Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients cialis uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Pone.0032122 1.7
Point-of-Care Test for Detection of Urogenital Chlamydiain Women Shows Low Sensitivity. A PerformanceEvaluation Study in Two Clinics in Suriname
Jannie J. van der Helm1, Leslie O. A. Sabajo2, Antoon W. Grunberg3, Servaas A. Morre´4,5, Arjen G. C. L.
Speksnijder6, Henry J. C. de Vries1,7,8,9*
1 STI Outpatient Clinic, Cluster Infectious Diseases, Public Health Service Amsterdam, Amsterdam, The Netherlands, 2 Dermatological Service, Ministry of Health,
Paramaribo, Suriname, 3 Lobi Foundation, Paramaribo, Suriname, 4 VU University Medical Center, Amsterdam, The Netherlands, 5 Institute of Public Health Genomics,
Department of Genetics and Cell Biology, Research Institutes CAPHRI and GROW, Faculty of Health, Medicine & Life Sciences, University of Maastricht, Maastricht, The
Netherlands, 6 Public Health Laboratory, Cluster Infectious Diseases, Public Health Service Amsterdam, Amsterdam, The Netherlands, 7 Department of Dermatology,
Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands, 8 Centre for Infections and Immunity Amsterdam, Academic Medical Center, University
of Amsterdam, Amsterdam, The Netherlands, 9 Centre for Infectious Disease Control, National Institute of Public Health and the Environment, Bilthoven, The Netherlands
Background: In general, point-of-care (POC) tests for Chlamydia trachomatis (Ct) show disappointing test performance,especially disappointing sensitivity results. However, one study sponsored by the manufacturer (Diagnostics for the RealWorld) reported over 80% sensitivity with their Chlamydia Rapid Test (CRT). We evaluated the performance of this CRT in anon–manufacturer-sponsored trial.
Methods: Between July 2009 and February 2010, we included samples from 912 women in both high- and low-risk clinicsfor sexually transmitted infections (STIs) in Paramaribo, Suriname. Sensitivity, specificity, positive- and negative predictivevalues (PPV and NPV) for CRT compared to NAAT (Aptima, Gen-Probe) were determined. Quantitative Ct load and humancell load were determined in all CRT and/or NAAT positive samples.
Results: CRT compared to NAAT showed a sensitivity and specificity of 41.2% (95% CI, 31.9%–50.9%) and 96.4% (95% CI,95.0%–97.5%), respectively. PPV and NPV were 59.2% (95% CI, 47.5%–70.1%) and 92.9% (95% CI, 91.0%–94.5%), respectively. Quantitative Ct bacterial load was 73 times higher in NAAT-positive/CRT-positive samples compared to NAAT-positive/CRT-negative samples (p,0.001). Human cell load did not differ between true-positive and false-negative CRT results (p = 0.835). Sensitivity of CRT in samples with low Ct load was 12.5% (95% CI, 5.2%–24.2%) and in samples with high Ct load 73.5% (95%CI, 59.9%–84.4%).
Conclusions: The sensitivity of CRT for detecting urogenital Ct in this non–manufacturer-sponsored study did not meet theexpectations as described previously. The CRT missed samples with a low Ct load. Improved POC are needed as meaningfuldiagnostic to reduce the disease burden of Ct.
Citation: van der Helm JJ, Sabajo LOA, Grunberg AW, Morre´ SA, Speksnijder AGCL, et al. (2012) Point-of-Care Test for Detection of Urogenital Chlamydia inWomen Shows Low Sensitivity. A Performance Evaluation Study in Two Clinics in Suriname. PLoS ONE 7(2): e32122. doi:10.1371/journal.pone.0032122
Editor: Deborah Dean, University of California San Francisco, University of California, Berkeley, and the Children’s Hospital Oakland Research Institute, UnitedStates of America
Received November 3, 2011; Accepted January 19, 2012; Published February 29, 2012
Copyright: ß 2012 van der Helm et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: This work was supported by the Research and Development fund of the Municipal Health Service of Amsterdam [project no 2369 and 2371] and AGIShealthcare insurance [RVVZ no 1417000]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of themanuscript.
Competing Interests: The authors have declared that no competing interests exist.
tion Tests (NAAT), but they are expensive and requiresophisticated laboratory conditions [5]. This makes NAAT
Urogenital chlamydia is the most prevalent, curable bacterial
unsuitable for the detection of Ct for most low-resource settings
sexually transmitted infection (STI) worldwide [1], with a
[6]. Therefore the World Health organization (WHO) has
significant public health burden, especially in young women [2].
launched a priority program that is designated to develop
The causative bacterium, Chlamydia trachomatis (Ct) causes a high
affordable and reliable point-of-care (POC) tests for STIs that
rate of asymptomatic infections [3] and is associated with adverse
are predominant in low resource countries [http://www.who.int/
outcomes like infertility, ectopic pregnancy and pelvic inflamma-
std_diagnostics]. In this program, WHO has formulated the
tory disease (PID) [4]. To reduce transmission and late
ASSURED criteria that POC tests have to meet: Affordable,
complications, active case finding and early treatment are critical
Sensitive, Specific, User-friendly, Robust and rapid, Equipment-
strategies. The standard diagnostics are Nucleic Acid Amplifica-
free, Deliverable to those who need them [7]. The POC test result
February 2012 | Volume 7 | Issue 2 | e32122
should be readily available, while the patient waits, to ensure
Specimen collection and testing procedures
prompt treatment. This is especially important where patient
Nurse-collected vaginal swabs were obtained blindly for the
return for treatment is low. It is estimated that a POC test of
Chlamydia Rapid Test (CRT) (Diagnostics for the Real World
moderate sensitivity (63%) combined with immediate treatment
(Europe), Cambridge, UK) and NAAT (Aptima, Gen-Probe, San
on-site may lead to the treatment of more infected individuals than
Diego, USA) testing using a cross-over model. This means that in
an ultra-sensitive and specific NAAT alone when patient return is
the first half of the included women the swab for the CRT was taken
low [8]. Moreover, counselling messages are most efficient when a
first and the second of the included women NAAT was taken first.
diagnosis can be communicated during the same consultation [9].
