.
Thus, regardless of type, coffee should act in vivo by sequestering L-T4 and reducing hormone
availability for uptake by the intestinal epithelium (Fig. 1).
Fig. 1 Sequestering activity of coffee reduces intestinal absorption of L-T4. 


 13. Woeber KA. Treatment of hypothyroidism. In: Braverman LE, Utiger RD (eds) Werner and
Ingbar’s The Thyroid, 9th edition. Lippincott Williams & Wilkins, Philadelphia, 2005. pp 864-
14. Centanni M, Gargano L, Canettieri G, Viceconti N, Franchi A, Delle Fave G, Annibale A.
Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis. N Engl J Med 354:
15. Ehrlich A, Basse H, Henkel-Ernst J, Hey B, Menthe J, Lucker PW. Effect of differently
processed coffee on the gastric potential difference and intragastric pH in healthy
volunteers. Methods Find Exp Clin Pharmacol 20:155-161, 1998.
16. van Nieuwenhoven MA, Brummer RM, Brouns F. Gastrointestinal function during exercise:
comparison of water, sports drink, and sports drink with caffeine. J Appl Physiol 89:1079-
17. Traganos F, Kapuscinski J, Gong J, Ardelt B, Darzynkiewicz RJ, Darzynkiewicz Z. Caffeine
prevents apoptosis and cell cycle effects induced by camptothecin or topotecan in HL-60
18. Gertz BJ, Holland SD, Kline WF, Matuszewski BK, Freeman A, Quan H, Lasseter KC,
Mucklow JC, Porras AG. Studies of the oral bioavailability of alendronate. Clin Pharmacol
19. Drugs interactions: factors affecting response to drugs: Merck Manual home edition.
Available at: http://www.merck.com/mmhe/sec02/ch013/ch013c.html (accessed January
20. Cabrera Forneiro J, Chamorro Merino G, González Alfonso M, Ramón Jarne FJ.
Bioavailability of haloperidol in nutritive solutions: clinical implications. Arch Neurobiol
21. Lasswell WL Jr, Weber SS, Wilkins JM. In vitro interaction of neuroleptics and tricylic
antidepressants with coffee, tea, and gallotannic acid. J Pharm Sci 73:1056-1058, 1984.
22. Kiel DP, Felson DT, Hannan MT, Anderson JJ, Wilson PW. Caffeine and the risk of hip
fracture: the Framingham Study. Am J Epidemiol 132: 675-684, 1990.
23. Morck TA, Lynch SR, Cook JD. Inhibition of food iron absorption by coffee. Am J Clin Nutr
24. FMI – Mechanisms of food medications interactions. Available at:
http://www.foodmedinteractions.com/mechs.html (accessed January 2009).
13. Woeber KA. Treatment of hypothyroidism. In: Braverman LE, Utiger RD (eds) Werner and
Ingbar’s The Thyroid, 9th edition. Lippincott Williams & Wilkins, Philadelphia, 2005. pp 864-
14. Centanni M, Gargano L, Canettieri G, Viceconti N, Franchi A, Delle Fave G, Annibale A.
Thyroxine in goiter, Helicobacter pylori infection, and chronic gastritis. N Engl J Med 354:
15. Ehrlich A, Basse H, Henkel-Ernst J, Hey B, Menthe J, Lucker PW. Effect of differently
processed coffee on the gastric potential difference and intragastric pH in healthy
volunteers. Methods Find Exp Clin Pharmacol 20:155-161, 1998.
16. van Nieuwenhoven MA, Brummer RM, Brouns F. Gastrointestinal function during exercise:
comparison of water, sports drink, and sports drink with caffeine. J Appl Physiol 89:1079-
17. Traganos F, Kapuscinski J, Gong J, Ardelt B, Darzynkiewicz RJ, Darzynkiewicz Z. Caffeine
prevents apoptosis and cell cycle effects induced by camptothecin or topotecan in HL-60
18. Gertz BJ, Holland SD, Kline WF, Matuszewski BK, Freeman A, Quan H, Lasseter KC,
Mucklow JC, Porras AG. Studies of the oral bioavailability of alendronate. Clin Pharmacol
19. Drugs interactions: factors affecting response to drugs: Merck Manual home edition.
Available at: http://www.merck.com/mmhe/sec02/ch013/ch013c.html (accessed January
20. Cabrera Forneiro J, Chamorro Merino G, González Alfonso M, Ramón Jarne FJ.
Bioavailability of haloperidol in nutritive solutions: clinical implications. Arch Neurobiol
21. Lasswell WL Jr, Weber SS, Wilkins JM. In vitro interaction of neuroleptics and tricylic
antidepressants with coffee, tea, and gallotannic acid. J Pharm Sci 73:1056-1058, 1984.
22. Kiel DP, Felson DT, Hannan MT, Anderson JJ, Wilson PW. Caffeine and the risk of hip
fracture: the Framingham Study. Am J Epidemiol 132: 675-684, 1990.
23. Morck TA, Lynch SR, Cook JD. Inhibition of food iron absorption by coffee. Am J Clin Nutr
24. FMI – Mechanisms of food medications interactions. Available at:
http://www.foodmedinteractions.com/mechs.html (accessed January 2009).