Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients cialis uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Chrisnutting-oncology.co.uk
The British Journal of Radiology, 78 (2005), 405–410
E 2005 The British Institute of Radiology
Management of non-Hodgkin’s lymphoma of the thyroid: theRoyal Marsden Hospital experience
1,2K J HARRINGTON, MRCP, FRCR, 1V J MICHALAKI, MD, 3L VINI, FRCR, 1,2C M NUTTING, MD, MRCP, FRCR,1K N SYRIGOS, MD, 4R A’HERN, PhD and 3C L HARMER, FRCP, FRCR
1Head and Neck Cancer Unit, Royal Marsden Hospital, Fulham Road, London, 2Institute of Cancer Research, FulhamRoad, London, 3Thyroid Unit, Royal Marsden Hospital, Fulham Road, London and 4Department of Statistics, RoyalMarsden Hospital, Fulham Road, London, UK
Abstract. A retrospective review was conducted of patients treated for thyroid non-Hodgkin’s lymphoma(TNHL) at the Royal Marsden Hospital between 1936 and 1996 to determine the effect of radiotherapy (RT) onoutcome. 91 patients were identified from the Thyroid Unit Database. There were 77 females and 14 males witha median age of 65 years (range 22–87 years). RT was delivered according to two separate policies: (1) involvedfield radiotherapy (IFRT) to the thyroid bed and cervical lymph nodes; (2) extended field radiotherapy (EFRT)covering the thyroid bed, cervical and mediastinal lymph nodes. 89 patients received RT as part of definitivetreatment following surgery, to a dose of approximately 40 Gy. 25 patients received IFRT and 64 patientsEFRT. 27 patients received cytotoxic chemotherapy. 18 patients (72%) treated with IFRT died of TNHL with amedian relapse free survival (RFS) of 10 months and a median overall survival (OS) of 21 months. In contrast,only 29 patients (46%) treated with EFRT died of TNHL with a median RFS of 76 months (p50.01 for RFSwith respect to IFRT and p50.04 for OS). Significantly more patients treated with IFRT relapsed locally (52%vs 27%). There was no difference in the rates of systemic relapse (20% vs 22%). EFRT alone for Stage I, but notfor Stage II disease, yielded acceptable rates of local control and disease free survival with doses of at least40 Gy. These historical data strongly support the addition of combination chemotherapy to the treatmentregimen in all patients with Stage II disease. Indeed, in recent years this has become the standard of care for allcases of thyroid lymphoma unless the histology is of marginal zone type (mucosa associated lymphoma tissue(MALT) lymphoma).
Thyroid non-Hodgkin’s lymphoma (TNHL) is an
shift towards using a combination of chemotherapy and
uncommon tumour, representing 2–8% of thyroid malig-
RT in all cases other than mucosa associated lymphoma
nancies and approximately 1–2% of extranodal lympho-
tissue (MALT) lymphoma of the thyroid gland. As
mas [1–4]. It occurs most frequently in elderly females and
regards therapeutic irradiation, there remain a number
has been linked to Hashimoto’s thyroiditis and prior
of unresolved issues regarding the volume of tissue that
therapeutic irradiation of the thyroid bed. Staging should
should be treated and the dose prescription required.
include CT scanning of the neck, thorax, abdomen and
There are two main options in the selection of radiation
pelvis, together with bone marrow aspirate and trephine
treatment fields: (1) involved field RT (IFRT) which aims
to include the entire thyroid gland and local neck nodes;
There exists no universally accepted standard of care for
and (2) extended field RT (EFRT) which involves treating
TNHL and a number of controversies exist regarding the
the thyroid, neck, mediastinal and in some centres, axillary
roles of surgery, radiotherapy (RT) and chemotherapy in
the management of this disease [5–12]. Previously, surgery
These two options have never been formally compared
occupied a pre-eminent place in management and most
in a randomized study and in view of the rarity of this
patients underwent extensive resections. In recent years,
condition; such a study is unlikely to be conducted. A a
however, the appreciation that TNHL is sensitive to RT
result, the choice between IFRT and EFRT has been a
and chemotherapy has resulted in a move towards limited
matter of clinical judgement based on prior experience.
surgical intervention, usually in the form of a diagnostic
Similarly, formal evaluation of the optimal radiation
biopsy followed by definitive RT (or chemotherapy
dose required for local control has never been undertaken.