Nurses were trained to collect the swabs before routine speculum
These advantages are relevant for industrialized countries as well,
examination was performed. A minimum period of 10 times for
even if POC tests have a lower sensitivity than standard NAAT.
CRT and 10 seconds for NAAT of contact between the tip of the
To date, POC tests for urogenital chlamydia show disappoint-
swab and the vaginal wall in a rotating motion was ensured. CRT
ing test characteristics, especially low sensitivity. In a recent
was immediately performed according to the manufacturer’s
evaluation, three POC tests for urogenital chlamydia, currently on
instructions on-site in the laboratory. All technicians that performed
the market, showed poor sensitivity between 12% and 17% in a
the CRT were trained with proficiency panels as provided and
non–manufacturer-sponsored clinical study [10]. In contrast, one
instructed by the manufacturer. Technicians did not receive
POC test for urogenital chlamydia (Diagnostics for the Real
information about the participant. The test results were interpreted
World, Cambridge, UK) especially developed for low-resource
and recorded by two laboratory technicians separately. CRT results
countries has an asserted sensitivity of over 80% [11]. A
were defined as indeterminate when the laboratory technicians
manufacturer-sponsored diagnostic field study in the Philippines
reported discordant results or when CRT failed (i.e. control line did
revealed sensitivities of 71% and 87% among women at high risk
not appear). The samples for NAAT testing were collected
and low risk for STI, respectively [12]. Suriname, South America,
according to the manufacturer’s instructions, and shipped to the
is a low-resource country and affordable and reliable diagnostics to
Public Health Laboratory in Amsterdam where they were tested
detect Ct are urgently needed. Therefore, we aimed to evaluate
within 50 days after collection. NAAT test results were communi-
the performance of this promising POC test in two outpatient
cated with the two recruitment sites in Suriname and participants
clinics in Suriname, with the objective to use this test for
with a positive-Ct NAAT were treated with doxycycline 100 mg bid
intervention of the chlamydia epidemic.
for 7 days at Lobi Foundation and 10 days bid at theDermatological Service or, in case of (possible) pregnancy, with a
single 1000 mg oral dose of azithromycin.
The study was approved by the ethical committee of the
The CRT was performed as described previously [13]. Version
Ministry of Health of the Republic of Suriname (VG010-2007)
6.1 of the Chlamydia Rapid Test (Professional use) (P/N 1200-20)
and the ethical committee of the Academic Medical Centre,
instructions for use (C03-0008) was used. Shortly, each swab was
University of Amsterdam, the Netherlands (MEC07/127). Patients
subjected to extraction by sequential addition of 400 ml of reagent
were recruited at two sites in Paramaribo, Suriname:
1, 300 ml of reagent 2, and 100 ml of reagent 3 to the swab in a
The Dermatological Service, an integrated outpatient clinic
tapered sample preparation tube, with gentle mixing between
that offers free-of-charge examination and treatment of STIs
additions. The sample preparation reagents were administered
and infectious skin diseases like leprosy and leishmaniasis. All
with unit dose pipettes. The extraction tube was then capped and
consecutive women who visited for an STI check-up were
used as a dropper to deliver 5 drops (approximately 100 ml) of the
asked to participate in the study and were considered to be at
extracted sample to a tube containing the lyophilized amplification
and detection reagents. The resulting mixture was agitated gentlyuntil a clear pink solution was obtained, after which the test strip,
The Lobi Foundation is a center for birth control and sexual
coated with a monoclonal antibody to chlamydial lipopolysaccha-
health. As women who visit this clinic do not attend primarily
ride (LPS) and including a procedural control, was added to the
to be checked for STI, these participants were considered to
solution and allowed to stand for 25 minutes before the result was
read. Each swab was subjected to one extraction. The test strip
Recruitment took place between July 2009 and February 2010.
was used in the interpretation of the result; a clearly visible test line
Exclusion criteria were: use of antibiotics in the past 7 days, age
indicated a positive result, provided that the control line was also
younger than 18 years and previous participation. After written
informed consent, patients were given a unique code toparticipate anonymously. Participants were interviewed about
demographic characteristics, including self-reported ethnicity as
For NAAT testing, the monospecific Aptima chlamydia assay
Suriname is a multiethnic society, with many ethnic groups such
for the detection of Chlamydia trachomatis rRNA (Gen-Probe Inc.,
as Creoles and Maroons (both descendants from the African
San Diego, USA) was used with the accompanying vaginal swab
diaspora due to slave trade), Hindustani, Javanese, and Chinese
specimen collection kit. The protocols described in the package
(all descendants from labor immigrants), Caucasians (descendants
inserts were followed. Technicians performing NAAT were
from Dutch farmers), indigenous Amerindian people and Mixed
blinded to the results of the POC-Ct and did not receive clinical
race persons. Moreover, participants were asked about willing-
information. This NAAT is an FDA-approved commercial test
ness to wait for POC test results, although in our study
and was used to estimate the Ct prevalence at both study sites.
