Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients levitra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Pii: s0015-0282(02)04216-4
FERTILITY AND STERILITY VOL. 78, NO. 5, NOVEMBER 2002Copyright 2002 American Society for Reproductive Medicine
Published by Elsevier Science Inc. Printed on acid-free paper in U.S.A. Consensus statement for the management of chronic pelvic pain and endometriosis: proceedings of an expert-panel consensus process Joseph C. Gambone, D.O., M.P.H.,a,b Brian S. Mittman, Ph.D.,b,cMalcolm G. Munro, M.D.,a Anthony R. Scialli, M.D.,d Craig A. Winkel, M.D., M.B.A.,dand the Chronic Pelvic Pain/Endometriosis Working GroupUCLA Medical School, Los Angeles, CaliforniaObjective: To develop recommendations for the medical and surgical care of women who present with chronic pelvic pain (CPP) and are likely to have endometriosis as the underlying cause. Design: An expert panel comprised of practicing gynecologists from throughout the United States and experts in consensus guideline development was convened. After completion of a structured literature search and creation of draft algorithms by an executive committee, the expert panel of Ͼ50 practicing gynecologists met for a 2-day consensus conference during which the clinical recommendations and algorithms were reviewed, refined, and then ratified by unanimous or near-unanimous votes. Patient(s): Women presenting with CPP who are likely to have endometriosis as the underlying cause. Main Outcome Measure(s): None. Conclusion(s): Chronic pelvic pain frequently occurs secondary to nongynecologic conditions that must be considered in the evaluation of affected women. For women in whom endometriosis is the suspected cause of the pain, laparoscopic confirmation of the diagnosis is unnecessary, and a trial of medical therapy, including
second-line therapies such as danazol, GnRH agonists, and progestins, is justified provided that there are no
other indications for surgery such as the presence of a suspicious adnexal mass. When surgery is necessary,
laparoscopic approaches seem to offer comparable clinical outcomes to those performed via laparotomy, but
with reduced morbidity. The balance of evidence supports the use of adjuvant postoperative medical therapy
after conservative surgery for CPP. There is some evidence that adjuvant presacral neurectomy adds benefit
for midline pain, but currently, there is inadequate evidence to support the use of uterosacral nerve ablation
or uterine suspension. Hysterectomy alone has undocumented value in the surgical management of women
with endometriosis-associated CPP. (Fertil Steril 2002;78:961–72. 2002 by American Society for Repro-
Key Words: Pain, endometriosis, guidelines, consensus
California 90095-1740(FAX: 310-206-3670; E-mail: jgambone@mednet. ucla.edu).
Chronic pelvic pain (CPP) and endometrio-
age of women with CPP who also have endo-
sis are two of the more common symptomatic
metriosis range as high as 70%–90% (3–5).
conditions in women’s healthcare. Ten percent
The natural history of endometriosis remains
Angeles, California. bDepartment of Veterans
of visits to gynecologists, 20% of laparoscopic
open to speculation because no prospective ob-
procedures performed by gynecologists, and
servational studies have been undertaken or
Յ18% of hysterectomies are performed for
reported. Although endometriosis has been ob-
CPP (1, 2). Chronic pelvic pain has multiple
served in females as young as 10.5 years, the
etiologies, and in many women a specific cause
disease usually presents during the reproduc-
may remain uncertain or unknown. Endometri-
tive years and is stable or regresses in 50% of
osis is a common cause of CPP. Currently there
women (6, 7), whereas in the remainder, pro-
exist no valid epidemiological data to establish
gression is generally slow. The type of CPP
the true incidence of endometriosis in women
most commonly attributed to endometriosis is
0015-0282/02/$22.00PII S0015-0282(02)04216-4
with CPP. However, estimates of the percent-
dysmenorrhea, but both cyclic and noncyclic
pain as well as deep dyspareunia and dyschesia are de-
The consensus panel met to review the evidence summa-
ries and draft materials during a 2-day consensus conference. The conference began with general sessions addressing con-
Evidence regarding the efficacy and other characteristics
sensus statement goals and methods, followed by individual
of available treatments, medical and surgical, for CPP and
subcommittee meetings to review and revise the draft mate-
endometriosis is incomplete. As a result, management of
rials. Ten consensus panel members were assigned by ran-
women with CPP thought to be secondary to endometriosis
dom drawing to each of three subcommittees which ad-
varies widely and may often be suboptimal and costly. These
dressed [1] diagnostic processes, [2] medical therapies, and
variations and opportunities for improvement, as well as the
[3] surgical therapies. Each subcommittee reviewed the rel-
availability of new evidence and changing opinions regard-
evant evidence summaries and draft algorithms and recom-
ing optimal management, suggest the potential value of an
mendations and revised the drafts after extensive discussion.
evidence-based consensus statement concerning the most
The subcommittee presented their revisions to the entire
appropriate care for these patients based on a combination of
panel in a subsequent plenary session, with ratifications by
expert opinion and a current literature review.
formal vote. All three subcommittees’ final algorithms and
Herein we describe the methodology and results of an
recommendation statements were approved by unanimous or
expert-panel consensus statement development process. The
available evidence for clinical management guidance is alsosummarized. The consensus recommendations and algo-
SUMMARY OF THE EVIDENCE
rithms do not address the additional diagnostic or treatmentsteps indicated in women for whom the presenting CPP
Herein we present the available evidence relevant to the
appears to have a cause other than endometriosis, or for
important areas of clinical management of CPP that occurs
whom other conditions (including pelvic masses) would
in association with endometriosis. Although some aspects of
necessarily complicate management. Similarly, the consen-
the diagnosis and treatment of CPP have been studied ex-
sus statement does not address treatment for infertility asso-
tensively, well-designed studies regarding other important
ciated with endometriosis and provides only partial guidance
aspects have not been reported or were not found during this
for women with CPP that is believed to be secondary to
endometriosis (whether or not infertility is demonstrated orsuspected), for whom immediate fertility is a primary goal. Medical Therapy Nonsteroidal Anti-Inflammatory Drugs CONSENSUS STATEMENT DEVELOPMENT METHODS
Nonsteroidal anti-inflammatory drugs (NSAIDs) have
been studied extensively in randomized controlled trials
The consensus statement (comprising clinical recommen-
(RCTs) for treatment of primary dysmenorrhea and are of
dations and algorithms) was developed by a panel of 52
proven efficacy (11–16). Although not specifically studied
practicing gynecologists and methodology experts according
for noncyclic CPP, it is apparent that NSAIDs are used
to accepted standards for development of clinical practice
empirically as a first-line medical treatment for CPP.
guidelines and consensus statements (8 –10). Panel members
Oral Contraceptives
were selected by a consensus statement executive committee(CSEC), based on practice credentials and geographic loca-
High-dose estrogen–progestin combinations were initially
tion. The development process included a MEDLINE liter-
employed as part of a “pseudopregnancy regimen” in the
ature search for articles addressing etiology and pathophys-
management of symptomatic endometriosis (17). Various
low-dose oral contraceptives (OCs) have been studied with-
endometriosis. The initial search covered the period 1966
out placebo controls as initial management of primary dys-
through August, 1999 and was updated through December,
menorrhea with a high degree of success (18 –20). These
2001. The article list was reviewed by four pairs of reviewers
studies included patients not screened by laparoscopy, sug-
(comprising the CSEC), focusing on [1] epidemiology of
gesting the possibility that patients with CPP and endome-
CPP, [2] etiology, pathophysiology and impact of endome-
triosis on CPP, [3] medical therapy for endometriosis and
Only a single RCT of low-dose OCs for CPP and endo-
CPP, and [4] surgical therapy for endometriosis and CPP.
metriosis has been published (21). In this 6-month trial,
The CSEC reviewed and summarized all relevant articles
cyclically administered OCs were compared with a GnRH
in a series of 5- to 10-page evidence summaries. The CSEC
agonist (GnRH-a) in women with laparoscopically diag-
then developed preliminary diagnostic and treatment algo-
nosed endometriosis. Oral contraceptives were reported to be
rithms, and the summaries and initial clinical recommenda-
less effective for relief of dysmenorrhea and to be of similar
tions were distributed to the consensus panel members in
efficacy to GnRH-a for relief of dyspareunia and nonmen-
Gambone et al. Danazol
ease, and vasomotor symptoms were all suppressed withoutsignificant change in bone density in either group. Hornstein
Danazol is a synthetic androgen that inhibits ovarian
et al. (50) reported 201 patients treated with depot leuprolide
steroid and pituitary gonadotropin release (22). A group of
acetate for 52 weeks and randomized into one of four add-
four 6-month RCTs (with possible patient overlap) com-
back groups. Groups received placebo, norethindrone acetate
pared danazol with placebo after laparoscopic diagnosis of
(5 mg/d) alone, or norethindrone acetate (5 mg/d) in con-
endometriosis in which danazol was more effective than
junction with conjugated equine estrogens (0.625 or 1.25
placebo (23–26). One of these studies also reported a sig-
mg/d). Pain symptoms were alleviated in each treatment
nificant improvement in painful symptoms after treatment
arm, although the highest number of dropouts due to persis-
with danazol compared with placebo in patients who had not
tent or recurrent pain was noted in those receiving the higher
undergone surgery (24). No other studies were found that
estrogen doses. Vasomotor symptoms were suppressed in all
reported the use of danazol in the management of CPP or
three add-back groups. Lumbar spine bone mineral density
dysmenorrhea or in patients with clinically suspected endo-
decreased 3.2% in 6 months and 6.3% in 12 months without
add-back, but no significant decrease was observed in any of
Gonadotropin-releasing Hormone Agonist
the add-back groups. Adverse lipid changes shown withdanazol and GnRH-a consist of decreased high-density li-
Gonadotropin-releasing hormone agonist effectively in-
poprotein (HDL) cholesterol and increased total and low-
duces a “functional oophorectomy” in treated patients,
density lipoprotein (LDL) cholesterol, with greater adverse
thereby dramatically reducing estradiol production. Only one
effects of danazol than those of GnRH-a on lipids (32, 51).
