Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients levitra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Diclegis.com
HIGHLIGHTS OF PRESCRIBING INFORMATION ------------------------ WARNINGS AND PRECAUTIONS --------------------- These highlights do not include all the information needed to use DICLEGIS safely and effectively. See full prescribing information for
Activities requiring mental alertness: Avoid engaging in activities
DICLEGIS.
requiring complete mental alertness, such as driving or operating heavy machinery, while using DICLEGIS until cleared to do so by a healthcare
DICLEGIS (doxylamine succinate and pyridoxine hydrochloride) delayed-release tablets, for oral use. Initial U.S. Approval: 1976
Central nervous system (CNS) depressants: Concurrent use with alcohol
or other CNS depressants is not recommended (5.1)
---------------------------- INDICATIONS AND USAGE --------------------------
Anticholinergic actions: Use with caution in patients with asthma,
DICLEGIS is a fixed dose combination drug product of doxylamine succinate,
increased intraocular pressure, narrow angle glaucoma, stenosing peptic
an antihistamine, and pyridoxine hydrochloride, a Vitamin B6 analog,
ulcer, pyloroduodenal obstruction and urinary bladder-neck obstruction
indicated for the treatment of nausea and vomiting of pregnancy in women
who do not respond to conservative management. (1)
------------------------------- ADVERSE REACTIONS ---------------------------- ----------------------- DOSAGE AND ADMINISTRATION ----------------------
The most common adverse reaction with DICLEGIS (≥5 percent and
Take two tablets daily at bedtime. If symptoms are not adequately controlled,
exceeding the rate in placebo) is somnolence. (6)
the dose can be increased to a maximum recommended dose of four tablets daily (one in the morning, one mid-afternoon and two at bedtime) as described
To report SUSPECTED ADVERSE REACTIONS, contact Duchesnay
in the full prescribing information. (2)
Inc. at 1-855-722-7734or [email protected] or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. ---------------------- DOSAGE FORMS AND STRENGTHS ------------------- ------------------------------- DRUG INTERACTIONS ----------------------------
Delayed-release tablets containing 10 mg doxylamine succinate and 10 mg pyridoxine hydrochloride. (3)
Severe drowsiness can occur when used in combination with alcohol or
-------------------------------CONTRAINDICATIONS----------------------------- ------------------------USE IN SPECIFIC POPULATIONS----------------------
Known hypersensitivity to doxylamine succinate, other ethanolamine
derivative antihistamines, pyridoxine hydrochloride or any inactive
Pregnancy Category A. DICLEGIS is intended for use in pregnant women.
Monoamine oxidase (MAO) inhibitors (4, 7)
See 17 for PATIENT COUNSELING INFORMATION and FDA- approved patient labeling. Revised: 04/2013 FULL PRESCRIBING INFORMATION: CONTENTS* INDICATIONS AND USAGE 10 OVERDOSAGE DOSAGE AND ADMINISTRATION DOSAGE FORMS AND STRENGTHS 11 DESCRIPTION CONTRAINDICATIONS 12 CLINICAL PHARMACOLOGY WARNINGS AND PRECAUTIONS
5.1 Activities Requiring Mental Alertness
13 NONCLINICAL TOXICOLOGY ADVERSE REACTIONS
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES 16 HOW SUPPLIED/STORAGE AND HANDLING DRUG INTERACTIONS 17 PATIENT COUNSELING INFORMATION USE IN SPECIFIC POPULATIONS *Sections or subsections omitted from the full prescribing information are not FULL PRESCRIBING INFORMATION 1 INDICATIONS
DICLEGIS is indicated for the treatment of nausea and vomiting of pregnancy in women who do not respond to conservative management. Limitations of Use
