Levitra has a minimal amount of contraindications which has increased its popularity cialis uk You can buy quality certified medications from us at an affordable price.
Tiotropium bromide step-up therapy for adults with uncontrolled asthma (talc trial)
Tiotropium bromide Step-Up Therapy for Adults with Uncontrolled Asthma (TALC trial)
Peters, S. et al. NEJM 363(18)1715-1726. Oct. 28, 2010
Rationale: - short acting anticholinergics have been around for decades and have been used for acute and chronic management of both COPD and asthma - Cochrane review 2004 “no justification for routinely introducing anticholinergics as part of add-on treatment for patients whose asthma is not well controlled on standard therapies.” This review looked at short acting anticholinergics (ipratropium) only. - Tiotropium approved for use in 2004 for COPD only - Recent (controversial) safety concerns of LABAs has fueled interest in looking for alternative step up therapies for asthma Methods: Hypothesis 1: In patients with asthma that is inadequately controlled by an inhaled glucocorticoid alone, the addition of tiotropium would be superior to doubling the dose of ICS Hypothesis 2: In such patients, the addition of tiotropium would not be inferior to the addition of a LABA Patient enrollment: (See figure 1) Enrolled 826 patient to two common trials (BASALT, TALC), 210 were randomized to TALC if FEV1 <70% predicted or had symptoms or rescue inhaler use 6 or more days per week or were awakened by asthma symptoms 2 or more nights/week Inclusion criteria
- use of prohibited medications (other asthma meds, other
- clinical history consistent with asthma
- significant medical illnesses or lung diseases other than asthma
- asthma confimed by : 1) reversibility ≥12% with 4 puffs
albuterol 2) PC20≤8 not on ICS or ≤16 on ICS
- RTI or significant asthma exacerbation in the past 4 weeks
- need for daily controller therapy (used or received prescription
- history of life-threatening asthma in the past 5 years
for asthma controller in the past year OR symptoms more than
- pregnant or not using acceptable birth control
- hyposensitization therapy other than established regimen
- If on steroid, not exceeding equivalent of 1000 mcg fluticasone
- inability to use drug delivery devices effectively
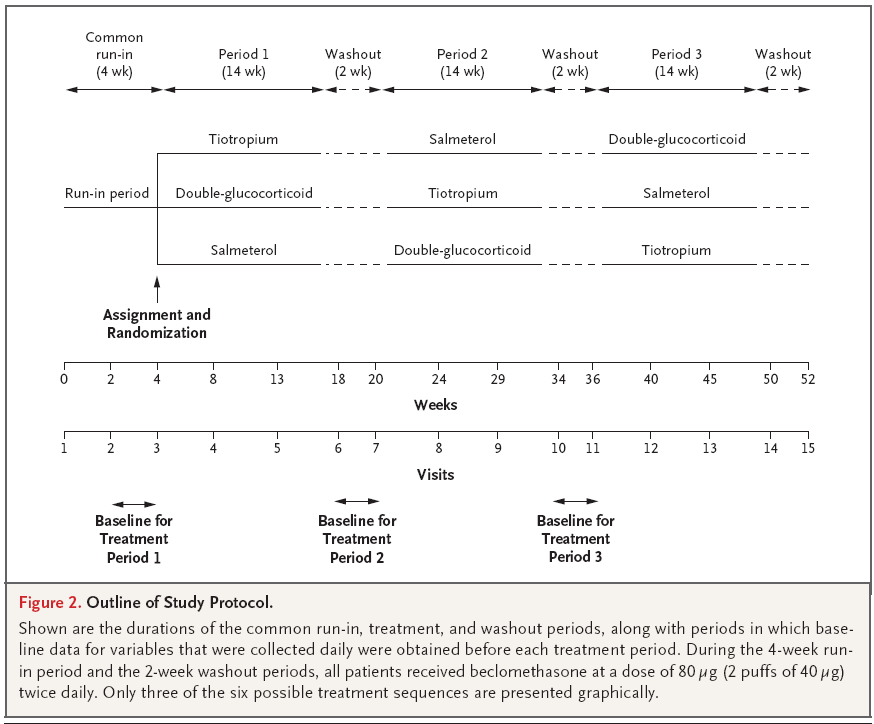
- Nonsmoker (<10 pk years, no smoking in past year) - able to provide informed consent Protocol:
Outcomes: Primary outcome: morning PEF Secondary outcomes: FEV1 before bronchodilation, number of asthma-control days (days without symptoms or use of rescue inhaler), asthma symptoms, rescue bronchodilator use, asthma exacerbations, use of health care services, biomarkers of inflammation, questionnaires on symptoms and quality of life Study oversight: Study funded by the National Heart, Lung and Blood Institute’s Asthma Clinical Research Network (not pharma) Statistical analysis: Intention to treat Results: √ Hypothesis #1: Tiotropium is superior to doubling dose of glucocorticoid Morning PEF was 25.8 L/min higher in patients receiving tiotropium compared with double dose glucocorticoid (P<0.001). Other indices also superior: higher prebronchodilator FEV1 0.1 L (P=0.004), increase in proportion of asthma control days of 0.079 (P=0.01), FEV1 after four puffs of albuterol 0.04 (P=0.01) √ Hypothesis #2: Tiotropium is not inferior to salmeterol as add-on Addition of tiotropium was noninferior to the addition of salmeterol for all assessed outcomes and increased the prebronchodilator FEV1 more than did salmeterol, with a difference of 0.11 liters (P=0.003). 