participants did not receive the results from POC, and if theyused any products for vaginal hygiene like douches, herbs, or
other home products, and if so, in what frequency. Data were
Quantitative Ct load was determined for samples with a
discrepant test result between CRT and NAAT, and for samples
February 2012 | Volume 7 | Issue 2 | e32122
that tested positive for CRT as well as for NAAT using a real-time
excluded from the CRT performance evaluation due to either
PCR targeting the cryptic plasmid [14]. Ct load was expressed as
discrepancy in CRT result between two lab technicians (n = 3) or
inclusion forming units (IFU) based on defined serial dilutions of
Ct cultured in human cells with over .90% infected HeLa cells of
General characteristics of the 912 women included in the CRT
100 IFU to 0.001 IFU taking into account also DNA from non-
performance evaluation are shown in Table 1. Their median age
viable Ct particles. The human cell load was assessed by
was 30 years (IQR 25–36), 336 (36.9%) were of Creole/Maroon
determination of human HLA copies in combination with a
ethnicity and 229 (25.1%) were of Hindustani ethnicity. Twenty-
defined serial dilution of quantified human DNA using the fol-
one (2.3%) women reported having had sex for money or goods.
lowing primer probe combination: HLA-F 59-TTG-TAC-CAG-
Almost all women 900 (98.7%) would wait for the CRT test result
TTT-TAC-GGT-CCC-39 HLA-R 59- TGG-TAG-CAG-CGG-
if the test were a standard offering in their clinic. Of these women,
TAG-AGT-TG,-3 and HLA-Probe 59-FAM- TTC TAC GTG
660 (73.3%) would be willing to wait for a maximum of half an
GAC CTG GAG AGG AAG GAG -BHQ1-39. By using a
hour to receive the results, the other 240 (26.7%) would be willing
chlamydial and a human target, the average chlamydial/human
cell ratio, and IFU/swab were calculated [10].
Ct prevalence and CRT performance results
Ct prevalence was 20.8% in the high-risk population (visiting
To evaluate the performance of CRT compared to NAAT
the Dermatological Service) and 9.2% in the low-risk population
sensitivity, specificity, positive predictive value (PPV) and negative
(visiting Lobi Foundation). Combining the results of the two sites,
predictive value (NPV) were calculated using standard methods.
the sensitivity and specificity of the CRT in identifying Ct
Specimens with indeterminate results by CRT were excluded. An
compared to NAAT were 41.2% (95% CI, 31.9%–50.9%) and
independent t-test was used to compare log-transformed Ct loads
96.4% (95% CI, 95.0%–97.5%), respectively. PPV of the CRT
between true-positive and false-negative CRT results. Analyses
was 59.2% (95% CI, 47.5%–70.1%) and NPV was 92.9% (95%
were performed with SPSS package version 19.0 (SPSS Inc.,
CI, 91.0%–94.5%). Sensitivity and specificity of CRT compared
to NAAT were comparable for the high-risk population (39.4%
The study has been reported according to the STARD checklist
and 94.4%) and the low-risk population (42.0% and 96.8%)
for the reporting of studies of diagnostic accuracy.
Quantitative Ct bacterial load and human HLA were assessed
for the samples that showed discrepant results for CRT and
In total, 1019 women were asked to participate in the study, of
NAAT (n = 89) and for samples that were CRT and NAAT
whom 917 were included and 102 did not meet the inclusion
positive (n = 42). Ct bacterial load could be detected in 99/131
criteria or declined to participate (Figure 1). Five women were
samples and human HLA in 126/131 samples. Of the 42 samples
Figure 1. Flow chart of specimen collection for the evaluation of a Chlamydia Rapid Test test as diagnostic for urogenital chlamydiain women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010. NAAT; Aptima chlamydia single test, Genprobe(control test) CRT; Chlamydia Rapid Test, Diagnostics for the Real World (evaluated test). doi:10.1371/journal.pone.0032122.g001
February 2012 | Volume 7 | Issue 2 | e32122
Table 1. General characteristics of the 912 women included in the evaluation of a Chlamydia Rapid Test as diagnostic forurogenital chlamydia in women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010.
Maximum time these women are willing to wait
Frequency of cleansing among those who practice vaginal cleansing
IQR; interquartile range. doi:10.1371/journal.pone.0032122.t001
Table 2. Performance results of the Diagnostics for the Real World Chlamydia Rapid Test (CRT) compared to NAAT (Aptimachlamydia single test).
Evaluation of a CRT as diagnostic for urogenital chlamydia in women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010. PPV; positive predictive value. NPV; negative predictive value. 95% CI; 95% confidence interval. doi:10.1371/journal.pone.0032122.t002
February 2012 | Volume 7 | Issue 2 | e32122
that tested positive for CRT and NAAT, quantitative Ct bacterial
load was detected in all 42 samples and human HLA in 39samples. Of the 60 samples that tested CRT negative and NAAT
We found a disappointingly low clinical sensitivity of 42.0% and
positive, quantitative Ct bacterial load was detected in 55 samples
39.4% of the CRT in low-risk and high-risk Surinamese women,
and human HLA in all 60 samples. Of the 29 samples that tested
respectively, compared to the sensitivity of 86.8% in low-risk
CRT positive and NAAT negative, quantitative Ct bacterial load
women and 71% in high-risk women in the Philippines, reported
was detected in 2 samples and human HLA in 27 samples
earlier in a study supported by the manufacturer [12]. The
discrepancy might partly be explained by the use of a differentreference test. Where we used Gen-Probe’s Aptima platform as a
Quantitative Ct bacterial load was 73 times higher in NAAT-
reference test, in the Philippines study the Roche Amplicor (Roche
positive/CRT-positive samples (geometric mean 120 IFU) com-
Molecular Systems, Branchburg, NJ) was used. Although current
pared to NAAT-positive/CRT-negative samples (geometric mean
generation NAATs have comparable sensitivities, NAAT could be
1.64 IFU, p,0.001). Human DNA concentration did not differ
more sensitive than Roche Amplicor [15]. A somewhat lower
sensitivity of CRT in our study could be expected with a more
(p = 0.835). The average chlamydial/human cell load ratio (Ct
sensitive control test, but this does not explain the large difference
concentration) was 60 times higher in NAAT-positive samples
in sensitivity found in the Philippine study and our results.
