Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Femoroplasty: a new option for femur metastasis
Ricardo Plancarte-Sanchez, MD, FIPP*; Jorge Guajardo-Rosas, MD†; Oscar
Cerezo-Camacho, MSc‡; Faride Chejne-Gomez, MD†; Francisco Gomez-Garcia,
MD§; Abelardo Meneses-Garcia, PhD¶; Cristopher Armas-Plancarte, MD†;
Gustavo Saldan˜a-Ramirez, BSN†; Roberto Medina-Santillan, PhD**
*Escuela Superior de Medicina, Postgraduate Division, Instituto Politecnico Nacional. Pain
Clinic and Palliative Care Department, Instituto Nacional de Cancerologia, Mexico City;
†Staff of Pain Clinic and Palliative Care, Instituto Nacional de Cancerologia, Mexico City;
‡Medical Sciences Researcher, Clinical Research Department, Instituto Nacional de Cancerolo-
gia, Mexico City; §Orthopaedics and Trauma Department, Instituto Nacional de Cancer-
ologı´a, Mexico City; ¶Escuela Superior de Medicina, Postgraduate Division, Instituto
Politecnico Nacional, Mexico City; **Department of Research and Postgraduate studies, Escu-
ela Superior de Medicina, Instituto Polite´cnico Nacional, Mexico City, Mexico
n Abstract: Bone metastases are very frequent in patients
the consolidation of the microfractures because of bone
with cancer and usually are located in the patient’s long
bones and spine. Various approaches to pain relief and sta-bility to the affected bone have been used. The aim of the
study is to report our experience with a new minimally
polymethylmethacrylate cement, bone metastases, femur,
invasive percutaneous technique in patients with bone
metastases located in the head, neck, and proximal femur. The technique is performed under fluoroscopic guidancethrough the application of polymethylmethacrylate bone
cement. Our descriptive, retrospective, longitudinal caseseries included 15 patients who underwent femoroplasty.
Bone metastasis is a frequent condition in patients with
All patients reported pain reduction and improved mobil-
cancer. Its incidence depends on the primary tumor
ity, with no complications observed. The femoroplasty pro-
type. It develops in up to 50% of patients with cancer,
cedure caused pain relief by stabilizing the bone through
most frequently breast, prostate, and lung cancers. Approximately 1.5 million new cancer cases are
Address correspondence and reprint requests to: Ricardo Plancarte-
reported each year.1 The most frequent symptom is
Sa´nchez, MD, FIPP, Av. San Fernando 22, Col. Seccio´n XVI, 14060 MexicoCity, Mexico. E-mail: [email protected]
pain, which is severe and as a result produces altera-
Submitted: July 12, 2011; Revision accepted: June 27, 2012
tions in mobility. This has repercussions on the muscu-
loskeletal system and therefore on quality of life.2–4The vast majority of cancer patients with bone metasta-
ses are in advanced stages of their disease. Some of
Pain Practice Ó 2012 World Institute of Pain, 1530-7085/12/$15.00Pain Practice, Volume ••, Issue •, 2012 ••–••
these metastatic bone lesions involve long bones such
as the femur, but there are few studies examining mini-
obturator artery is divided into 2 types as well, the
mally invasive treatments for these areas. Therefore,
anterior and posterior. In the second plane, the mus-
our primary goal in this study was to examine whether
cles passing nearby are the tensor of fascia lata and
such a therapy would improve quality of life and reduce
pain in individuals with metastatic cancer to the femur.
In the third plane, we find the medial and lateral
Existing treatments for this kind of patient include
region of the greater trochanter of femur, between the
surgery, radiation therapy, chemotherapy, hormonal
meeting point of the gluteus medius and vastus medial-
therapy, and the use of bisphosphonates. Of these,
radiation remains the treatment of choice. Commonly,pharmacological handling by itself does not control
pain adequately in these patients5; for this reason, it isnecessary to use a multimodal therapy that can offer a
The Ethics Committee of the Instituto Nacional de
better option of integral palliation.