DICLEGIS has not been studied in women with hyperemesis gravidarum. 2 DOSAGE AND ADMINISTRATION 2.1 Dosage Information Initially, take two DICLEGIS delayed-release tablets orally at bedtime (Day 1). If this dose adequately controls symptoms the next day, continue taking two tablets daily at bedtime. However, if symptoms persist into the afternoon of Day 2, take the usual dose of two tablets at bedtime that night then take three tablets starting on Day 3 (one tablet in the morning and two tablets at bedtime). If these three tablets adequately control symptoms on Day 4, continue taking three tablets daily. Otherwise take four tablets starting on Day 4 (one tablet in the morning, one tablet mid-afternoon and two tablets at bedtime). The maximum recommended dose is four tablets (one in the morning, one in the mid-afternoon and two at bedtime) daily. Take on an empty stomach with a glass of water [see Clinical Pharmacology (12.3)]. Swallow tablets whole. Do not crush, chew, or split DICLEGIS tablets. Take as a daily prescription and not on an as needed basis. Reassess the woman for continued need for DICLEGIS as her pregnancy progresses. 3 DOSAGE FORMS AND STRENGTHS
DICLEGIS delayed-release tablets are white, round, film coated tablets containing 10 mg doxylamine succinate and 10 mg pyridoxine hydrochloride. The tablets are imprinted with the pink image of a pregnant woman on one side. 4 CONTRAINDICATIONS DICLEGIS is contraindicated in women with any of the following conditions:
Known hypersensitivity to doxylamine succinate, other ethanolamine derivative antihistamines,
pyridoxine hydrochloride or any inactive ingredient in the formulation
Monoamine oxidase (MAO) inhibitors intensify and prolong the adverse central nervous system effects
of DICLEGIS [see Drug Interactions (7.1)].
WARNINGS AND PRECAUTIONS
5.1 Activities Requiring Mental Alertness DICLEGIS may cause somnolence due to the anticholinergic properties of doxylamine succinate, an antihistamine. Women should avoid engaging in activities requiring complete mental alertness, such as driving or operating heavy machinery, while using DICLEGIS until cleared to do so by their healthcare provider. DICLEGIS use is not recommended if a woman is concurrently using central nervous system (CNS) depressants including alcohol. The combination may result in severe drowsiness leading to falls or accidents [see Drug Interactions (7.1)].
5.2 Concomitant Medical Conditions DICLEGIS has anticholinergic properties and, therefore, should be used with caution in women with: asthma, increased intraocular pressure, narrow angle glaucoma, stenosing peptic ulcer, pyloroduodenal obstruction and urinary bladder-neck obstruction. 6 ADVERSE REACTIONS The following adverse reactions are discussed elsewhere in the labeling: Somnolence [see Warnings and Precautions (5.1)]
Falls or other accidents resulting from the effect of the combined use of DICLEGIS with CNS depressants
including alcohol [see Warnings and Precautions (5.1)] 6.1 Clinical Trial Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. The safety and efficacy of DICLEGIS were compared to placebo in a double-blind, randomized, multi-center trial in 261 women with nausea and vomiting of pregnancy. The mean gestational age at enrollment was 9.3 weeks, range 7 to 14 weeks gestation [see Clinical Studies (14)]. Adverse reactions for DICLEGIS that occurred at an incidence ≥5 percent and exceeded the incidence for placebo are summarized in Table 1. Table 1: Number (Percent) of Subjects with ≥ 5 Percent Adverse Reactions in a 15-Day Placebo- Controlled Study of DICLEGIS (Only Those Adverse Reactions Occurring at an Incidence ≥ 5 Percent and at a Higher Incidence with DIGLEGIS than Placebo are Shown) 6.2 Postmarketing Experience The following adverse events, listed alphabetically, have been identified during post-approval use ofthe combination of 10 mg doxylamine succinate and 10 mg pyridoxine hydrochloride. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Cardiac disorders: dyspnea, palpitation, tachycardia Ear and labyrinth disorders: vertigo Eye disorders: vision blurred, visual disturbances Gastrointestinal disorders: abdominal distension, abdominal pain, constipation, diarrhea General disorders and administration site conditions: chest discomfort, fatigue, irritability, malaise Immune system disorders: hypersensitivity Nervous system disorders: dizziness, headache, migraines, paresthesia, psychomotor hyperactivity Psychiatric disorders: anxiety, disorientation, insomnia, nightmares Renal and urinary disorders: dysuria, urinary retention Skin and subcutaneous tissue disorders: hyperhidrosis, pruritus, rash, rash maculo-papular 7 DRUG INTERACTIONS