where CRT detected Ct infection (geometric mean 0.32 IFU/
Another explanation for the lower sensitivity we found could be
human cell) compared to loads that CRT did not detect (geometric
attributed to a different wash-out period for antibiotic use between
mean 0.0053 IFU/human cell, p,0.001). Quantitative HLA load
the two studies. We excluded women who used antibiotics in the
was comparable for NAAT-positive/CRT-positive samples (geo-
last 7 days, while in the Philippines study women who used
metric mean 344 cells) compared to NAAT-negative/CRT-
antibiotics in the previous month were excluded. Time to
positive samples (geometric mean 451 cells, p = 0.424).
clearance of LPS antigen, which is targeted by the CRT, might
Quantitative Ct loads were comparable for women reporting
be shorter after antibiotic use than time to clearance of Ct rRNA,
symptoms like vaginal discharge, irregular menstruation, pain
which is targeted by NAAT [16]. This could have caused the
during intercourse, lower abdominal pain or dysuria and women
occurrence of false-positive NAAT samples, and consequently
without the specific symptom (data not shown). Women visiting
more false-negative CRT samples could be expected. Low
the high-risk STI clinic had comparable quantitative Ct loads with
sensitivity of the CRT due to inadequate collection resulting in a
those visiting the low-risk clinic (p = 0.525). Sensitivity of the CRT
low sample yield could be ruled out since the human cell load in
was comparable for those who practiced any vaginal hygienic
samples with true-positive and false-negative CRT results was
measures, 37.5% (95% CI, 23.6%–53.1%), compared to those
comparable. The CRT had a 96.4% specificity. False-positive
who did not practice vaginal cleansing, 43.3% (95% CI, 31.3%–
CRT results could have been caused by cross reactivity with C.
56.0%). When comparing women who practice vaginal cleansing
ptsittaci or C. pneumoniae as described in the manufacturers manual.
frequently, at least once a week, with those who cleanse less than
Yet infections with these organisms in the urogenital tract in
once weekly, sensitivity of CRT yields comparable results, 39.1%
humans are uncommon [17,18]. As a false positive chlamydia
(95% CI, 21.1%–59.8%) and 27.3% (95% CI, 7.5%–57.8%),
diagnosis can have serious adverse social consequences a specificity
of 96,4% is undesirable, especially in low prevalent settings. The
Based on the overall median Ct load, NAAT-positive samples
CRT in our study had a few modifications compared to the study
were divided in two groups with either a low- (range 0.006–12.5
in the Philippines. We used unit dose pipettes instead of unit dose
IFU) or high-grade quantitative bacterial Ct load (range 13.5–
vials. Also, the nitrocellulose membrane was changed by the
6470 IFU). In the low-grade bacterial load group, the CRT
manufacturer and according to the manual, only one dipstick had
sensitivity was 12.5% (95% CI, 5.2%–24.2%), whereas in the high-
to be used to interpret the results. However, when a test is renewed
grade Ct load group the sensitivity was 73.5% (95% CI, 59.9%–
one might expect at least comparable diagnostic characteristics
Table 3. C. trachomatis quantitative bacterial load and human cell load measurements in concordant and discordant samples withNAAT (Aptima chlamydia single test) and the Diagnostics for the Real World Chlamydia Rapid Test (CRT).
Geometric mean human cell load (HLA copy)
Concentration Ct load per human cell assessed (IFU/HLA copy)
Geometric mean of concentration (IFU/HLA copy)
Evaluation of a CRT as diagnostic for urogenital chlamydia in women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010. IFU; inclusion forming units. HLA; human leucocyte antigen gene. doi:10.1371/journal.pone.0032122.t003
February 2012 | Volume 7 | Issue 2 | e32122
In the CRT evaluation study performed in the Philippines, the
commercially available products [10]. Still, with a sensitivity of
Ct prevalence was 6.3% in the low-risk group (women visiting an
only 41.7%, this test performs under the minimally required
obstetrics-gynaecology clinic) and 17.9 to 32% in the high-risk
sensitivity of 63% required for a POC test to treat more infected
group (female sex workers), which compares well with the
individuals than the standard NAAT in a setting with low patient
prevalences found in our study, 9.2% and 20.8% respectively.
return (,65%), [8]. On the other hand, in situations where
The sensitivity figures found in our study were comparable for
transmission during treatment delay and low return for treatment
low-risk and high-risk women, 42.0% and 39.4% respectively.
are considerable, even a POC test with a sensitivity below 63%
Quite surprisingly, in the Philippines study a much lower
could be beneficial in the prevention of ongoing STI transmission
sensitivity was found in the high-risk group compared to the
[23]. A recent economic evaluation analysis using the same CRT
low-risk group. The authors explain this finding as a result of the
as we evaluated in this study, showed that in the UK using NAAT
use of vaginal creams and other feminine hygiene products, which
is more cost-effective. [24]. In that evaluation, a sensitivity
can interfere with the CRT. In our study, the sensitivity of CRT
between 73% and 85% for the CRT was assumed.
was comparable for women who practiced any vaginal cleansing
POC tests available for systemic infections like HIV and syphilis
are highly sensitive since they are based on the detection of serum
Although we consider the population recruited at Lobi
antibodies [25,26]. Infections caused by organisms like Ct (but also
Foundation a low risk group, with a prevalence of 9.2% this
N. gonorrhoeae) are confined to mucosal tissue and normally invoke
population would be considered high risk in many settings. Yet,
little to no production of antibodies. Therefore, the development
with a prevalence of 20.8% as found at the Dermatological
of POC tests to diagnose mucosal Ct infections based on the
Service, the difference in prevalence between the two study sites is
detection of serum antibodies is, at least for now, not an option.