12 adverse events (3 for tiotropium, 4 for double dose beclomethasone, 4 for salmeterol and one during run in) Discussion and Critical Analysis: 1. Are the results valid? - Method of randomization not described. - All patients were accounted for in figure 1. – Intention to treat - Three way, double-blind, triple dummy crossover trial - All groups treated similarly 2. What were the results? - Superiority of tiotropium over double dose glucocorticoid significant but ?clinically significant - No significant difference between tiotropium and salmeterol for primary outcome and most measures. Prebronchodilator FEV1 favoured tiotropium, though this was a small difference and a secondary outcome so ?clinical relevance. 3. Will the results help me in caring for pts? - inclusion/exclusion criteria themselves reasonable and fairly inclusive, but subsequent selection of patients for TALC vs BASALT selected significantly obstructed population for TALC. This may be reasonable for a noninferiority trial - trial done in ideal circumstances – frequent visits, excellent compliance (beclomethasone 84% of doses, salmeterol 93%, tiotropium 93%). Poor compliance (<75%) excluded Were all clinically NB outcomes considered? - PEF as primary endpoint is less clinically meaningful. Secondary endpoints were more clinically meaningful – FEV1, asthma control days - Limited duration of study does not permit evaluation of whether tiotropium reduces asthma exacerbations Was noninferiority appropriate design? - Design of noninferiority trial implies that we do not care if tiotropium is better, as long as it is equivalent we would consider using it over salmeterol – big and potentially untrue assumption. Safety concerns with LABAs highly controversial. - May be ethically challenging to design superiority trial for tiotropium without doing this study first. This may create clinical equipoise to perform longer term superiority study using clinically relevant outcomes.
Informe especial / Special report Treatment of type 2 diabetes in Latin America: a consensus statement by the medical associations of 17 Latin American countries Juan Rosas Guzmán,1 Ruy Lyra,2 Carlos A. Aguilar-Salinas,3Saulo Cavalcanti,4 Felix Escaño,5 Marcos Tambasia,6Elizabeth Duarte,7 and the ALAD Consensus Group1 Suggested citation Guzmán JR, Lyra R, Aguilar-Salinas CA, Cavalcanti
Schriftenverzeichnis Franz Ludwig Dumoulin (nur in PubMed gelistete Veröffentlichungen) Nin N, Lombardi R, Frutos-Vivar F, Esteban A, Lorente JA, Ferguson ND, et al. Early and small changes in serum creatinine concentrations are associated with mortality in mechanically ventilated patients. Shock. 2010; 34(2):109-16. Kerker A, Hardt C, Schlief HE, Dumoulin FL. Combined sedation with midazol
 Tiotropium bromide Step-Up Therapy for Adults with Uncontrolled Asthma (TALC trial)
Tiotropium bromide Step-Up Therapy for Adults with Uncontrolled Asthma (TALC trial)