followed by RT). However, there are opponents of this
In line with treatment of nodal and non-thyroid extra-
view who recommend excision or debulking of disease
nodal NHL, most patients with TNHL have received
followed by post-operative RT [13–22].
doses in the order of 40 Gy. Previous studies have
In spite of the controversy regarding the surgical
suggested that there is a threshold dose below which the
management of TNHL, radical RT became the treatment
chance of achieving local control is small. Tupchong et al
of choice in most centres, although there has now been a
[23] reported 0% local control rated for patients whoreceived less than 20 Gy. Therefore, in this retrospectiveanalysis, we have attempted to address these twoimportant questions relating to the management of
Received 27 February 2004 and in revised form 28 October 2004,accepted 6 December 2004.
The British Journal of Radiology, May 2005
K J Harrington, V J Michalaki, L Vini et al
Table 1. Summary of patient characteristics for 91 patientswith thyroid non-Hodgkin’s lymphoma
A search of the Royal Marsden Hospital (RMH)
Thyroid Database was undertaken for a period that
spanned the years between 1936 and 1996.
This database contains a thorough summary of over
2000 patients presenting to RMH with thyroid malignancy
over the last six decades. A total of 91 patients with
histologically proven NHL were identified. Case notes
were reviewed in order to collect demographic data, details
of disease-related symptoms and tumour stage, surgical
and radiotherapeutic management and standard outcome
measures, including relapse free (RFS) and overall survival
(OS). For the purposes of data collection, the results of
staging investigations were accepted at face value and noattempt was made to re-evaluate the staging assigned topatients treated at different times. Similarly, the patholo-
gical classification of NHL has undergone a number of
The presenting symptoms are documented in Table 1.
changes during the period of time under study [24–29]. In
For two patients, no presenting symptoms were recorded
a previous study of 46 patients with TNHL from RMH,
but the vast majority (98%) presented with neck swelling.
all of whom are included in this analysis, it was shown that
Local obstructive symptoms (stridor, dysphagia and
the majority (91%) presented with adverse (intermediate or
high grade) histology. Similar findings were apparent for
number (34%) had previously been noted to have goitre,
this group of patients. No attempt has been made to
review previous pathological specimens or re-classify casesaccording to the current REAL classification. Of the 91
patients who were identified, 89 were eligible for analysis
In keeping with data presented for other studies, the
of the effect of definitive RT. The two patients excluded,
majority of patients presented with early stage disease. 35
received primary chemotherapy without RT.
had Stage I disease confined to the thyroid gland and 49had Stage II disease. Only seven patients, were found tohave more advanced Stage III or IV disease at presenta-
tion. From analysis of the database, it was apparent thatthese patients presented with massive thyroid enlargement
Follow-up data were obtained for all patients treated
and evidence of dissemination, rather than as patients with
with RT. RFS and OS times were calculated for each
widely disseminated lymphoma with incidental involve-
patient to the nearest month, taken from the time of
ment of the thyroid gland. Systemic B symptoms were
presentation to the time of first relapse (for RFS) or death/
uncommon, occurring in only two patients.
All of the patients underwent an initial surgical
procedure, the details of which are presented in Table 2.
Statistical analysis was performed using the Statistical
Package for the Social Sciences (SPSS, Inc., Chicago, IL),
statistical software. Survival curves were obtained by the
Over the 60 year period in which patients were treated, a
Kaplan-Meier method and comparisons were made with
number of different treatment protocols were applied
the log-rank statistics. Factors found to be significant at
involving use of 220–250 kV X-rays, 60Co gamma rays and
univariate analysis were considered for multivariate
4–6 MV photons. The median tumour radiation dose was
analysis. Cox proportional hazards models were developed
40 Gy (range 4–72 Gy), which was delivered at a dose rate
for the multivariate analysis of survival and any value of
of between 1.2 Gy and 2.3 Gy per day.
p,0.05 was considered to be statistically significant.
Table 2. Initial surgical procedure performed on the 91
patients with thyroid non-Hodgkin’s lymphoma
The median age of the patients was 65 years (range 22–
87 years). There was no significant difference between the
median ages of the female (median 65 years, range 27–87
years) and male (median 63 years, range 22–85 years)
patients. There were 77 females and 14 males, representing
The British Journal of Radiology, May 2005
The majority (61 of 89) received a radiation dose of
Table 3. Significant factors on univariate analysis of overall
40 Gy or more. Treatment was usually delivered using
parallel-opposed anterior and posterior fields, although,
direct anterior, anterior oblique or lateral fields wereemployed occasionally. Spinal cord shielding was not used.