published RCT compared a GnRH-a (leuprolide acetate) to
Add-back with norethindrone acetate with or without low-
placebo (27). Because most (27 of 31) placebo patients
dose or high-dose equine estrogen resulted in increased HDL
dropped out by 3 months because of symptoms, valid scien-
and decreased LDL cholesterol (50). The mechanism of
tific comparisons could not be made between the groups.
action is unclear but may be related, in part, to hepatic
Nevertheless, a substantial degree of pain relief was demon-
conversion of small but clinically significant amounts of
norethindrone acetate to ethinyl estradiol.
The majority of studies compared GnRH-a with danazol
Progestins
(400 – 800 mg/d) administered to women with laparoscopi-cally confirmed symptomatic endometriosis. A large group
Medroxyprogesterone acetate (MPA) may be beneficial
of studies demonstrated the danazol and GnRH-a treatment
for patients with CPP secondary to known or suspected
regimens to be equally efficacious (28 – 42).
endometriosis. Progestins induce decidualization and acy-
Empiric use of GnRH-a was tested by RCT in 100 women
clicity of endometrium and endometriotic tissue. One review
with noncyclic pelvic pain who had not undergone assess-
article by Vercellini et al. (52) analyzed 27 trials of various
ment by laparoscopy but nevertheless had clinically sus-
progestins for treatment of symptomatic endometriosis, four
pected endometriosis (5). After 12 weeks of therapy with
of which were RCTs (21, 53–55). Variously, progestins were
depot leuprolide acetate (3.75 mg/mo), decreases in dysmen-
compared with danazol (23), with danazol and an OC (24),
orrhea, pelvic pain, and tenderness were noted in the treat-
with a depot preparation of a GnRH-a (21), and with placebo
ment group. Endometriosis was visualized at subsequent
(25). Dydrogesterone (2 different doses) was found to be no
laparoscopy in 78% of the leuprolide-treated and 87% of the
more effective than placebo. In one 12-month trial, MPA
placebo-treated groups. Women who did not present visual
depot (150 mg every 90 days) used alone had effects equiv-
evidence of endometriosis, however, also responded to treat-
alent to those of GnRH-a. In two 6-month trials, the proges-
tins desogestrel (56) or cyproterone acetate (57) were com-bined with ethinyl estradiol. Overall, odds ratios (OR) for
Steroidal and nonsteroidal agents have been employed in
these two non–placebo-controlled randomized trials varied
the context of add-back regimens to allow maintenance of
from 0.3 to 2.5, with a common nonsignificant OR of 1.1
the function and efficacy of the GnRH-a while suppressing
(confidence interval [95% CI] ϭ 0.4 –3.1). Oral MPA in a
side effects such as osteopenia and vasomotor symptoms. A
50-mg daily dose was effective in reducing pain scores at the
number of RCTs have demonstrated the efficacy of add-back
end of therapy, but the benefit was not sustained (58).
regimens with various GnRH-a for treatment of endometri-osis during 6-month courses (43– 48). Medical Adjunctive Therapy
Two RCTs have assessed the role of add-back with depot
Many of the agents reviewed above can be used before,
leuprolide acetate (depot GnRH-a) during therapy for Ͼ6
after, or both before and after either conservative or radical
months (49, 50). In an open-label trial of 19 patients who
surgery. Adamson and Nelson (59) suggested that preoper-
received GnRH-a with either norethindrone (10 mg/d p.o.) or
ative medical therapy may result in less risk of injury to
norethindrone (2.5 mg/d) ϩ cyclic etidronate (400 mg/d)
ureters, blood vessels, and the bowel, although none of these
during a 48-week trial (49), pain symptoms, extent of dis-
potential benefits have been proved. FERTILITY & STERILITY
Danazol has been evaluated as postoperative adjuvant
diagnostic laparoscopy alone for stage I–III endometriosis-
therapy in three randomized trials (60 – 62). A dose of 600
associated CPP. Ninety percent of those with improvement
mg/d for 6 months after surgery was found to be equivalent
at 6 months continued to demonstrate improvement at 1 year.
to 100 mg/d of MPA and to be superior to placebo although
Unfortunately, the addition of uterosacral nerve ablation to
side effects occurred, including bleeding, weight gain, and
the surgical procedure confounded interpretation of the ef-
acne (60). A randomized trial to compare a similar dose of
ficacy of endometriosis destruction alone in producing pain
danazol with no therapy (no placebo) for 3 postoperative
relief. However, investigators from the same center per-
months demonstrated no advantage with respect to pain
formed a subsequent double-blind RCT in which all women
recurrence (61). Morgante et al. (62) evaluated low-dose
underwent laparoscopic laser vaporization of endometriosis;
danazol (100 mg/d) in a cohort of women who underwent
half of the women were randomized to receive uterosacral
conservative laparoscopic surgery and 6 months of GnRH-a
nerve ablation as well (69). At 6 months of follow-up, all
therapy (62). The danazol group had lower pain scores than
patients in the trial were significantly improved compared
did those patients who did not use danazol after the postop-
with baseline, but those with vaporization alone had pain
scores that were similar to or better than those of womenwho underwent vaporization and uterosacral nerve ablation.
Despite the existence of RCTs evaluating the issue, there
These findings suggest that local destruction of endometri-
is controversy regarding the value of GnRH-a after conser-
otic lesions is associated with improvements in pelvic pain,
vative surgical therapy. An Italian group compared 3 months
at least at 6 to 12 months after surgery.
of postoperative nafarelin (400 g/day) with placebo nasalspray and found no difference in pain scores at 12 months
Surgery Directed at Endometriosis: Type of Treatment
(63). A larger Italian multicenter RCT of 269 patients, how-ever, has shown that adjuvant GnRH-a therapy was effica-
There are a number of techniques by which endometriosis
cious at 6 months after conservative surgery but failed at 1 to
can be removed or destroyed, and each has potential advan-
tages, disadvantages, and differences in efficacy. However,no RCTs were found that compare surgical excision with
In a third RCT that was done in the United States,
energy-based ablation techniques that include vaporization,
investigators found that women treated with a GnRH-a had
fulguration, or coagulation. Winkel and Bray (67) reported a
better outcomes than women treated with surgery alone (65).
24-month follow-up of women who underwent surgical
Winkel and Bray (66) recently reported the results of a
treatment by excision alone, laser vaporization alone, or
24-month follow-up of 240 women with endometriosis and
laser vaporization plus GnRH-a. Twelve months after sur-
CPP who underwent excision alone, laser ablation alone, or
gery, 96% of excision patients were pain free, whereas 69%
laser ablation followed by treatment with leuprolide acetate
of those undergoing coagulation were without pain. At 2
for 3 to 6 months. In this nonrandomized trial, only 23% of
years, the corresponding figures were 69% and 23%, respec-
the ablation group was pain free at 24 months, whereas 70%
tively. Although these results suggest that excision may be
of the ablation plus GnRH-a–treated group remained pain
superior to ablation, the retrospective design of the study
leaves such a conclusion open to criticism. Surgical Therapy Management of Endometriosis-associated Cystic Ovarian
Evaluation of the treatment effect of surgery on endo-
Masses
metriosis-associated pain is difficult because few RCTs havebeen performed and none have compared surgical manage-
There exist a number of approaches to the surgical man-
agement of ovarian cysts encountered in the treatment ofendometriosis, including cystectomy, simple drainage, drain-
Surgery Directed at Endometriosis: Overview
age and coagulation, and drainage followed by stripping ofthe cyst lining. Not all ovarian cysts associated with endo-
Sutton (67) reported that 70% of women treated for
metriosis are endometriomas (in one study, none of the
endometriosis with laparoscopically directed techniques
excised cysts or cyst linings contained histologically dem-
were improved at 1 year. Redwine (68) reported a cumula-
onstrated endometriosis) (70). In another retrospective study,
tive rate of recurrence and persistence (defined as visualizing
however, the authors compared outcomes in 231 women
endometriosis at repeat laparoscopy without regard to symp-
managed laparoscopically either with fenestration and abla-
toms) of 19% by 5 years. Both uncontrolled studies em-
tion (n ϭ 70) or by cystectomy (n ϭ 161) (71). Reoperation
ployed retrospective data collection, inconsistent approaches
rates at 42 months were 23.5% after excision and 57.8% after
to the measurement of symptoms, and heterogeneity of sur-
fenestration and ablation. Somewhat similar results were
reported by Beretta et al. (72), who performed an RCT
In a double-blind RCT, Sutton et al. (69) reported the
comparing cystectomy with drainage and bipolar electrosur-
results of laparoscopically directed conservative surgery (la-
gical coagulation of the lining in 64 women operated on via
ser vaporization, adhesiolysis, uterosacral nerve ablation) vs.