Cancerologia (IRB) approved this retrospective obser-
To provide pain relief and offer stability to the
vational case series. Informed consent was obtained
affected bone, physicians have been looking for new
prior to intervention. Fifteen patients with metastatic
minimally invasive techniques to approach these bone
disease of the femur were treated at the Instituto Nac-
metastases, such as vertebroplasty. Vertebroplasty
ional de Cancerologia, Mexico City, from November
consists of the application of bone cement to a com-
2004 through December 2007. Inclusion criteria were
pression fracture within the vertebral body, which
as follows: (1) patients with primary malignancy of
produces substantial pain relief in 80–90% of the
lung, breast, and prostate and metastatic lesions in the
cases, with low morbidity. 6–11 Likewise, patients
head, neck, and proximal one-third of the femur and
who were treated with the application of bone
(2) Karnofsky score >60%. Exclusion criteria were as
cement—under fluoroscopic or tomographic guid-
follows: (1) impairment of coagulation and platelet
ance—reported 90% of pain relief in different parts
dysfunction; (2) local infection at the proposed proce-
of the skeletal system such as tibia, pelvis, as well as
dure site; and (3) cognitive dysfunction.
several support points in the acetabulum, ilium, and
Outcome measures were visual analog scale (VAS) rat-
sacrum. 12–19 At the femoral level, when the polym-
ing, use of opioid and nonopioid pain medication, and
ethylmethacrylate (PMMA) bone cement is used, it
changes in function as measured by mobility. All patients
solidifies and permits stabilization of the bone struc-
were previously evaluated using the following studies:
ture and coxofemoral articulation. A lytic activity is
elevation of alkaline phosphatase, bone scanning, pelvis
originated as a consequence of the thermal action
and affected hip X-ray, and pelvis MRI in some cases.
produced by the cement, reducing the metastatic
Depending on the progression of their disease, some
activity, and it is suggested that this probably inhib-
patients were receiving chemotherapy, radiotherapy, and
its the regional nociceptors, thus alleviating pain, as
both opioids and nonsteroidal anti-inflammatory drugs
(NSAID) without satisfactory results.
The objective of this study was to investigate a new,
minimally invasive, fluoroscopically guided, percutane-
ous technique called ‘‘femoroplasty’’ in patients withmetastatic disease in the head, neck, and proximal
The patients’ blood pressure, pulse oximetry, and ECG
were monitored continuously during the procedure;conscious sedation was achieved with fentanyl, propo-fol, and midazolam. One gram of IV cephalosporin was
administered for prophylaxis prior to starting the pro-
When performing femoroplasty, it is necessary to
cedure. Using fluoroscopy, the patients’ pelvis and
have good knowledge of the anatomical planes
involved hip were imaged in the anteroposterior posi-
tion. The patient was then placed in the lateral decub-
described: In the first plane, the skin is innervated by
itus position with the affected side up and the hip
the lateral femoral cutaneous nerve and vascularized
slightly flexed. Using sterile technique, the area was
by the superior gluteal artery. The superior gluteal
then prepped, and the fluoroscopy machine was ori-
artery is divided into 2 types, superior and deep. The
ented so that the needle entry site could be lateral to the
Figure 1. Lateral view of the femur with 22-gauge needles
Figure 2. Correct position of the needle in AP view.
placed on both sides; bone biopsy needle located in the middleof the greater trochanter.
through the greater trochanter until its tip reached the
femur with a craniocaudal angle varying from 20 to 30
junction of the anterior and medial third of the femoral
degrees. The C-arm was rotated until the femoral neck
head. Once the biopsy needle was properly placed by this
and head could be visualized and the greater trochanter
maneuver, the spinal needle was removed and the intro-
appeared as an oval (tunnel view). The procedure site
duction of the biopsy needle continued (Figure 3).
was infiltrated with 2% lidocaine, and two 22-gauge
Once the biopsy needle was placed adequately in
needles were placed for reference between the neck and
the femoral head, its location was verified with 3 mL
head of the femur. An 11-gauge bone biopsy needle was
of nonionic contrast to evaluate the filling pattern and
then placed in the middle and upper area of the greater
identify leaks into the articular space, veins, or muscle.