Improved POC tests for Ct need to detect bacterial antigens or
The sensitivity of CRT is higher in samples with a high bacterial
nucleic acids, even in cases with a low bacterial load. Promising
load. The clinical relevance of organism load is still debated, but it
steps have been made in the field of POC HIV-load NAAT using
is suggested that infections with high organism loads are more
nanotechnology [27]. Along the same lines, a POC test for
likely to lead to cervicitis or PID and are associated with multiple
urogenital chlamydia with sufficient sensitivity could be developed.
patient-reported symptoms [19]. However, the association with
Until reliable and affordable diagnostics are available, algorithms
patient-reported symptoms was only found with first-void urine
for syndromic management can be used for low-resource settings,
and endocervical samples and not with self-collected vaginal
although the success of algorithms for vaginal discharge varies
samples. In our study, where nurse-collected vaginal swabs were
used, quantitative Ct loads were not significantly different for
In conclusion, the evaluated CRT of Diagnostics for the Real
asymptomatic women and women reporting one or multiplesymptoms such as vaginal discharge or dysuria.
World has no added value in the management of Ct infections due
The NAAT platform is a latest generation highly sensitive
to its low test performance. There is an urgent need for POC
commercial diagnostic test for Ct [20]. However no test is 100%
diagnostics for the detection of urogenital chlamydia meeting the
accurate and a positive bacterial Ct load signal was detected in two
ASSURED criteria, including adequate sensitivity.
samples that were NAAT negative and CRT positive. One samplehad a Ct load of 62.9 IFU which might be explained by inhibition
of high target load [21]. The other sample had a very low load of
The authors would like to express their gratitude to all nurses and
0.00261 IFU. Since the frequency of these discrepancies was
laboratory technicians of the Dermatological Service and the Lobi
extremely low, we do not consider that this finding significantly
Foundation for data collection, and Susan T. Landry for editing the final
A recent field study of the same CRT test but to detect ocular
chlamydia infection (trachoma) found similar disappointingly low
sensitivity (33.3%–67.9%) and specificity (92.4%–99.0%) [22].
Conceived and designed the experiments: JvdH LS SM AS HdV.
Most commercially available and clinically evaluated POC tests
Performed the experiments: JvdH AG SM AS. Analyzed the data: JvdH
for urogenital chlamydia show poor sensitivity results [10].
SM HdV. Contributed reagents/materials/analysis tools: LS AG SM AS
Compared with the results found in our evaluation, the CRT of
HdV. Wrote the paper: JvdH LS AG SM HdV.
Diagnostics for the Real World outperforms some of the other
1. World Health Organization. Global prevalence and incidence of selected cur-
7. Peeling RW, Holmes KK, Mabey D, Ronald A (2006) Rapid tests for sexually
able sexually transmitted infections: Overview and estimates. Geneva,
transmitted infections (STIs): the way forward. Sex Transm Infect 82 Suppl 5: v1–v6.
Switzerland: World Health Organization, 2001, Available: http://www.who.
8. Gift TL, Pate MS, Hook EW, Kassler WJ (1999) The rapid test paradox: when
int/hiv/pub/sti/pub7/en/ Accessed 2012 Jan 30.
fewer cases detected lead to more cases treated: a decision analysis of tests for
2. Datta SD, Sternberg M, Johnson RE, Berman S, Papp JR, et al. (2007)
Chlamydia trachomatis. Sex Transm Dis 26: 232–240.
Gonorrhea and chlamydia in the United States among persons 14 to 39 years of
9. Sanders GD, Anaya HD, Asch S, Hoang T, Golden JF, et al. (2010) Cost-
age, 1999 to 2002. Ann Intern Med 147: 89–96.
effectiveness of strategies to improve HIV testing and receipt of results: economic
3. Farley TA, Cohen DA, Elkins W (2003) Asymptomatic sexually transmitted
analysis of a randomized controlled trial. J Gen Intern Med 25: 556–563.
diseases: the case for screening. Prev Med 36: 502–509.
10. van Dommelen L, van Tiel FH, Ouburg S, Brouwers EE, Terporten PH, et al.
4. Land JA, van Bergen JE, Morre SA, Postma MJ (2010) Epidemiology of
(2010) Alarmingly poor performance in Chlamydia trachomatis point-of-care
Chlamydia trachomatis infection in women and the cost-effectiveness of
testing. Sex Transm Infect 86: 355–359.
screening. Hum Reprod Update 16: 189–204.
11. Mahilum-Tapay L, Laitila V, Wawrzyniak JJ, Lee HH, Alexander S, et al.
5. Peeling RW, Mabey D, Herring A, Hook EW (2006) Why do we need quality-
(2007) New point of care Chlamydia Rapid Test–bridging the gap between
assured diagnostic tests for sexually transmitted infections? Nat Rev Microbiol 4:
diagnosis and treatment: performance evaluation study. BMJ 335: 1190–1194.
12. Saison F, Mahilum-Tapay L, Michel CE, Buttress ND, Nadala EC, et al. (2007)
6. Petti CA, Polage CR, Quinn TC, Ronald AR, Sande MA (2006) Laboratory
Prevalence of Chlamydia trachomatis infection among low- and high-risk
medicine in Africa: a barrier to effective health care. Clin Infect Dis 42:
Filipino women and performance of Chlamydia rapid tests in resource-limited
settings. J Clin Microbiol 45: 4011–4017.