laparoscopy. Although complication rates were similar, there
Gambone et al.
were significantly different outcomes in favor of cystectomy
results at laparotomy. Although Candiani et al. (78) found
for each of the three types of pain evaluated, including
that adding PSN to conservative surgery markedly reduced
dysmenorrhea (15.8% vs. 52.9%), deep dyspareunia (20%
the midline component of menstrual pain, in long-term fol-
vs. 75%), and nonmenstrual pain (10% vs. 52.9%).
low-up, there were no differences between the two groups inthe frequency and severity of dysmenorrhea, pelvic pain, and
Laparoscopy vs. Laparotomy
dyspareunia. Tjaden et al. (79) also found that the addition of
The literature is replete only with comparisons of laparo-
PSN to standard surgical therapy by laparotomy enhanced
scopic and laparotomic surgery that include AFS stage IV
pain relief for midline pain. Although this was reported as an
endometriosis. Crosignani et al. (73) evaluated women with
RCT, only 8 of 26 patients were randomized, and the study
CPP and stage IV endometriosis after laparoscopic surgery
was terminated before completion because of significant
(n ϭ 47) or at the time of laparotomy (n ϭ 108) surgery
reduction in midline pain experienced by the patients under-
selected by the surgeon. Many of the women also received
going PSN. Chen et al. (80) reported the only RCT evaluat-
medical therapy after surgery. At 24 months, the laparo-
ing laparoscopic PSN in 68 patients assigned to either PSN
scopic and laparotomy approaches were about equally effec-
or LUNA. These patients had primary dysmenorrhea and
tive (approximately two thirds of patients were pain free).
were not known to have endometriosis. At 3-month follow-
Recurrence rates for dysmenorrhea were 16.4% to 20.3% for
up, both groups were equal in terms of symptom relief
laparoscopic surgery vs. 20.3% to 27.7% for those per-
(87.9% vs. 82.9%), but the efficacy of PSN was significantly
formed via laparotomy; 28.6% to 33.3% for deep dyspareu-
better than that of LUNA (81.8% vs. 51.4%) at 12 months.
nia for laparoscopy vs. 10.4% to 15.4% for dyspareunia; and
Role of Gonadectomy and Hysterectomy
17.5% to 25% vs. 15.9% to 20.1% for nonmenstrual CPP.
Conservative surgery at laparotomy was compared with
Removal of the ovaries (bilateral oophorectomy), with or
the laparoscopic approach in 81 patients who required repeat
without hysterectomy, is generally regarded as the most
surgery for endometriosis (AFS stages I–IV) (74). They were
effective procedure for women who have recurrent symp-
similar with respect to recurrence rates for dysmenorrhea
tomatic endometriosis and who have no desire to retain
(28.6% vs. 25%), dyspareunia (25% vs. 30%), and noncyclic
reproductive function. A number of investigators have eval-
CPP (23% vs. 34%). Similar results were reported in 132
uated the incidence of symptom recurrence after hysterec-
women with stage III and IV endometriosis who also were
tomy with ovarian retention. One group demonstrated that 18
of 29 women experienced recurrent pain and 9 (31%) un-derwent reoperation after hysterectomy with ovarian reten-
The incidence of pain recurrence was 19% after lapa-
tion (81). Retained ovarian function had an 8.1 OR (CI ϭ
rotomic surgery and 13.4% after laparoscopy in a retrospec-
2.1–31.3) of requiring reoperation for CPP. The incidence of
tive study with 12-month follow-up done by Bateman et al.
persistent or recurrent CPP after hysterectomy and bilateral
(76). Laparoscopic technique was associated with equivalent
salpingo-oophorectomy was 10% (11 of 109).
operating time, reduced hospital stay, and a more rapidreturn to work. Uterine Suspension Procedures Surgery Directed at Pain Transmission
The consensus group could find no data supporting or
refuting the place for uterine suspension as an adjunct in the
Uterosacral Nerve Ablation. Laparoscopic uterosacral
treatment of endometriosis-associated pelvic pain. Individual
nerve ablation (LUNA) is designed to disrupt the efferent
practitioner experience can guide the use of this procedure.
nerve fibers in the uterosacral ligament to diminish uterinepain. However, there seems to be little evidence to support
CLINICAL RECOMMENDATIONS AND
the performance of this procedure. In a cohort study, Lichten
ALGORITHMS
and Bombard (77) reported Ͼ80% relief from menstrualpain after LUNA that declined to 50% after 12 months. The
The overall algorithm produced and approved by the
double-blind RCT reported by Sutton et al. (69), discussed
consensus panel (Fig. 1) provides a general guide for the
previously, showed that adding LUNA to laser vaporization
assessment and management of women presenting with CPP.
of endometriosis did not improve pain scores. In fact, in this
Subalgorithms were created for sections A and E of the
well-designed double-blinded trial, patients who had LUNA
overall algorithm, as discussed below.
added to the procedure had less successful 6-month out-
Section A (seen in detail in Fig. 2) addresses the diag-
comes with respect to both dysmenorrhea and chronic non-
nostic approach to women with CPP, including an assess-
ment of patient preferences and values, leading to an initial
Presacral Neurectomy. Presacral neurectomy (PSN) is a
diagnostic impression. Significantly, this algorithm identifies
procedure designed to interrupt sympathetic pathways from
women who may have CPP secondary to diagnoses other
the uterus. There have been three reported RCTs, one eval-
than endometriosis (section B). Management of these clini-
uating PSN as performed via laparoscopy and two that assess
cal entities, although extremely important, was not consid-
FERTILITY & STERILITY
Algorithm that delineates the steps for the assessment, diagnosis, and treatment options of patients with chronic pelvic painand presumed endometriosis: overall approach. Gambone. Chronic pelvic pain and endometriosis. Fertil Steril 2002.
ered to be within the purview of this expert panel and
triosis, GI or GU problems, infections, musculoskeletal
therefore was not developed further. Sections C through I
problems, and psychiatric conditions, including infor-
address management of the target group for the consensus
mation on response to any previous treatments for en-
statement. A detailed algorithm is provided for section E in
dometriosis or other conditions related to the presenting
Section A: Initial Diagnosis and Assessment
● Previous symptoms suspicious for endometriosis, GI or
GU problems, infections, musculoskeletal problems,
Clinical History
psychological or psychiatric conditions, sexual abuse,or physical abuse
A thorough history of the woman’s symptoms, and pre-
● Menstrual, contraceptive, and sexual histories, in-
vious diagnoses and treatments should include, but should
cluding previous menstrual disorders; use of intra-
uterine devices, OCs, and other contraceptive meth-
● The presenting pain, including its location, magnitude,
ods; age of onset of menses; a history of all
timing, relationship to physical exertion, sexual activity,
pregnancy outcomes; and other reproductive tract–
menses, pregnancy, abdominal distention, gastrointesti-
nal (GI) and genitourinary (GU) function, as well as
● Family history of relevant clinical conditions, includ-
ing malignancies and pain disorders such as endome-
● Prior and current diagnoses and treatments for endome-
Gambone et al.