trochanter between the 2 spinal needles directed toward
If necessary, the needle was repositioned. Subse-
the femoral head and a third needle in the center. These
quently, we administrated the PMMA, using fluoro-
needles are essential to locate the femur, depth, and tra-
scopic guidance in the lateral view using real-time
jectory of the biopsy needle (Figure 1). Once the biopsy
needle touched bone, it was then advanced across the
Polymethylmethacrylate preparation: the PMMA
cortical region of the trochanter using both lateral and
was mixed to a semiliquid consistency and drawn up
tunnel views for guidance (Figure 2).
into 1-mL syringes. Administration of the PMMA was
A 22-gauge long spinal needle was passed through the
performed under fluoroscopic imaging in the AP and
biopsy needle as a guide before advancing the biopsy
lateral view. To achieve satisfactory filling of the
needle toward the femoral head; this reduced the possi-
affected bone, the needle should be withdrawn while
bility of needle deviation. The advancement of the spinal
delivering the cement, directing the bevel of the needle
needle was sometimes complicated by bone hardening.
toward the site that requires more filling (Figures 5A
In this circumstance, the biopsy needle was advanced
and 5B). The quantity of PMMA varies depending on
Figure 3. The biopsy needle advanced through the femoralhead with the tip between the anterior and medial thirds.
Figure 5. (A) AP VIEW: PMMA application; (B) view of the pro-cedure’s final step.
PMMA, polymethylmethacrylate; VAS, visual analog scale; Mets source, origin of themetastasis.
the extent of the metastatic lesion and patient size. Filling should be stopped once the distribution of
Figure 4. Lateral view to verify PMMA distribution.
cement in the metastatic area has been achieved.
to be multifactorial. The injection of bone cement mayaid in the stabilization of microfractures, reduce thermaldamage, and reduce cytotoxicity in bones. Furthermore,the antineoplastic effect of bone cement may play a sig-nificant role in treating osteolysis.22,23 The present studydemonstrated a sustained effect on pain relief (decreasedVAS score) at femoral level across PMMA use, withimprovement in function and pain (WOMAC score.)
Our study did not find any serious complications,
perhaps because of the femoral characteristics (longbone, size, easy approach) in our study population.
The literature mentions potential complications infemoroplasty,
We performed 17 femoroplasties in 15 patients (2
cement leakage, nerve and vascular injury, persistent
bilateral): 8 women (mean age 42.6 ± 12.6), 2 with
pain, incident fracture after cementoplasty, rejection to
lung cancer and 6 with breast cancer, and 7 men
PMMA, and avascular necrosis of femoral head by
(mean age 62.8 ± 13.8), 6 with prostate cancer and 1
cement leakage to the circumflex artery. Three previ-
with lung cancer (Table 1). The distribution of affected
ous case series had been reported without detailed
sides was as follows: 10 right sides and 7 left sides of
affected femur in 15 patients. The mean volume of
One previous series reported 11 patients who pre-
sented with osteolytic lesions and severe pain (none of
whom were treated with previous radiotherapy), and 5
patients more than 50% compared with baseline levels
patients presented with fracture at the femoral neck or
and was maintained throughout follow-up (ANOVA
trochanter. The author used a greater volume of injec-
repeated measures P < 0.01). Moreover, 15 sides saw
tion than our study of PMMA (up to 30 mL) and
improvement according to Western Ontario and
found a clinical improvement in pain relief without
McMaster Universities Osteoarthritis Index (WO-
any information regarding statistical significance.24 In
MAC) score, while only 2 reached slight improvement
our study, every patient was treated with radiotherapy
(standard medical therapy for bone metastases) and
Baseline mean VAS score for pain was 5.6 ± 1.1.
pharmacologic treatment. They presented with signifi-
Pain was localized in the affected pelvic member. Post-
cant pain and functional impairment. The technique
procedure VAS was 1.2 ± 2.3, remaining at the same
presented in our study seems easier than Kang’s tech-
level throughout the follow-up of 2 months (t-test
nique, in spite of the fact that we used only one bone
[basal vs. following measures] and ANOVA repeated
biopsy needle and we did not use special tools, for
measures <0.001) (Figure 6). All patients reported pain
reduction on the treated pelvic member and improved
The other 2 case series reported one and 2 cases,
mobility; however, analgesic intake was not modified
respectively. The case report used cementoplasty at the
because of patients’ pathology. There were no compli-
femoral head with optimal pain relief. The author used
cations observed, but 3 patients presented with tran-
a double approach (neck and acetabulum) with the
sient pain that improved 10 days after the procedure.
patient in prone position.25 We consider prone posi-tion a more difficult position than lateral decubitus.