February 2012 | Volume 7 | Issue 2 | e32122
13. Michel CE, Solomon AW, Magbanua JP, Massae PA, Huang L, et al. (2006)
Chlamydia trachomatis in significantly more women by the APTIMA Combo 2
Field evaluation of a rapid point-of-care assay for targeting antibiotic treatment
assay. J Clin Microbiol 44: 400–405.
for trachoma control: a comparative study. Lancet 367: 1585–1590.
21. Birch L, Dawson CE, Cornett JH, Keer JT (2001) A comparison of nucleic acid
14. Catsburg A, Savelkoul PHM, Vliet A, Algra J, Vandenbroucke-Grauls CMJE,
amplification techniques for the assessment of bacterial viability. Lett Appl
et al. (2006) Development and evaluation of an internally controlled Real-Time
quantitative PCR assay for the detection of Chlamydia trachomatis. In:
22. Harding-Esch EM, Holland MJ, Schemann JF, Molina S, Sarr I, et al. (2011)
Chernesky M, Caldwell H, Christiansen G, et al. (2006) Eleventh International
Diagnostic accuracy of a prototype point-of-care test for ocular Chlamydia
Symposium on Human Chlamydial Infections. June 18–23, 2006, Niagara-on-
trachomatis under field conditions in The Gambia and Senegal. PLoS Negl
the-Lake, Ontario, Canada. pp 521–524.
15. Lowe P, O’Loughlin P, Evans K, White M, Bartley PB, et al. (2006) Comparison
23. Vickerman P, Watts C, Alary M, Mabey D, Peeling RW (2003) Sensitivity
of the Gen-Probe APTIMA Combo 2 assay to the AMPLICOR CT/NG assay
requirements for the point of care diagnosis of Chlamydia trachomatis and
for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in urine
Neisseria gonorrhoeae in women. Sex Transm Infect 79: 363–367.
samples from Australian men and women. J Clin Microbiol 44: 2619–2621.
24. Hislop J, Quayyum Z, Flett G, Boachie C, Fraser C, et al. (2010) Systematic
16. Renault CA, Israelski DM, Levy V, Fujikawa BK, Kellogg TA, et al. (2011)
review of the clinical effectiveness and cost-effectiveness of rapid point-of-caretests for the detection of genital chlamydia infection in women and men. Health
Time to clearance of Chlamydia trachomatis ribosomal RNA in women treated
for chlamydial infection. Sex Health 8: 69–73.
25. Delaney KP, Branson BM, Uniyal A, Phillips S, Candal D, et al. (2011)
17. Pospischil A, Thoma R, Hilbe M, Grest P, Gebbers JO (2002) Abortion in
Evaluation of the performance characteristics of 6 rapid HIV antibody tests. Clin
woman caused by caprine Chlamydophila abortus (Chlamydia psittaci serovar
26. Chin CD, Laksanasopin T, Cheung YK, Steinmiller D, Linder V, et al. (2011)
18. Whyte A, Garnett P, Thompson C, McMullen P (1998) Chlamydia pneumoniae
Microfluidics-based diagnostics of infectious diseases in the developing world.
in the female genital tract. J Infect 36: 245.
19. Michel CE, Sonnex C, Carne CA, White JA, Magbanua JP, et al. (2007)
27. Niemz A, Ferguson TM, Boyle DS (2011) Point-of-care nucleic acid testing for
Chlamydia trachomatis load at matched anatomic sites: implications for
infectious diseases. Trends Biotechnol 29: 240–250.
screening strategies. J Clin Microbiol 45: 1395–1402.
28. Pettifor A, Walsh J, Wilkins V, Raghunathan P (2000) How effective is
20. Chernesky M, Jang D, Luinstra K, Chong S, Smieja M, et al. (2006) High
syndromic management of STDs?: A review of current studies. Sex Transm Dis
analytical sensitivity and low rates of inhibition may contribute to detection of
February 2012 | Volume 7 | Issue 2 | e32122
GlaxoSmithKline, Uxbridge, Middlesex, United Kingdom Konsolidierung von Systemen mit der RBE Plus Solution Die RBE Plus Solution hilft uns dabei, unsere Geschäftsab-läufe hochqualitativ zu unterstützen. Steven Thavam, GlaxoSmithKline Als Hilfsmittel für diesen Prozess wählte GlaxoSmith-Kline die RBE Plus Solution von IBIS Prof. Thome AG. Mit über 100.000 Mitarbeitern und mehreren Produ
 Point-of-Care Test for Detection of Urogenital Chlamydiain Women Shows Low Sensitivity. A PerformanceEvaluation Study in Two Clinics in Suriname
Jannie J. van der Helm1, Leslie O. A. Sabajo2, Antoon W. Grunberg3, Servaas A. Morre´4,5, Arjen G. C. L.