● Blood tests, including complete blood count with dif-
ferential and erythrocyte sedimentation rate
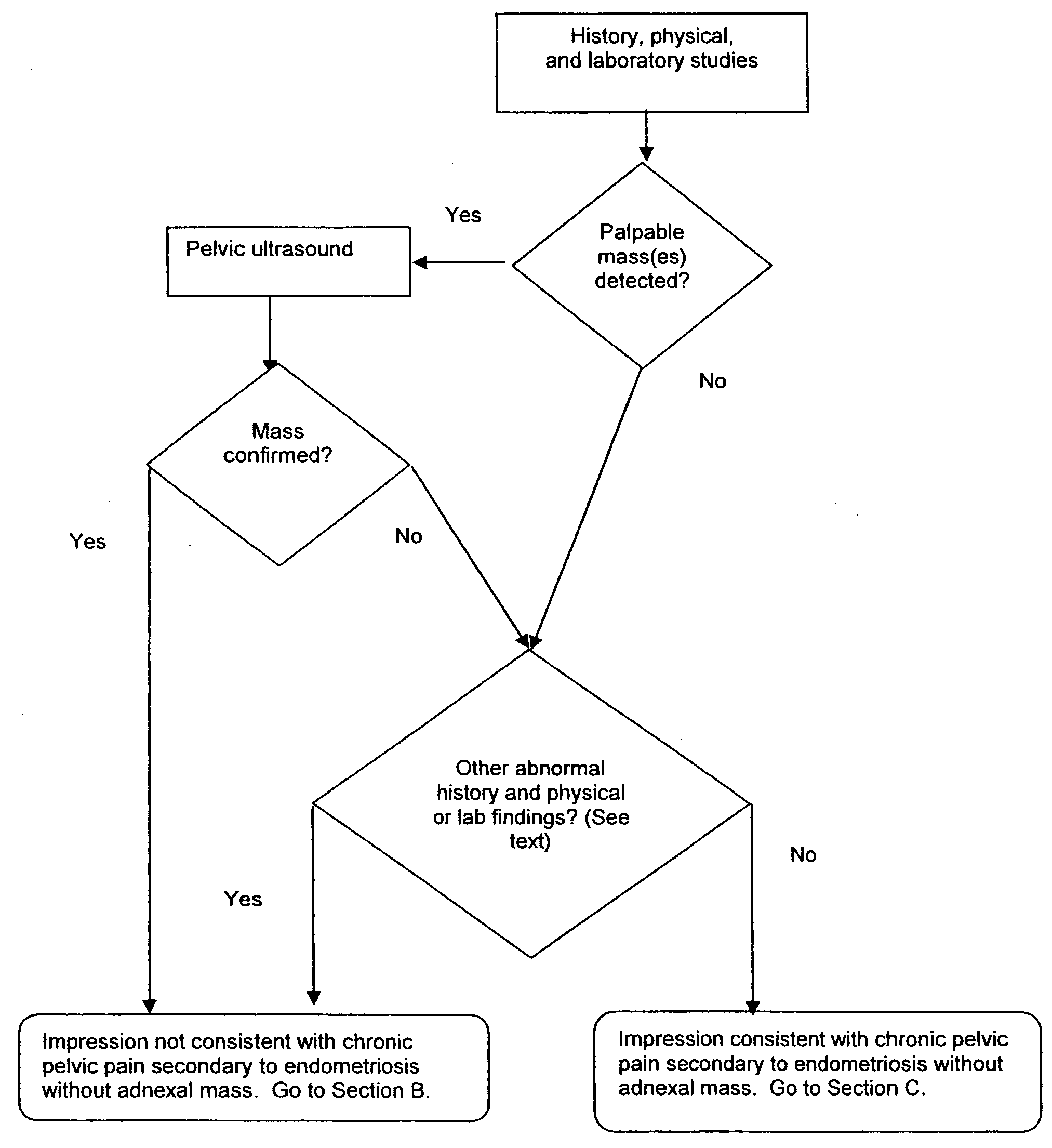
Closer view of section A of overall algorithm shown in Figure
● CA-125 (in selected cases, e.g., evidence of ascites)
1: initial assessment of patients with chronic pelvic pain andpresumed endometriosis.
● Pelvic ultrasound (if a mass is palpated)● Magnetic resonance imaging (in selected cases, e.g., if
it is necessary to identify deep infiltrative disease pre-operatively, although the accuracy of magnetic reso-nance imaging for this diagnosis is controversial)
Patient Preferences and Values
A thorough discussion and assessment of the patient’s
preferences and values should be conducted, addressing hernear-term and long-term plans and desires regarding fertility,her attitudes and preferences regarding medical and surgicaltreatments, and other relevant issues. Development of the Initial Impression
On the basis of the history, physical examination, labo-
ratory, and any indicated imaging studies, an initial impres-sion should be developed. If one or more findings are con-sistent with a condition other than endometriosis withoutadnexal mass, then further diagnostic testing and/or treat-ment should be conducted, as appropriate (see section B ofthe algorithm). If no findings are consistent with anothergynecologic or nongynecologic diagnosis, then endometrio-sis should be strongly suspected, and first-line medical ther-apy should be considered. Section B: Nongynecologic Causes Gambone. Chronic pelvic pain and endometriosis. Fertil Steril 2002.
When a patient’s CPP is thought to be due to nongyne-
cological conditions such as irritable bowel syndrome or
Physical Examination
urologic problems such as chronic cystitis or is associatedwith psychological problems secondary to physical or sexual
A complete gynecologic and targeted physical examina-
abuse, an appropriate workup for these nongynecologic con-
tion should be conducted considering both potential gyneco-
ditions is recommended. Details about specific interventions
logic and nongynecologic causes of the pain as well as the
for nongynecologic conditions or management of women
concepts of referred pain and the existence of trigger points.
who have adnexal masses were beyond the scope of this
Specifically, it should include the following:
● Pelvic exam, focusing on tenderness and its location,
Section C: First-Line Medical Treatment
the presence or absence of nodularity, particularly in the
Medical treatment of women with CPP suspected to be
cul-de-sac, and the detection of palpable masses also in
related to endometriosis should begin with a trial of NSAIDs
or OCs or a combination of both. Selection of a first-line
● Abdominal exam, focusing on the presence or absence
medical therapeutic agent should be based on the nature of
of abdominal distention and the location of the symp-
the pain (cyclic or noncyclic), contraindications to NSAIDs
or OCs (including a history of GI problems), desire for
● Straight leg–raising test, focusing on its ability to in-
contraception, and other factors. Nonsteroidal anti-inflam-
duce lower right or left quadrant tenderness
matory drugs should be used around the time of menses in
Laboratory and Imaging Studies
women with cyclic pain, intermittently for those with inter-mittent cyclic pain, or continuously, based on the patient’s
Appropriate laboratory tests and imaging studies can be
symptoms or response to initial therapy. If adequate pain
conducted to evaluate for nongynecological causes of CPP
relief is obtained from NSAIDs or OCs (individually or in
and, if endometriosis is present, to assess the extent of the
combination), then a maintenance management regimen
disease. These tests and studies are as follows:
should be considered (see section H of the algorithm).
If the initial medical therapy fails to relieve the pain
FERTILITY & STERILITY
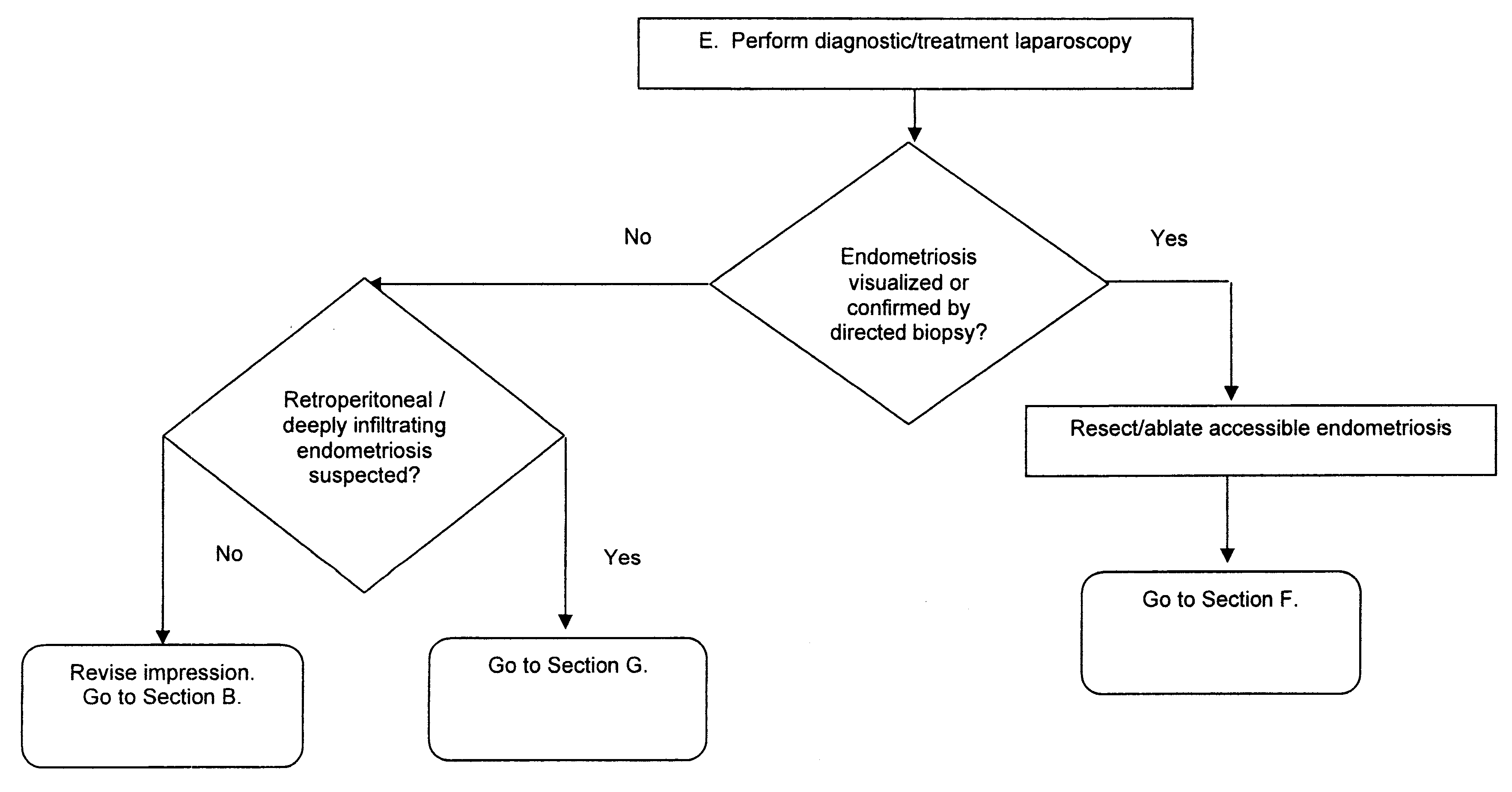
Closer view of section E of overall algorithm shown in Figure 1: laparoscopic diagnosis and conservative treatment ofendometriosis. Gambone. Chronic pelvic pain and endometriosis. Fertil Steril 2002.