The lateral decubitus position allowed us to visualizethe AP and lateral views of femur in a better way.
Polymethylmethacrylate use at sites of bone metastases
It also allowed us to modify the angle to obtain a
resulted in improved function, pain relief, and health-
coaxial or tunnel vision view. The lateral decubitus
related quality of life. The use of PMMA at sites other
approach resides in the middle of greater trochanter,
than the vertebrae is a novel, interventional approach
consequently allowing us to use only one needle to
that may be used to potentially reduce pain and improve
patient function. The mechanisms of bone cement–
The last report took into account 2 cases of femur
induced analgesia and functional improvement are likely
cementoplasty. In both patients, the author found
improvement in pain relief; however, one had a pathologic
8. Galibert P, Deramond H, Rosat P, Le Gars D. Prelimin-
fracture in the treated area, and in the other, the
ary note on the treatment of vertebral angioma by percutane-
patient did not improve in functionality.26 In contrast,
ous acrylic vertebroplasty. Neurochirurgie 1987;33:166–168.
we did not have pathologic fracture postprocedures.
9. O’Brien J, Sims J, Evans A. Vertebroplasty in patients
with severe vertebral compression fractures: a technical
We observed improved WOMAC scores in every
report. AJNR Am J Neuroradiol 2000;21:1555–1558.
10. Amar A, Larsen D, Esnaashari N, Albuquerque FC,
Adequate pre-, intra-, and postprocedure evalua-
Lavine SD, Teitelbaum GP. Percutaneous transpedicular
tions of the patient are necessary. The venography
PMMA vertebroplasty for the treatment of spinal compres-
procedure is an important tool that allows us to ade-
sion fractures. Neurosurgery 2001;49:1105–1115.
quately fill the lesion and detect potential leakage
11. Weill A, Chiras J, Simon JM, Rose M, Sola-Martinez
into the vasculature. PMMA bone cement should be
T, Enkaoua E. Spinal metastases: indications for and resultsof percutaneous injection of acrylic surgical cement. Radiol-
confined to the area of bone defect. Because of the
high temperature reached during the hardening pro-
12. Kelekis A, Lovblad K, Mehdizade A, et al. Pelvic
cess, the cement can cause thermal necrosis and pro-
osteoplasty in osteolytic metastases: technical approach
duce a dysfunction in nociceptors. It can also achieve
under fluoroscopic. Guidance and early clinical results.
analgesia and stabilize the bone through the consoli-
J Vasc Interv Radiol 2005;16:81–88.
dation of the microfractures in the affected lower
13. Marcy PY, Palussie`re J, Descamps B, et al. Percutane-
ous cementoplasty for pelvic bone metastasis. Support Care
Drawbacks to this study include a retrospective and
14. Hokotate H, Baba Y, Churei H, Nakajo M, Ohkubo
nonuniform case series format, which is inherently
K, Hamada K. Pain palliation by percutaneous acetabular
flawed and subject to reporting bias. Future study will
osteoplasty for metastatic hepatocellular carcinoma. Cardio-
clarify the exact indications and outcomes of this tech-
vasc Intervent Radiol 2001;24:343–346.
nique. In spite of these problems, we suggest this pro-
15. Cotten A, Deprez X, Migaud H, Chabanne B, Du-
cedure may be best for those patients presenting with
quesnoy B, Chastanet P. Malignant acetabular osteolyses:
Karnofsky performance scores over 60%, with pain on
percutaneous injection of acrylic bone cement. Radiology
the affected pelvic extremity, and whose physical activ-
ities present risk of fractures of the femoral bone, a sit-
16. Kelly C, Wilkins R, Eckardt J, Ward W. Treatment of
metastatic disease of the Tibia. Clin Orthop Relat Res
uation that rapidly deteriorates their quality of life.