Point-of-Care Test for Detection of Urogenital Chlamydiain Women Shows Low Sensitivity. A PerformanceEvaluation Study in Two Clinics in Suriname
Jannie J. van der Helm1, Leslie O. A. Sabajo2, Antoon W. Grunberg3, Servaas A. Morre´4,5, Arjen G. C. L. should be readily available, while the patient waits, to ensure
Specimen collection and testing procedures
prompt treatment. This is especially important where patient
Nurse-collected vaginal swabs were obtained blindly for the
return for treatment is low. It is estimated that a POC test of
Chlamydia Rapid Test (CRT) (Diagnostics for the Real World
moderate sensitivity (63%) combined with immediate treatment
(Europe), Cambridge, UK) and NAAT (Aptima, Gen-Probe, San
on-site may lead to the treatment of more infected individuals than
Diego, USA) testing using a cross-over model. This means that in
an ultra-sensitive and specific NAAT alone when patient return is
the first half of the included women the swab for the CRT was taken
low [8]. Moreover, counselling messages are most efficient when a
first and the second of the included women NAAT was taken first.
should be readily available, while the patient waits, to ensure
Specimen collection and testing procedures
prompt treatment. This is especially important where patient
Nurse-collected vaginal swabs were obtained blindly for the
return for treatment is low. It is estimated that a POC test of
Chlamydia Rapid Test (CRT) (Diagnostics for the Real World
moderate sensitivity (63%) combined with immediate treatment
(Europe), Cambridge, UK) and NAAT (Aptima, Gen-Probe, San
on-site may lead to the treatment of more infected individuals than
Diego, USA) testing using a cross-over model. This means that in
an ultra-sensitive and specific NAAT alone when patient return is
the first half of the included women the swab for the CRT was taken
low [8]. Moreover, counselling messages are most efficient when a
first and the second of the included women NAAT was taken first.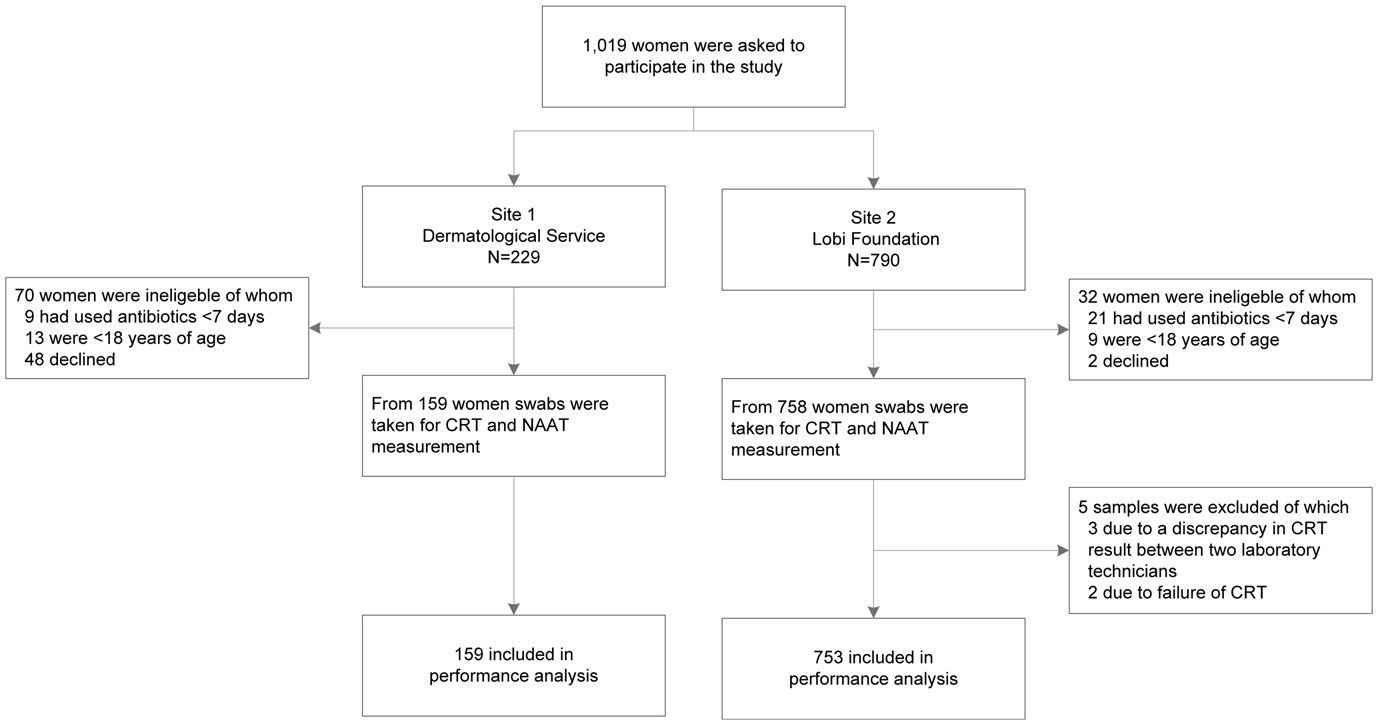
 that tested positive for CRT as well as for NAAT using a real-time
excluded from the CRT performance evaluation due to either
PCR targeting the cryptic plasmid [14]. Ct load was expressed as
discrepancy in CRT result between two lab technicians (n = 3) or
inclusion forming units (IFU) based on defined serial dilutions of
Ct cultured in human cells with over .90% infected HeLa cells of
General characteristics of the 912 women included in the CRT
100 IFU to 0.001 IFU taking into account also DNA from non-
performance evaluation are shown in Table 1. Their median age
viable Ct particles. The human cell load was assessed by
was 30 years (IQR 25–36), 336 (36.9%) were of Creole/Maroon
determination of human HLA copies in combination with a
ethnicity and 229 (25.1%) were of Hindustani ethnicity. Twenty-
defined serial dilution of quantified human DNA using the fol-
one (2.3%) women reported having had sex for money or goods.
that tested positive for CRT as well as for NAAT using a real-time
excluded from the CRT performance evaluation due to either
PCR targeting the cryptic plasmid [14]. Ct load was expressed as
discrepancy in CRT result between two lab technicians (n = 3) or
inclusion forming units (IFU) based on defined serial dilutions of
Ct cultured in human cells with over .90% infected HeLa cells of
General characteristics of the 912 women included in the CRT
100 IFU to 0.001 IFU taking into account also DNA from non-
performance evaluation are shown in Table 1. Their median age
viable Ct particles. The human cell load was assessed by
was 30 years (IQR 25–36), 336 (36.9%) were of Creole/Maroon
determination of human HLA copies in combination with a
ethnicity and 229 (25.1%) were of Hindustani ethnicity. Twenty-
defined serial dilution of quantified human DNA using the fol-
one (2.3%) women reported having had sex for money or goods. Table 1. General characteristics of the 912 women included in the evaluation of a Chlamydia Rapid Test as diagnostic forurogenital chlamydia in women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010.