symptoms, then a trial of a second-line treatment should be
directed excision, ablation, or both should be strongly con-
considered (see section D of the algorithm).
sidered provided that the operator is adequately experienced. The location and/or extent of disease in combination with the
Section D: Options for Second-Line
patient’s desires regarding future fertility are important con-
Treatment
siderations. Patients with dysmenorrhea who have not re-
If first-line medical therapy fails, there are two therapeu-
sponded to medical therapy may be offered PSN at laparot-
tic options to consider. First, a trial of advanced medical
omy or, if the operator is adequately experienced, via
therapy should be considered (see section G of the algo-
laparoscopy. Available evidence suggests that LUNA does
rithm). Alternately, an operative procedure such as laparos-
not benefit women with CPP associated with endometriosis.
copy or laparotomy may be considered (see section E of thealgorithm). Considerations relevant to the selection of one of
Section F: Adjunctive Medical Treatment
these treatment options include the following:
Adjunctive medical therapy should be provided to women
after conservative surgical treatment for endometriosis and
● Several available second-line medical treatments are
may consist of danazol, GnRH-a, or progestins, based on
effective and are relatively free of serious complica-
individual response to previous trials of medical therapy,
patient preference, and other factors. There is no published
● Laparoscopy and other surgical procedures may be less
evidence supporting OCs as an adjunctive medical treatment,
effective than medical therapies and are reported to
although a trial and continuation when effective seems rea-
entail greater cost and surgical complication rates (re-
● Patient preferences, cost, effect on future fertility, and
Section G: Advanced Medical Therapy
the possibility and consequences of a false presumptive
Advanced medical treatment instead of surgery is recom-
diagnosis should always be taken into account.
mended for women with CPP that has not responded to
Section E: Operative Diagnosis and
NSAIDs or OCs or for whom these agents are contraindi-
Conservative Surgical Treatment
If patients with CPP undergo diagnostic laparoscopy and
Unless contraindicated, advanced medical therapy should
endometriosis is identified and thought to cause or contribute
begin with a 2-month trial of full-dose danazol, GnRH-a, or
to the pain, conservative treatment with laparoscopically
a progestin such as MPA and continued for 6 months or
Gambone et al.
longer if relief is obtained. If a GnRH-a is selected, an
remain significant gaps in the body of evidence available for
appropriate add-back regimen should be considered (unless
many important clinical problems, a situation that continues
contraindicated) to minimize treatment side effects.
to make the opinions of panels of experts a necessary and
When side effects or other considerations preclude a
essential part of clinical decision making (84). This meth-
complete trial of danazol, GnRH-a or MPA, or if all such
odology combines a search for the best evidence in conjunc-
agents are contraindicated, then surgical evaluation should
tion with a formal opinion-based process to gain consensus
when available evidence does not provide specific guidance.
Chronic pelvic pain is a common clinical complaint that
If adequate pain relief is not obtained from a complete
is responsible for 40% of laparoscopies and 6%–18% of
trial of an advanced medical therapy, then alternative diag-
hysterectomies, either alone or in combination with other
noses should be considered (section B above).
indications. There is evidence that a substantial proportion of
If adequate pain relief is obtained from the selected agent,
women with CPP have nongynecologic causes for their
then an appropriate maintenance management regimen
symptoms (85) and that Յ50% have a history of current or
should be initiated (section H below), keeping in mind that
previous physical or sexual abuse (86 – 88). Endometriosis is
pain often has multiple causes and may recur, requiring
a histologic diagnosis frequently associated with pain, in-
reevaluation and treatment revisions.
cluding CPP. The literature is not consistent regarding the
Section H: Surveillance and Medical
link between visualized endometriosis (the basis of AFS
Maintenance
staging) and CPP. Clearly, endometriosis can be asymptom-atic, and women with CPP may harbor asymptomatic endo-
Maintenance, after acute treatment, should include peri-
metriosis together with other causes for their symptoms. This
odic monitoring for return of symptoms, continuing treat-
may be one explanation for therapeutic failure or recurrence,
ment with NSAIDs or OCs, or continuing treatment with
including the persistence of CPP in Յ10% of women who
second-line medical therapies such as danazol, GnRH-a, or
have had a hysterectomy and bilateral salpingo-oopherec-
tomy (89, 90). Consequently, it is incumbent on the clinician
Selection of appropriate maintenance management should
to consider the potential for entities other than endometriosis
be based on the history of symptoms, treatment effective-
ness, and patient preference, as follows:
Many women with CPP have normal pelvic exams, and
● Women who obtain adequate relief from NSAIDs or
many have findings consistent with endometriosis. There
OCs but for whom symptoms return upon completion or
have been no published clinical trials that have compared
cessation of medical treatment should be maintained on
directly surgical and medical therapy for CPP and endome-
the therapeutic regimen that previously produced relief.
triosis. On the basis of the results of the current review, they
● Women who obtain relief from advanced medical ther-
could be considered equally effective, however. Conse-
apies but for whom symptoms return upon reversion to
quently, the consensus panel supported the notion of primary
NSAIDs or OCs should be considered for long-term
medical therapy for women with CPP that is suspected to be
treatment with advanced medical therapies.
related to endometriosis. Should this therapy fail, a trial of
● Women who obtain relief from laparoscopic resection
advanced medical therapy with danazol, GnRH-a, or contin-
and/or ablation should be considered for continuation
uous progestins is considered an appropriate option without
treatment with NSAIDs or OCs or with advanced med-
prior laparoscopy. However, when a pelvic or adnexal mass
is detected, operative evaluation or surgical exploration isrecommended because of the possibility of neoplasia. Section I: Nonconservative Surgical Therapy
Bilateral salpingo-oophorectomy, with or without hyster-
For women in whom surgery is performed, the nature of
ectomy, should be reserved for women who have completed
the procedure should be individualized and tailored to the
their child bearing and who realize the potential impact of
desires of the patient regarding future fertility, the location
castration on other health parameters such as risk of osteo-
and extent of disease, and the experience and expertise of the
porosis, sexual dysfunction, and other menopausal issues.
surgeon. It is clear that successful surgical results may be
Hysterectomy alone has little or no place in the management
temporary and that the use of postoperative adjuvant medical
of women who have CPP secondary to endometriosis alone.
therapy appears to reduce or delay the return of CPP. Al-though there is some evidence that presacral neurectomyprovides relief of midline pain in women with endometriosis,
DISCUSSION
available evidence suggests that uterosacral ablation is not
A substantial portion of current medical and surgical
effective. We were unable to find evidence that adjuvant
practice is primarily opinion based. Opinions underlying
uterine suspension has undergone critical evaluation.
clinical decision-making are not always based on the best
For women who have no desire for future fertility and
currently available evidence (82, 83). Nevertheless, there
who are willing to deal with the risks of surgical menopause,
FERTILITY & STERILITY
bilateral oophorectomy, with or without hysterectomy, has
lewski, M.D.; Eureka, California: Depak Stokes, M.D.; Salt Lake City,
been shown to relieve symptoms, provided that endometri-
Utah: Mark Stowers, M.D.; Englewood, Colorado: Eric S. Surrey, M.D.;Fullerton, California: Jerry Thanos, M.D.; Eugene, Oregon: Eldad Vered,
osis is the cause of the CPP or at least is a significant
M.D.; Beaumont, Texas: Ruben Victores, M.D.
Finally, we demonstrated the use of a formal consensus
development process in facilitating the critical review andinterpretation of a body of evidence by a panel of practicinggynecologists. Funding support disclosure: Partial funding was provided by an unre-
This process and the participation of a large panel of
stricted grant from the International Center for Postgraduate Medical Edu-
practicing gynecologists differed from other consensus de-
cation (ICPMED), formerly Medical Education Collaborative (MEC), an
velopment processes, which often rely on a much smaller
independent non-profit medical education provider. ICPMED’s program-
group of academic experts, with far less geographic and
ming is partially supported by TAP Pharmaceuticals. ICPMED providedlogistical and administrative support for the consensus conference and
practice-setting diversity and representation. Although the
evidence review. No ICPMED or TAP representatives played any substan-
advanced preparation and initial formulation of consensus
tive role in the development, review or reporting of the consensus statement
statements were performed by a smaller executive commit-
tee (CSEC), thereby limiting the breadth of opinion, sub-stantial changes were made by the larger panel during a
References
3-day conference. The consensus statement resulting from
1. Reiter RC. A profile of women with chronic pelvic pain. Clin Obstet
this process may be more acceptable to physicians in diverse
2. Gambone JC, Reiter RC, Slesinski MJ, Reiter RC, Moore JG. Valida-
community-based practice settings, given the central role
tion of hysterectomy indications and the quality assurance process.
that such physicians played in the statement’s final develop-
3. Koninckx PR, Meuleman C, Demeyere S, Lesaffre E, Cornillie FJ.
Suggestive evidence that pelvic endometriosis is a progressive disease,whereas deeply infiltrating endometriosis is associated with pelvic pain. Fertil Steril 1991;55:759 – 65.