17. Harris K, Pugash R, David E, et al. Percutaneous
cementoplasty of lytic metastasis in left acetabulum. Curr
1. Jemal A, Siegel R, Ward E, et al. Cancer statistics,
18. Mercy P, Palussiere J, Descamps B, et al. Percutane-
2007. Cancer CA Cancer J Clin 2007;57:43–66.
ous cementoplasty for pelvis bone metastasis. Support Care
2. Schaefer O, Lohrmann C, Herling M, Uhrmeister P,
Langer M. Combined radiofrequency thermal ablation and
19. Swanson KC, Pritchard DJ, Sim FH. Surgical treat-
percutaneous cementoplasty treatment of a pathologic frac-
ment of metastatic disease of the femur. J Am Acad Orthop
ture. J Vasc Interv Radiol 2002;13:1047–1050.
3. Perrin RG, Laxton AW. Metastatic spine disease: epi-
20. Deramond H, Wright NT, Belkoff SM. Temperature
demiology, pathophysiology, and evaluation of patients.
elevation caused by bone cement polymerization during ver-
Neurosurg Clin N Am 2004;15:365–373.
tebroplasty. Bone 1999;25:S17–S21.
4. Coleman RE. Clinical features of metastatic bone dis-
21. Netter FH. Lower Limb. En: Atlas of Human Anat-
ease and risk of skeletal morbidity. Clin Cancer Res
omy, 4th ed. Philadelphia: Saunders, Elsevier Inc; 2006.
22. Baroud G, Samara M, Steffen T. Influence of mixing
5. Fallon M, McConnell S. The principles of cancer pain
method on the cement temperature-mixing time history and
management. Clin Med 2006;6:136–139.
doughing time of three acrylic cements for vertebroplasty.
6. Tschishart C, Finkelstein J, Whyne C. Optimization
J Biomed Mater Res B Appl Biomater 2004;68:112–116.
of tumor volume reduction and cement augmentation in per-
23. Belkoff SM, Molloy S. Temperature measurement
cutaneous vertebroplasty for prophylactic treatment of spinal
during polymerization of polymethylmethacrylate cement
metastases. J Spinal Disord Tech 2006;19:584–590.
used for vertebroplasty. Spine (Phila Pa 1976) 2003;28:
7. Fourney DR, Schomer DF, Nader R, et al. Percutane-
ous vertebroplasty and kyphoplasty for painful vertebral body
fractures in cancer patients. J Neurosurg 2003;98:21–30.
metastasis to the femoral neck using percutaneous hollow
perforated screws with cement augmentation. J Bone Joint
26. Yamada K, Matsumoto Y, Kita M, et al. Clinical out-
come of percutaneous osteoplasty for pain caused by meta-
25. Wang WG, Wu CG, Gu YF, Li MH. Percutaneous
static bone tumors in the pelvis and femur. J Anesth
osteoplasty for the management of a femoral head metasta-
sis: a case report. Korean J Radiol 2009;10:641–644.
410-121-0030 Practitioner-Managed Prescription Drug Plan (PMPDP) (1) The Practitioner-Managed Prescription Drug Plan (PMPDP) is a plan that ensures that fee for service clients of the Oregon Health Plan shall have access to the most effective prescription drugs appropriate for their clinical conditions at the best possible price: (a) Licensed health care practitioners (informed by the latest
Experienta in Pastel Group Dana conduce activitatile financiare si administrative ale grupului. Felul in care manageriaza relatia cu furnizorii externi asigura grupului un avantaj competitiv considerabil: un raport calitate-pret foarte corect. Pe de alta parte, Dana asigura analiza si evaluarea performantelor membrilor echipei, raportate la planificarea financiara a com
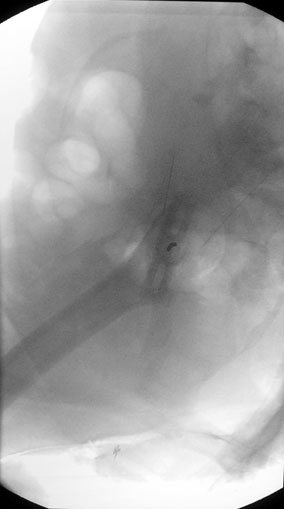
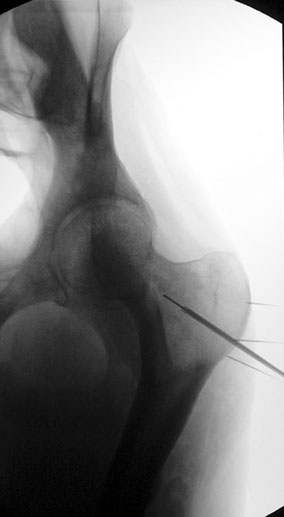 Figure 1. Lateral view of the femur with 22-gauge needles
Figure 2. Correct position of the needle in AP view.