7.1 Drug Interactions Use of DICLEGIS is contraindicated in women who are taking monoamine oxidase inhibitors (MAOIs), which prolong and intensify the anticholinergic (drying) effects of antihistamines. Concurrent use of alcohol and other CNS depressants (such as hypnotic sedatives and tranquilizers) with DICLEGIS is not recommended. 7.2 Drug-Food Interactions A food-effect study demonstrated that the delay in the onset of action of DICLEGIS may be further delayed, and a reduction in absorption may occur when tablets are taken with food [see Dosage and Administration (2), Clinical Pharmacology (12.3)]. Therefore, DICLEGIS should be taken on an empty stomach with a glass of water [see Dosage and Administration (2)]. 8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category A
DICLEGIS is intended for use in pregnant women. The combination of doxylamine succinate and pyridoxine hydrochloride has been the subject of many epidemiological studies (cohort, case control and meta-analyses) designed to detect possible teratogenicity. A meta-analysis of 16 cohort and 11 case-control studies published between 1963 and 1991 reported no increased risk for malformations from first trimester exposures to doxylamine succinate and pyridoxine hydrochloride, with or without dicyclomine hydrochloride. A second meta-analysis of 12 cohort and 5 case-control studies published between 1963 and 1985 reported no statistically significant relationships between fetal abnormalities and the first trimester use of the combination doxylamine succinate and pyridoxine hydrochloride with or without dicyclomine hydrochloride. Animal Data The effects of doxylamine succinate and pyridoxine hydrochloride on embryofetal development have been studied in rats and monkeys. Once daily treatment of pregnant rats with doxylamine succinate and pyridoxine hydrochloride during organogenesis (gestational day (GD) 6-15) resulted in increased fetal resorptions, decreased fetal body weight and increased skeletal variations with reduced ossification at doses 60 to 100 times the highest clinical dose based on body surface area. Pregnant cynomolgus monkeys were treated once daily with doxylamine succinate and pyridoxine hydrochloride during organogenesis (GD 22-50). At birth, there were no observed malformations, and no evidence of embryo, fetal or maternal toxicity at doses up to 3.2 times the highest proposed clinical dose based on body surface area. In a similarly designed study in pregnant cynomolgus and rhesus monkeys and baboons, ventricular septal defects (VSDs) were observed in the preterm (GD 100) fetuses. Doses used in this study were 0.5-20 times higher than the clinical dose based on body surface area, with no relationship between dose and incidence of VSD. There were no VSDs in infant monkeys at term. No VSDs were observed at GD 100 in cynomolgus monkeys administered the combination of doxylamine succinate and pyridoxine hydrochloride for 4-day periods between 22 and 41 days of gestation. 8.3 Nursing Mothers Women should not breastfeed while using DICLEGIS. The molecular weight of doxylamine succinate is low enough that passage into breast milk can be expected. Excitement, irritability and sedation have been reported in nursing infants presumably exposed to doxylamine succinate through breast milk. Infants with apnea or other respiratory syndromes may be particularly vulnerable to the sedative effects of DICLEGIS resulting in worsening of their apnea or respiratory conditions. Pyridoxine hydrochloride is excreted into breast milk. There have been no reports of adverse events in infants presumably exposed to pyridoxine hydrochloride through breast milk. 8.4 Pediatric Use The safety and effectiveness of DICLEGIS in children under 18 years of age have not been established. Fatalities have been reported from doxylamine overdose in children. The overdose cases have been characterized by coma, grand mal seizures and cardiorespiratory arrest. Children appear to be at a high risk for cardiorespiratory arrest. A toxic dose for children of more than 1.8 mg/kg has been reported. A 3 year old child died 18 hours after ingesting 1,000 mg doxylamine succinate. However, there is no correlation between the amount of doxylamine ingested, the doxylamine plasma level and clinical symptomatology.