Table 1. General characteristics of the 912 women included in the evaluation of a Chlamydia Rapid Test as diagnostic forurogenital chlamydia in women at two study sites in Paramaribo, Suriname, from July 2009 to February 2010. that tested positive for CRT and NAAT, quantitative Ct bacterial
load was detected in all 42 samples and human HLA in 39samples. Of the 60 samples that tested CRT negative and NAAT
We found a disappointingly low clinical sensitivity of 42.0% and
positive, quantitative Ct bacterial load was detected in 55 samples
39.4% of the CRT in low-risk and high-risk Surinamese women,
and human HLA in all 60 samples. Of the 29 samples that tested
respectively, compared to the sensitivity of 86.8% in low-risk
CRT positive and NAAT negative, quantitative Ct bacterial load
women and 71% in high-risk women in the Philippines, reported
was detected in 2 samples and human HLA in 27 samples
earlier in a study supported by the manufacturer [12]. The
discrepancy might partly be explained by the use of a differentreference test. Where we used Gen-Probe’s Aptima platform as a
Quantitative Ct bacterial load was 73 times higher in NAAT-
reference test, in the Philippines study the Roche Amplicor (Roche
positive/CRT-positive samples (geometric mean 120 IFU) com-
Molecular Systems, Branchburg, NJ) was used. Although current
pared to NAAT-positive/CRT-negative samples (geometric mean
generation NAATs have comparable sensitivities, NAAT could be
1.64 IFU, p,0.001). Human DNA concentration did not differ
more sensitive than Roche Amplicor [15]. A somewhat lower
sensitivity of CRT in our study could be expected with a more
(p = 0.835). The average chlamydial/human cell load ratio (Ct
sensitive control test, but this does not explain the large difference
concentration) was 60 times higher in NAAT-positive samples
in sensitivity found in the Philippine study and our results.
that tested positive for CRT and NAAT, quantitative Ct bacterial
load was detected in all 42 samples and human HLA in 39samples. Of the 60 samples that tested CRT negative and NAAT
We found a disappointingly low clinical sensitivity of 42.0% and
positive, quantitative Ct bacterial load was detected in 55 samples
39.4% of the CRT in low-risk and high-risk Surinamese women,
and human HLA in all 60 samples. Of the 29 samples that tested
respectively, compared to the sensitivity of 86.8% in low-risk
CRT positive and NAAT negative, quantitative Ct bacterial load
women and 71% in high-risk women in the Philippines, reported
was detected in 2 samples and human HLA in 27 samples
earlier in a study supported by the manufacturer [12]. The
discrepancy might partly be explained by the use of a differentreference test. Where we used Gen-Probe’s Aptima platform as a
Quantitative Ct bacterial load was 73 times higher in NAAT-
reference test, in the Philippines study the Roche Amplicor (Roche
positive/CRT-positive samples (geometric mean 120 IFU) com-
Molecular Systems, Branchburg, NJ) was used. Although current
pared to NAAT-positive/CRT-negative samples (geometric mean
generation NAATs have comparable sensitivities, NAAT could be
1.64 IFU, p,0.001). Human DNA concentration did not differ
more sensitive than Roche Amplicor [15]. A somewhat lower
sensitivity of CRT in our study could be expected with a more
(p = 0.835). The average chlamydial/human cell load ratio (Ct
sensitive control test, but this does not explain the large difference
concentration) was 60 times higher in NAAT-positive samples
in sensitivity found in the Philippine study and our results. In the CRT evaluation study performed in the Philippines, the
commercially available products [10]. Still, with a sensitivity of
Ct prevalence was 6.3% in the low-risk group (women visiting an
only 41.7%, this test performs under the minimally required
obstetrics-gynaecology clinic) and 17.9 to 32% in the high-risk
sensitivity of 63% required for a POC test to treat more infected
group (female sex workers), which compares well with the
individuals than the standard NAAT in a setting with low patient
prevalences found in our study, 9.2% and 20.8% respectively.
In the CRT evaluation study performed in the Philippines, the
commercially available products [10]. Still, with a sensitivity of
Ct prevalence was 6.3% in the low-risk group (women visiting an
only 41.7%, this test performs under the minimally required
obstetrics-gynaecology clinic) and 17.9 to 32% in the high-risk
sensitivity of 63% required for a POC test to treat more infected
group (female sex workers), which compares well with the
individuals than the standard NAAT in a setting with low patient
prevalences found in our study, 9.2% and 20.8% respectively. 13. Michel CE, Solomon AW, Magbanua JP, Massae PA, Huang L, et al. (2006)
Chlamydia trachomatis in significantly more women by the APTIMA Combo 2
Field evaluation of a rapid point-of-care assay for targeting antibiotic treatment
assay. J Clin Microbiol 44: 400–405.
13. Michel CE, Solomon AW, Magbanua JP, Massae PA, Huang L, et al. (2006)
Chlamydia trachomatis in significantly more women by the APTIMA Combo 2
Field evaluation of a rapid point-of-care assay for targeting antibiotic treatment
assay. J Clin Microbiol 44: 400–405.