4. Carter JE. Combined hysteroscopic and laparoscopic findings in pa-
tients with chronic pelvic pain. J Am Assoc Gynecol Laparosc 1994;2:43–7.
5. Ling F, Pelvic Pain Study Group. Randomized controlled trial of depot
leuprolide in patients with chronic pelvic pain and clinically suspectedendometriosis. Obstet Gynecol 1999;93:51– 8. Acknowledgments: The following individuals are members of the Chronic
6. Wardle P, Hull MGR. Is endometriosis a disease? Bailleres Clin Obstet
Pelvic Pain/Endometriosis Working Group: Mobile, Alabama: Oscar
7. Thomas EJ. Endometriosis, 1995— confusion or sense? Int J Obstet
Almeida, Jr., M.D.; Chula Vista, California: Eugene Basilere, M.D.; Edina,
Minnesota: Edward Beadle, M.D.; Raleigh, North Carolina: Pouru Bhiwan-
8. American Medical Association, Office of Quality Assurance. Attributes
diwalla, M.D.; Kansas City, Kansas: Henry Bishop, M.D.; Bend, Oregon:
to guide the development and evaluation of practice parameters. Chi-
Tammy Bull, M.D.; Tulsa, Oklahoma: Clark Bundren, M.D.; Fort Wayne,
cago, IL: American Medical Association, 1990.
9. Woolf SH. Manual for clinical practice guideline development. Rock-
Indiana: Steven Coats, M.D.; East Amherst, New York: Ivan D’Souza,
ville, MD: Agency for Health Care Policy and Research, 1991. AHCPR
M.D.; Knoxville, Tennessee: Michael Doody, M.D.; Anaheim Hills, Cali-
fornia: Janis Fee, M.D.; Missoula, Montana: J. Paul Ferguson, M.D.; Baylor
10. Grimshaw JM, Freemantle N, Wallace S. Developing and implement-
College of Medicine, Houston, Texas: Joseph R. Feste, M.D.; Tucson,
ing clinical practice guidelines. Qual Health Care 1995;4:55– 64.
11. Hamann GO. Severe primary dysmenorrhea treated with naproxen. A
Arizona: Timothy Gelety, M.D.; Waterville, Maine: Bill George, M.D.;
prospective, double-blind crossover investigation. Prostaglandins 1980;
Flossmore, Illinois: James Goldstone, M.D.; Brockton, Massachusetts: So-
heil Hanjani, M.D.; Baltimore, Maryland: Dwight Im, M.D.; South Euclid,
12. Hanson FW, Izu A, Henzl MR. Naproxen sodium, ibuprofen and a
Ohio: Thomas Janicki, M.D.; Brighton, Colorado: Amy Johnson, M.D.;
placebo in dysmenorrhea. Its influence in allowing continuation ofwork/school activities. Obstet Gynecol 1978;52:583–7.
Brooklyn, New York: Leslie Kernisant, M.D.; Boise, Idaho: Anthony Keys,
13. Henzl MR, Buttram V, Segre EJ, Bessler S. The treatment of dysmen-
M.D.; Wyoming, Michigan: Stephen Lown, D.O.; Montgomery, Alabama:
orrhea with naproxen sodium: a report on two independent double-blind
Keith Martin, M.D.; Orlando, Florida: Steven McCarus, M.D.; Warner
trials. Am J Obstet Gynecol 1977;127:818 –23.
Robins, Georgia: James Mitchell, M.D.; Londonderry, New Hampshire:
14. Roy S. A double-blind comparison of a propionic acid derivative
(ibuprofen) and a fenamate (mefenamic acid) in the treatment of dys-
Joseph Montanaro, M.D.; University of Kansas Medical Center, Kansas
menorrhea. Obstet Gynecol 1983;61:628 –32.
City, Kansas: Valerie Montgomery-Rice, M.D.; University of Wisconsin-
15. Jacobsen J. Naproxen in the treatment of OC-resistant primary dysmen-
Madison: David L. Olive, M.D.; Chattanooga, Tennessee: Alfredo Nieves,
orrhea. A double-blind cross-over study. Acta Obstet Gynecol Scand
M.D.; Honolulu, Hawaii: Robb Ohtani, M.D.; Cape May Courthouse, Cape
16. Arnold JD. Comparison of fenoprofen calcium, ibuprofen and placebo
May, New Jersey: Thomas Papperman, M.D.; Albuquerque, New Mexico:
in primary dysmenorrhea. J Reprod Med 1983;14:337–50.
Jeffrey Penikas, M.D.; University of Oklahoma Health Sciences Center,
17. Kistner RW. Treatment of endometriosis by inducing pseudo-preg-
Oklahoma City, Oklahoma: Tony Puckett, M.D.; Richmond, Virginia:
nancy with ovarian hormones. Fertil Steril 1959;10:539 –54.
Nathan Rabhan, M.D.; New York, New York: Lionel Roseff, M.D.; Lan-
18. Robinson JL. Dysmenorrhea and use of oral contraceptives in adoles-
cent women attending a family planning clinic. Am J Obstet Gynecol
ham, Maryland: Cynthia Sadler, M.D.; Shreveport, Louisiana: Darrell San-
difer, M.D.; Tacoma, Washington: Elizabeth Sanford, M.D.; Cornell Med-
19. Milsom I, Sundell G, Andersch B. The influence of different combined
ical College: Glenn L. Schattman, M.D.; Green Lake, Wisconsin: Michael
oral contraceptives on the prevalence and severity of dysmenorrhea.
Seitzinger, M.D.; Monroeville, Pennsylvania: Leonard Selednik, M.D.; Las
20. Milsom I, Andersch B. Effect of various oral contraceptives combina-
Vegas, Nevada: Jane Shen-Gunther, M.D.; Omaha, Nebraska: Kent Siem-
tions on dysmenorrhea. Gynecol Obstet Invest 1984;17:284 –92.
ers, M.D.; Austin, Texas: Kaylen Silverberg, M.D.; Charleston, South
21. Vercellini P, Trespidi L, Colombo A, Vendola N, Marchini M, Crosig-
Carolina: Jack Simmons, Jr., M.D.; Allentown, Pennsylvania: Craig Sobo-
nani PG. A gonadotrophin-releasing hormone agonist versus a low-dose
Gambone et al.
oral contraceptive for pelvic pain associated with endometriosis. Fertil
goserelin treatment in patients with endometriosis. Fertil Steril 1997;
22. Barbieri RL. Endometriosis 1990 — current treatment approaches.
46. Edmonds D, Howell R. Can hormone replacement therapy be used
during medical therapy of endometriosis? Br J Obstet Gynecol 1994;
23. Kauppila A, Telimaa S, Ronnberg L, Vuori J. Placebo-controlled study
on serum concentrations of CA-125 before and after treatment of
47. Kiiholma P, Korhonen M, Tuimala R, Korhonen M, Hagman E. Com-
endometriosis with danazol or high-dose medroxyprogesterone acetate
parison of the gonadotropin-releasing hormone agonist goserelin ace-
alone or after surgery. Fertil Steril 1988;49:37– 41.
tate alone versus goserelin combined with estrogen-progestogen add-
24. Telimaa S, Puolakka J, Ronnberg L, Kauppila A. Placebo-controlled
back therapy in the treatment of endometriosis. Fertil Steril 1995;64:
comparison of danazol and medroxyprogesterone acetate in the treat-
ment of endometriosis. Gynecol Endocrinol 1987;1:13–23.
48. Moghissi KS, Schlaff WD, Olive DL, Skinner MA, Yin H. Goserelin
25. Telimaa S, Apter D, Reinila M, Ronnberg L, Kauppila A. Placebo-
acetate (Zoladex) with or without hormone replacement therapy for the
controlled comparison of hormonal and biochemical effects of danazol
treatment of endometriosis. Fertil Steril 1998;69:1056 – 62.
and high-dose medroxyprogesterone acetate. Eur J Obstet Gynaecol
49. Surrey ES, Voigt B, Fournet N, Judd HL. Prolonged gonadotropin-
releasing hormone agonist treatment of symptomatic endometriosis: the
26. Telimaa S, Ronnberg L, Kauppila A. Placebo-controlled comparison of
role of cyclic sodium etidronate and low dose norethindrone “add-
danazol and high-dose medroxyprogesterone acetate in the treatment of
back” therapy. Fertil Steril 1995;63:747–55.
endometriosis after conservative surgery. Gynecol Endocrinol 1987;1:
50. Hornstein MD, Surrey ES, Weisberg GW, Casino LA, Lupron Add-
Back Study Group. Leuprolide acetate depot and hormonal add-back in
27. Dlugi AM, Miller JD, Knittle J. Lupron depot (leuprolide acetate for
endometriosis: a 12-month study. Obstet Gynecol 1998;91:16 –24.
depot suspension) in the treatment of endometriosis: a randomized,
51. Henzl MR, Kwei L. Efficacy and safety of nafarelin in the treatment of
placebo-controlled, double-blind study. Lupron Study Group. Fertil
endometriosis. Am J Obstet Gynecol 1990;162:570 – 4.