10 OVERDOSAGE 10.1 Signs and Symptoms of Overdose
DICLEGIS is a delayed-release formulation, therefore, signs and symptoms of intoxication may not be apparent immediately. Signs and symptoms of overdose may include restlessness, dryness of mouth, dilated pupils, sleepiness, vertigo, mental confusion and tachycardia. At toxic doses, doxylamine exhibits anticholinergic effects, including seizures, rhabdomyolysis, acute renal failure and death. 10.2 Management of Overdose
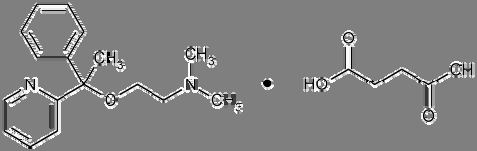
If treatment is needed, it consists of gastric lavage or activated charcoal, whole bowel irrigation and symptomatic treatment. For additional information about overdose treatment, call a poison control center (1-800-222-1222). 11 DESCRIPTION DICLEGIS (doxylamine succinate and pyridoxine hydrochloride) delayed-release tablets are round, white, film- coated, delayed-release tablets containing 10 mg of doxylamine succinate and 10 mg of pyridoxine hydrochloride. Tablets are imprinted on one side with the pink image of a pregnant woman. Inactive ingredients are as follows: ammonium hydroxide, n-butanol, carnauba wax powder, colloidal silicon dioxide, croscarmellose sodium, D&C Red#27, denatured alcohol, FD&C Blue#2, hypromellose, isopropyl alcohol, magnesium stearate, magnesium trisilicate, methacrylic acid copolymer, microcrystalline cellulose 102, PEG 400, PEG 8000, polysorbate 80, propylene glycol, shellac glaze, simethicone, talc, titanium dioxide. Doxylamine Succinate Doxylamine succinate is classified as an antihistamine. The chemical name for doxylamine succinate is ethanamine, N,N-dimethyl-2-[1-phenyl-1-(2-pyridinyl)ethoxy]-, butanedioate (1:1). The empirical formula is C17H22N2O • C4H6O4 and the molecular mass is 388.46. The structural formula is:
Doxylamine succinate is a white to creamy white powder that is very soluble in water and alcohol, freely soluble in chloroform and very slightly soluble in ether and benzene.
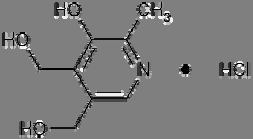
Pyridoxine Hydrochloride Pyridoxine hydrochloride is a vitamin B6 analog. The chemical name for pyridoxine hydrochloride is 3,4- pyridinedimethanol, 5-hydroxy-6-methyl-, hydrochloride. The empirical formula is C8H11NO3 • HCl and the
molecular mass is 205.64. The structural formula is: Pyridoxine hydrochloride is a white or practically white crystalline powder that is freely soluble in water, slightly soluble in alcohol and insoluble in ether. 12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action The mechanism of action of DICLEGIS is unknown. 12.3 Pharmacokinetics
The pharmacokinetics of DICLEGIS has been characterized in healthy non-pregnant adult women. Pharmacokinetic results for doxylamine and pyridoxine, including its vitamin B6 metabolites, pyridoxal, pyridoxal 5’-phosphate, pyridoxamine and pyridoxamine 5’-phosphate, are summarized in Tables 2 to 5. Absorption A single-dose (two tablets) and multiple-dose (four tablets daily), open-label study was conducted to assess the safety and pharmacokinetic profile of DICLEGIS administered in healthy non-pregnant adult women. Single- doses (two tablets at bedtime) were administered on Days 1 and 2. Multiple-doses (one tablet in the morning, one tablet in the afternoon and two tablets at bedtime) were administered on Days 3-18. Blood samples for pharmacokinetic analysis were collected pre-and post-dose on Days 2 and 18 as well as pre- dose prior to bedtime dose only (trough) on Days 9, 10, 11, 16, 17, and 18. Doxylamine and pyridoxine are absorbed in the gastrointestinal tract, mainly in the jejunum. The Cmax of doxylamine and pyridoxine are achieved within 7.5 and 5.5 hours, respectively (see Table 2). Table 2 – Single-Dose and Multiple-Dose Pharmacokinetics of DICLEGIS in Healthy Non-Pregnant Adult Women Single Dose Multiple Dose AUC0-inf AUC0-inf (ng•h/mL) (ng•h/mL) Doxylamine Pyridoxine Pyridoxal Pyridoxal 5`Phosphate Pyridoxamine 2.7 Pyridoxamine 5.2 ± 5'-phosphate Multiple-dose administration of DICLEGIS results in increased concentrations of doxylamine as well as increases in doxylamine Cmax and AUC0-last of absorption. The time to reach the maximum concentration is not
affected by multiple doses. The mean accumulation index is more than 1.0 suggesting that doxylamine accumulates following multiple dosing (see Table 3). Although no accumulation was observed for pyridoxine, the mean accumulation index for each metabolite (pyridoxal, pyridoxal 5’-phosphate, and pyridoxamine 5’-phosphate) is more than 1.0 following multiple-dose administration of DICLEGIS. The time to reach the maximum concentration is not affected by multiple doses (see Table 2). Table 3 – Pharmacokinetics of Doxylamine and Pyridoxine Following Single Dose and Multiple Dose Administration of DICLEGIS to Healthy Non-Pregnant Adult Women AUC0-last AUC0-inf (ng•h/mL) (ng•h/mL) Doxylamine Single Multiple Pyridoxine Single Multiple