Figure 1. Lateral view of the femur with 22-gauge needles
Figure 2. Correct position of the needle in AP view.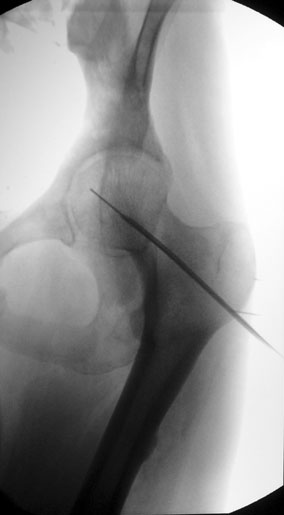
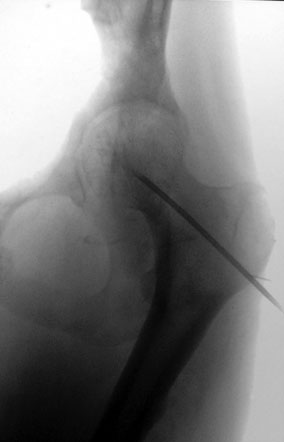
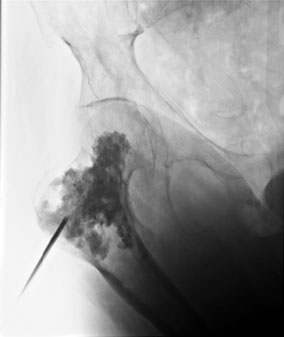
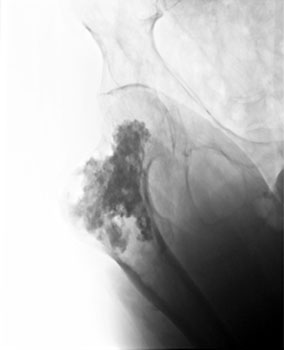 Figure 3. The biopsy needle advanced through the femoralhead with the tip between the anterior and medial thirds.
Figure 3. The biopsy needle advanced through the femoralhead with the tip between the anterior and medial thirds.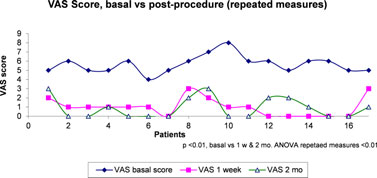 to be multifactorial. The injection of bone cement mayaid in the stabilization of microfractures, reduce thermaldamage, and reduce cytotoxicity in bones. Furthermore,the antineoplastic effect of bone cement may play a sig-nificant role in treating osteolysis.22,23 The present studydemonstrated a sustained effect on pain relief (decreasedVAS score) at femoral level across PMMA use, withimprovement in function and pain (WOMAC score.)
Our study did not find any serious complications,
perhaps because of the femoral characteristics (longbone, size, easy approach) in our study population.
to be multifactorial. The injection of bone cement mayaid in the stabilization of microfractures, reduce thermaldamage, and reduce cytotoxicity in bones. Furthermore,the antineoplastic effect of bone cement may play a sig-nificant role in treating osteolysis.22,23 The present studydemonstrated a sustained effect on pain relief (decreasedVAS score) at femoral level across PMMA use, withimprovement in function and pain (WOMAC score.)
Our study did not find any serious complications,
perhaps because of the femoral characteristics (longbone, size, easy approach) in our study population.