52. Vercellini P, Cortesi I, Crosignani P. Progestins for symptomatic en-
28. Anonymous. Goserelin depot versus danazol in the treatment of endo-
dometriosis: a critical analysis of the evidence. Fertil Steril 1997;68:
metriosis. The Australian/New Zealand experience. Aust NZ J Obstet
53. Fedele L, Arcaini L, Bianchi S, Baglioni A, Vercillini P. Comparison of
29. Chang SP, Ng HT. A randomized comparative study of the effect of
cyproterone acetate and danazol in the treatment of pelvic pain associ-
leuprorelin acetate depot and danazol in the treatment of endometriosis.
ated with endometriosis. Obstet Gynaecol 1989;73:1000 – 4.
Chin Med J (Taipei) 1996;57:431–7.
54. Vercellini P, De Giorgi O, Oldani S, Cortesi I, Panazza S, Crosignani
30. Cirkel U, Ochs H, Schneider HPG. A randomized, comparative trial of
PG. Depot medroxyprogesterone acetate versus an oral contraceptive
triptorelin depot (D-Trp6-LHRH) and danazol in the treatment of en-
combined with very low dose danazol for long term treatment of pelvic
dometriosis. Eur J Obstet Gynecol Reprod Biol 1995;59:61–9.
pain associated with endometriosis. Am J Obstet Gynecol 1996;175:
31. Crosignani PG, Gastaldi A, Lombardi PL. Leuprorelin acetate depot vs
danazol in the treatment of endometriosis: results of an open multicen-
55. Overton C, Lindsay P, Johal B, Collins S, Siddle N, Shaw R, et al. A
tre trial. Clin Ther 1992;14 Suppl A:29 –36.
randomized, double-blind, placebo-controlled study of luteal phase
32. Dmowski WP, Radwanska E, Binor Z, Tummon I, Pepping P. Ovarian
dydrogesterone (Duphaston) in women with minimal to mild endome-triosis. Fertil Steril 1985;43:351–2.
suppression induced with Buserelin or danazol in the management of
56. Vercellini P, Trespidi L, Colombo A, Vendola N, Marchini M, Crosig-
endometriosis: a randomized, comparative study. Fertil Steril 1989;51:
nani PG. A gonadotropin releasing hormone agonist vs low dose oral
contraceptive for pelvic pain associated with endometriosis. Fertil Steril
33. Fraser IS, Shearman RP, Jansen RP, Sutherland PD. A comparative
treatment trial of endometriosis using the gonadotrophin-releasing hor-
57. Fedele L, Arcaini L, Bianchi S, Baglioni A, Vercellini P. Comparison
mone agonist, nafarelin, and the synthetic steroid, danazol. Aust NZ J
of cyproterone acetate and danazol in the treatment of pelvic pain
associated with endometriosis. Obstet Gynecol 1989;73:1000 – 4.
34. Henzl MR, Corson SL, Moghissi K, Buttram VC, Berqvist C, Jacobson
58. Walton SM, Batra HK. The use of medroxyprogesterone acetate 50 mg
J. Administration of nasal nafarelin as compared with oral danazol for
in the treatment of painful pelvic conditions: preliminary results from a
endometriosis. A multicenter double-blind comparative clinical trial.
multicenter trial. J Obstet Gynaecol 1992:12 Suppl 2:S50 –3.
59. Adamson GD, Nelson HP. Surgical treatment of endometriosis. Obstet
35. Adamson GD, Kwei L, Edgren RA. Pain of endometriosis: effects of
Gynecol Clin North Am 1997;24:375– 408.
nafarelin and danazol therapy. Int J Fertil Menopausal Stud 1994;39:
60. Telimaa S, Ronnberg L, Kauppila A. Placebo-controlled comparison of
danazol and high-dose medroxyprogesterone acetate in the treatment of
36. Wheeler JM, Knittle JD, Miller JD. Depot leuprolide versus danazol in
endometriosis after conservative surgery. Gynecol Endocrinol 1987;1:
treatment of women with symptomatic endometriosis. I. Efficacy re-
sults. Am J Obstet Gynecol 1992;167:1367–71.
61. Bianchi S, Busacca M, Agnoli B, Candiani M, Calia C, Vignali M.
37. Dawood MY, Ramos J, Khan-Dawood FS. Depot leuprolide acetate
Effects of 3 month therapy with danazol after laparoscopic surgery for
versus danazol for treatment of pelvic endometriosis: changes in ver-
stage III/IV endometriosis: a randomized study. Hum Reprod 1999;14:
tebral bone mass and serum estradiol and calcitonin. Fertil Steril 1995;
62. Morgante G, Ditto A, La Marca A, De Leo V. Low-dose danazol after
38. The Nafarelin European Endometriosis Trial Group (NEET). Nafarelin
combined surgical and medical therapy reduces the incidence of pelvic
for endometriosis: a large-scale, danazol-controlled trial of efficacy and
pain in women with moderate and severe endometriosis. Hum Reprod
safety, with 1-year follow-up. Fertil Steril 1992;57:514 –22.
39. Rolland R, van der Heijden PF. Nafarelin versus danazol in the treat-
63. Parazzini F, Fedele L, Busacca M, Falsetti L, Pellegrini S, Venturini
ment of endometriosis. Am J Obstet Gynecol 1990;162:586 – 8.
PL, et al. Postsurgical medical treatment of advanced endometriosis:
40. Kennedy SH, Williams IA, Brodribb J, Barlow DH, Shaw RW. A
results of a randomized clinical trial. Am J Obstet Gynecol 1994;171:
comparison of nafarelin acetate and danazol in the treatment of endo-
metriosis. Fertil Steril 1990;53:998 –1003.
64. Vercellini P, Crosignani PG, Fadini R, Radici E, Belloni C, Sismondi
41. Rock JA. A multicenter comparison of GnRH agonist (Zoladex) and
P. A gonadotrophin-releasing hormone agonist compared with expect-
danazol in the treatment of endometriosis. Fertil Steril 1991;56:S49.
ant management after conservative surgery for symptomatic endome-
42. Shaw RW. An open randomized comparative study of the effect of
triosis. Br J Obstet Gynaecol 1999;106:672–7.
goserelin depot and danazol in the treatment of endometriosis. Zoladex
65. Hornstein MD, Hemmings R, Yuzpe AA, Heinrichs WL. Use of na-
Endometriosis Study Team. Fertil Steril 1992;58:265–72.
farelin versus placebo after reductive laparoscopic surgery for endome-
43. Surrey E, Judd H. Reduction of vasomotor symptoms and bone mineral
triosis. Fertil Steril 1997;68:860 – 4.
density loss with combined norethindrone and long-acting gonado-
66. Winkel CA, Bray M, eds. Treatment of women with endometriosis
tropin-releasing hormone agonist therapy of symptomatic endometrio-
using excision alone, ablation alone, or ablation in combination with
sis: a prospective randomized trial. J Clin Endocrinol Metab 1992;75:
leuprolide acetate [abstract no. 105]. Proceedings of the 5th World
Congress on Endometriosis, Oct. 21–24, 1996, Pacifico, Yokohama,
44. Makarainen L, Ronneberg L, Kauppila A. Medroxyprogesterone ace-
tate supplementation diminishes the hypoestrogenic side-effects of go-
67. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized,
nadotropin-releasing hormone agonists without changing its efficacy in
double-blind, controlled trial of laser laparoscopy in the treatment of
endometriosis. Fertil Steril 1996;65:29 –34.
pelvic pain associated with minimal, mild, and moderate endometriosis.
45. Tabkin O, Yakinoghe AH, Kucuk S, Uryan I, Buhur A, Burak F.
Effectiveness of tibolone on hypoestrogenic symptoms induced by
68. Redwine DB. Conservative laparoscopic excision of endometriosis by
FERTILITY & STERILITY
sharp dissection: life table analysis of reoperation and persistent or
neurectomy for the relief of midline dysmenorrhea. Obstet Gynecol
recurrent disease. Fertil Steril 1991;56:628 –34.
69. Sutton C, Pooley AS, Jones KD, Dover RW, Haines P. A prospective,
80. Chen FP, Chang SD, Chu K, Soong YK. Comparison of laparoscopic
randomized, double-blind controlled trial of laparoscopic uterine nerve
presacral neurectomy and laparoscopic uterine nerve ablation for pri-
ablation in the treatment of pelvic pain associated with endometriosis.
mary dysmenorrhea. J Reprod Med 1996;41:463– 6.
81. Namnoum AB, Hickman TN, Goodman AB, Gehlbach DL, Rock JA.
70. Fayez JA, Vogel MF. Comparison of different treatment methods of
Incidence of symptom recurrence after hysterectomy for endometriosis.
endometriomas by laparoscopy. Obstet Gynecol 1991;78:660 –5.