Food Effect The administration of food delays the absorption of both doxylamine and pyridoxine. This delay is associated with a lower peak concentration of doxylamine, but the extent of absorption is not affected (see Table 4). The effect of food on the peak concentration and the extent of absorption of the pyridoxine component is more complex because the pyridoxal, pyridoxamine, pyridoxal 5’-phosphate and pyridoxamine 5’-phosphate metabolites also contribute to the biological activity. Food significantly reduces the bioavailability of pyridoxine, lowering its Cmax and AUC by approximately 50% compared to fasting conditions. Similarly, food
significantly reduces pyridoxal AUC and reduces its Cmax by 50% compared to fasting conditions. In contrast,
food slightly increases pyridoxal 5’-phosphate Cmax and extent of absorption. As for pyridoxamine and
pyridoxamine 5’-phosphate, the rate and extent of absorption seem to decrease under fed conditions. Table 4 – Pharmacokinetics of Doxylamine and Pyridoxine Following Administration of DICLEGIS Under Fed and Fasted Conditions in Healthy Non-Pregnant Adult Women AUC0-inf (ng•h/mL) (ng•h/mL) Doxylamine Fasted Pyridoxine Fasted
a N=37; b N=18; c N=31 Distribution Pyridoxine is highly protein bound, primarily to albumin. Its main active metabolite, pyridoxal 5’-phosphate (PLP) accounts for at least 60% of circulating vitamin B6 concentrations. Metabolism Doxylamine is biotransformed in the liver by N-dealkylation to its principle metabolites N-desmethyl- doxylamine and N, N-didesmethyldoxylamine. Pyridoxine is a prodrug primarily metabolized in the liver. Excretion The principle metabolites of doxylamine, N-desmethyl-doxylamine and N, N-didesmethyldoxylamine, are excreted by the kidney. The terminal elimination half-life of doxylamine and pyridoxine are 12.5 hours and 0.5 hours, respectively (see Table 5). Table 5 – Terminal Elimination Half-Life (T1/2el) for DICLEGIS Administered as a Single Dose of Two Tablets under Fasting Conditions in Healthy Non-Pregnant Adult Women Use in Specific Populations Race: No pharmacokinetic studies have been conducted related to race. Hepatic Impairment: No pharmacokinetic studies have been conducted in hepatic impaired patients. Renal Impairment: No pharmacokinetic studies have been conducted in renal impaired patients. 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis and Impairment of Fertility Carcinogenicity Two-year carcinogenicity studies in rats and mice have been conducted with doxylamine succinate. Doxylamine succinate is not likely to have human carcinogenic potential. The carcinogenic potential of pyridoxine hydrochloride has not been evaluated. 14 CLINICAL
A double-blind, randomized, multi-center, placebo-controlled study was conducted to support the safety and efficacy of DICLEGIS in the treatment of nausea and vomiting of pregnancy. Adult women 18 years of age or older and 7 to 14 weeks gestation (median 9 weeks of gestation) with nausea and vomiting of pregnancy were randomized to 14 days of DICLEGIS or placebo. Two tablets of DICLEGIS were administered at bedtime on Day 1. If symptoms of nausea and vomiting persisted into the afternoon hours of Day 2, the woman was directed to take her usual dose of two tablets at bedtime that night and, beginning on Day 3, to take one tablet in the morning and two tablets at bedtime. Based upon assessment of remaining symptoms at her clinic visit on Day 4 (± 1 day), the woman may have been directed to take an additional tablet mid-afternoon. A maximum of four tablets (one in the morning, one in the mid-afternoon and two at bedtime) were taken daily. Over the treatment period, 19% of DICLEGIS-treated patients remained on 2 tablets daily, 21% received 3 tablets daily, and 60% received 4 tablets daily. The primary efficacy endpoint was the change from baseline at Day 15 in the Pregnancy Unique-Quantification of Emesis (PUQE) score. The PUQE score incorporates the number of daily vomiting episodes, number of daily heaves, and length of daily nausea in hours, for an overall score of symptoms rated from 3 (no symptoms) to 15 (most severe). At baseline, the mean PUQE score was 9.0 in the DICLEGIS arm and 8.8 in the placebo arm. There was a 0.7 (95% confidence interval 0.2 to 1.2 with p-value 0.006) mean decrease (improvement in nausea and vomiting symptoms) from baseline in PUQE score at Day 15 with DICLEGIS compared to placebo (see Table 6).
Table 6 – Change from Baseline in the Primary Endpoint, Pregnancy Unique-Quantification of Emesis (PUQE) Score at Day 15. (Intent-to-Treat Population with Last-Observation Carried Forward) PUQE Score* Doxylamine Succinate + Treatment Difference Pyridoxine Hydrochloride [95% Confidence Interval] Baseline Change from baseline at Day 15
*The Pregnancy-Unique Quantification of Emesis and Nausea (PUQE) score incorporated the number of daily vomiting episodes, number of daily heaves, and length of daily nausea in hours, for an overall score of symptoms rated from 3 (no symptoms) to 15 (most severe). Baseline was defined as the PUQE score completed at the enrollment visit. 16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How supplied
DICLEGIS delayed-release tablets are supplied in a high-density polyethylene bottle with a polypropylene child-resistant cap and a silica gel desiccant canister. Each white, round, film-coated, delayed-release tablet contains 10 mg doxylamine succinate and 10 mg pyridoxine hydrochloride, and is imprinted on one side with the pink image of a pregnant woman. DICLEGIS tablets are provided as follows: NDC 55494-100-10 Bottles of 100. 16.2 Storage and Handling Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C and 30°C (59°F and 86°F) [see USP Controlled Room Temperature]. Keep bottle tightly closed and protect from moisture. Do not remove desiccant canister from bottle. 17 PATIENT COUNSELING INFORMATION
See FDA-approved patient labeling (Patient Information) 17.1 Somnolence and Severe Drowsiness
Inform women to avoid engaging in activities requiring complete mental alertness, such as driving or operating heavy machinery, while using DICLEGIS until cleared to do so. Inform women of the importance of not taking DICLEGIS with alcohol or sedating medications, including other antihistamines (present in some cough and cold medications), opiates and sleep aids because somnolence could worsen leading to falls or other accidents. DICLEGIS® is a registered trademark of Duchesnay Inc. U.S. Patent Nos. 6,340,695 & 7,560,122. Distributed by: Duchesnay USA, Inc. Bryn Mawr, PA, 19010 Tel: 1-855-722-7734 Fax: 1-888-588-8508 www.duchesnayusa.com 2013, Duchesnay Inc. All rights reserved.
Indian Journal of Pharmacy Practice Association of Pharmaceutical Teachers of India A Prospective Study on Adverse Drug Reactions in a Tertiary Care South Indian Hospital Palanisamy S*, ArulKumaran KSG, Rajasekaran A Department of Pharmacy Practice, KMCH College of Pharmacy, Coimbatore-48 A B S T R A C T Submitted: 25/03/2013 Accepted: 17/06/2013 Background: ADRs have a maj
A hyperglycaemia kezelése 2-es típusú diabetes mellitusban – kivonat az Amerikai és az Európai Diabetes Társaság (ADA és EASD) konszenzus nyilatkozatából A klasszikus orális antidiabetikumok és inzulinkészítmények mellett az utóbbi években számos új antidiabetikum jelent meg, mely amellett, hogy szélesíti a terápiás lehetőségek palettáját, meg is neh