71. Saleh A, Tulandi T. Reoperation after laparoscopic treatment of ovarian
82. Chassin MR, Brook RH, Park RE, Keesey J, Fink A, Kosecoff J, et al.
endometriomas by excision and by fenestration. Fertil Steril 1999;72:
Variations in the use of medical and surgical services by the Medicare
population. N Engl J Med 1986;314:285–90.
72. Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Random-
83. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesis of
ized clinical trial of two laparoscopic treatments of endometriomas:
best evidence for clinical practice. Ann Intern Med 1997;126:376 – 80.
cystectomy versus drainage and coagulation. Fertil Steril 1998;70:
84. Leape LL, Park RE, Kahan JP, Brook RH. Group judgments of appro-
priateness: the effect of panel composition. Qual Assur Health Care
73. Crosignani PG, Vercellini P, Biffignandi F, Costantini W, Cortesi I,
Imparato E. Laparoscopy versus laparotomy in conservative surgical
85. Reiter RC, Gambone JC. Nongynecologic somatic pathology in women
treatment for severe endometriosis. Fertil Steril 1996;66:706 –11.
with chronic pelvic pain and negative laparoscopy. J Reprod Med
74. Busacca M, Fedele L, Bianchi S, Candiani M, Agnoli B, Raffaelli R, et
al. Surgical treatment of recurrent endometriosis: laparotomy versus
86. Walling MK, Reiter RC, O’Hara MW, Milburn AK, Lilly G, Vincent
laparoscopy. Hum Reprod 1998;13:2271– 4.
SD. Abuse history and chronic pain in women: I. Prevalences of sexual
75. Catalano GF, Marana R, Caruana P, Muzii L, Mancusco S. Laparos-
abuse and physical abuse. Obstet Gynecol 1994;84:193–9.
copy versus microsurgery by laparotomy for excision of ovarian cysts
87. Lampe A, Solder E, Ennemoser A, Schubert C, Rumpold G, Sollner W.
in patients with moderate or severe endometriosis. J Am Assoc Gynecol
Chronic pelvic pain and previous sexual abuse. Obstet Gynecol 2000;
76. Bateman BG, Kolp LA, Mills S. Endoscopy versus laparotomy man-
88. Collett BJ, Cordle CJ, Stewart CR, Jagger C. A comparative study of
agement of endometriomas. Fertil Steril 1994;62:690 –5.
women with chronic pelvic pain, chronic nonpelvic pain and those with
77. Lichten EM, Bombard J. Surgical treatment of primary dysmenorrhea
no history of pain attending general practitioners. Br J Obstet Gynaecol
with laparoscopic uterine nerve ablation. J Reprod Med 1987;32:37–
89. Carlson KJ, Miller BA, Fowler FJ Jr. The Maine Women’s Health
78. Candiani GB, Fedele L, Vercellini P, Bianch S, Di Nola G. Presacral
Study: I. Outcomes of hysterectomy. Obstet Gynecol 1994;83:556 – 65.
neurectomy for the treatment of pelvic pain associated with endome-
90. Kjerulff KH, Rhodes JC, Langenberg PW, Harvey LA. Patient satis-
triosis: a controlled study. Am J Obstet Gynecol 1992;167(1):100 –3.
faction with results of hysterectomy. Am J Obstet Gynecol
79. Tjaden B, Schlaff WD, Kimball A, Rock JA. The efficacy of presacral
Gambone et al.
Camp Chen-A-Wanda Camper Health History Form Please complete pages 1-3 and 5 and have your child’s Name: __________________________________________________ physician complete and sign page 4 . All forms must be completed and submitted along with Dates of Attendance ___________ to __________ copies of your child’s health insurance cards by by June 1st for camp to give treatment
University of Wisconsin Research Subject Information and Consent Form A Randomized, Double-Blind, Placebo-Controlled Trial of Spironolactone versus Eplerenone in Patients with Mild to Moderate Heart Failure Investigator: [name and contact information] INVITATION/SUMMARY You are invited to participate in a research study about medications used to treat heart failure. You

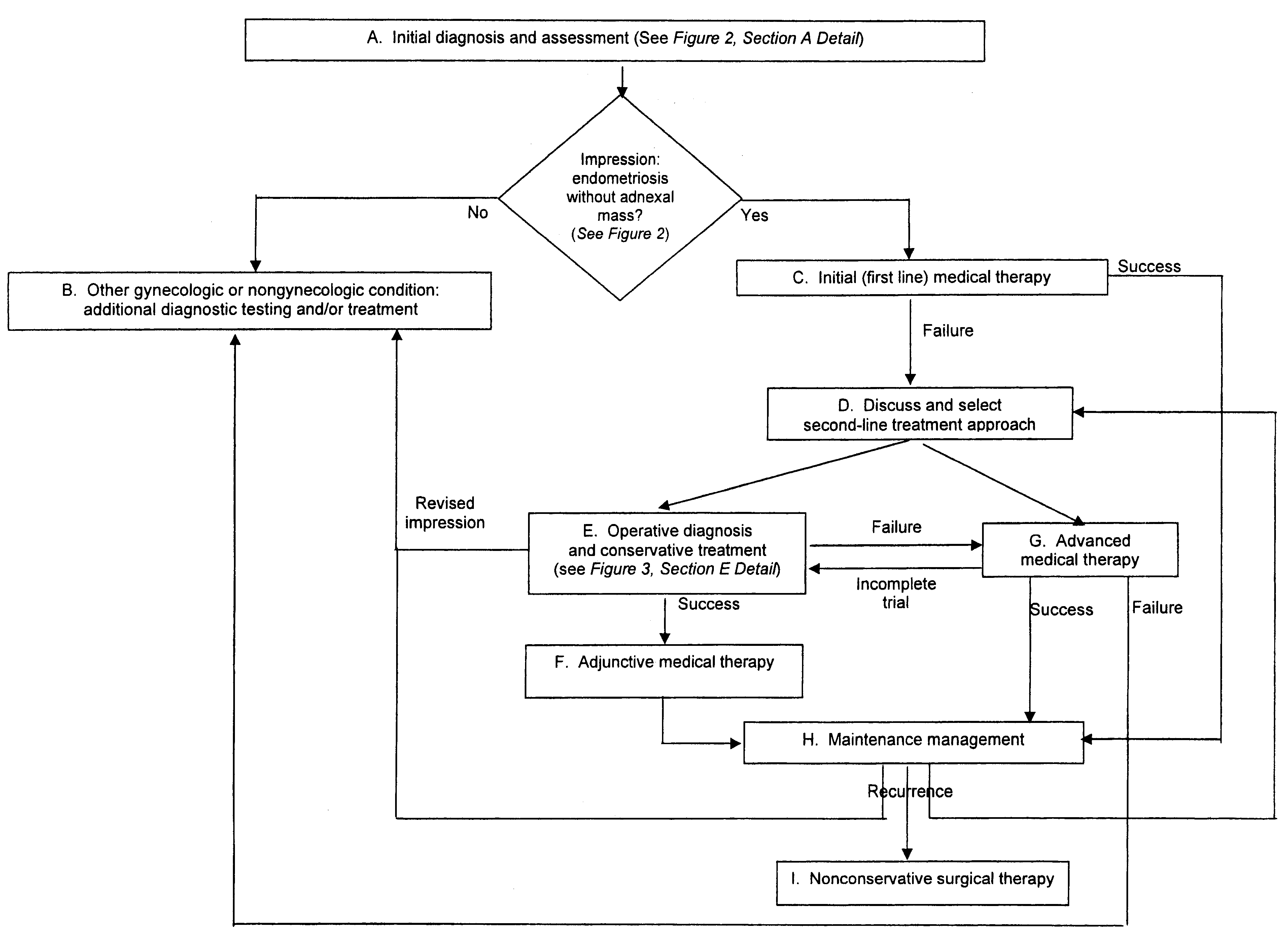 Algorithm that delineates the steps for the assessment, diagnosis, and treatment options of patients with chronic pelvic painand presumed endometriosis: overall approach.
Algorithm that delineates the steps for the assessment, diagnosis, and treatment options of patients with chronic pelvic painand presumed endometriosis: overall approach.
 ● Blood tests, including complete blood count with dif-
ferential and erythrocyte sedimentation rate
Closer view of section A of overall algorithm shown in Figure
● CA-125 (in selected cases, e.g., evidence of ascites)
1: initial assessment of patients with chronic pelvic pain andpresumed endometriosis.
● Blood tests, including complete blood count with dif-
ferential and erythrocyte sedimentation rate
Closer view of section A of overall algorithm shown in Figure
● CA-125 (in selected cases, e.g., evidence of ascites)
1: initial assessment of patients with chronic pelvic pain andpresumed endometriosis.
 Closer view of section E of overall algorithm shown in Figure 1: laparoscopic diagnosis and conservative treatment ofendometriosis.
Closer view of section E of overall algorithm shown in Figure 1: laparoscopic diagnosis and conservative treatment ofendometriosis.