No attempt has been made to assess the effect of technique
on outcome. 25 patients received IFRT to the thyroid bed
and cervical lymph nodes and 64 patients received EFRT
to the thyroid bed, cervical and mediastinal lymph nodes.
In this latter group, there were no data detailing the
number of patients in whom the superior mediastinal
nodes, as opposed to all mediastinal nodes, were treated.
The axillary nodes were not treated routinely.
27 patients received cytotoxic chemotherapy under a
wide variety of circumstances. Two received definitive
IFRT, involved field radiotherapy; EFRT, extended field radio-
combination chemotherapy without RT. Five patients
received induction chemotherapy prior to radical RT, eightreceived adjuvant chemotherapy following RT and 14
The type of surgical procedure performed had a significant
received chemotherapy following relapse after RT. Clearly,
impact on the outcome of subsequent RT as demonstrated
this experience reflects the state of what was considered
optimal practice at the time that the patients presented. Incurrent practice, it is likely that the majority of patientswould receive combination chemotherapy followed by
18 of 25 patients (72%) treated with IFRT died of
Regimens comprised cyclophosphamide, vincristine and
TNHL. The median RFS was only 10 months and the
prednisolone (COP), cyclophosphamide, doxorubicin, vin-
median OS was 21 months. In contrast, only 29 of 64
patients (45%) treated with EFRT died of TNHL. The
mitoxantrone, cyclophosphamide, etoposide, bleomycin
median RFS was 76 months, while the median OS has not
and vincristine (PMitCEBO). Analysis of the role of
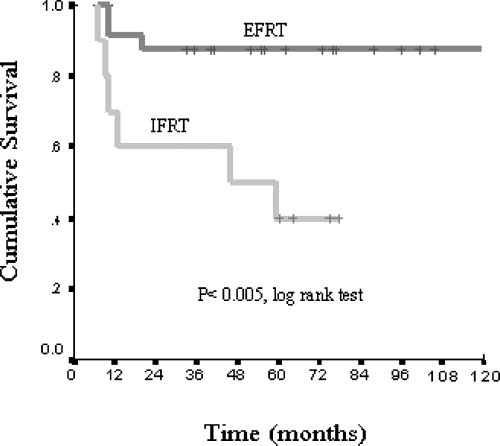
yet been reached. The 5-year survival data according to
chemotherapy in this cohort of patients was not possible
disease stage stratified by radiation field (IFRT or EFRT)
because of the small numbers and the different regimens
are illustrated in Figures 1 and 2. Patients who received
employed. Eight of 13 patients treated initially with
EFRT had higher survival rates (p,0.005), (log rank test).
chemotherapy as part of a planned combined approach
For patients treated with IFRT, 52% (20% local alone and
were long-term survivors. However, results for relapsed
32% combined local and distant) had evidence of loco-
disease were generally poor, with only two of eight
regional failure at the time of death, compared with only
patients relapsing after RT successfully salvaged with
26% (9% local alone plus 17% local and distant), of patients
treated with EFRT. There was no significant difference inthe rates of local control between two groups (20% forIFRT vs 22% for EFRT). The patterns of failure of patients
dying following IFRT and EFRT are detailed in Table 5.
The overall 5-year survival rate was 48%, with a median
RFS of 34 months. Univariate analysis of OS according to
patient variables and treatment factors is shown in
When the survival data for patients who received
Table 3. Adverse prognostic factors were as follows:
,40 Gy were compared with those who received 40 Gy
advanced stage, surgical procedure (only biopsy vs moredebulking procedure), extent of radiation field, radiation
Table 4. Significant independent factors on multivariate analy-
dose of 40 Gy or more, and the presence of stridor at
diagnosis. A number of these factors have been implicatedpreviously [29–32]. Analysis of the effect of dysphagia,
dysphonia and previous goitre on the OS revealed no
significant impact. Independent predictive factors obtained
from multivariate analysis are shown in Table 4.
Analysis of the extent of surgical resection (biopsy alone
vs more extensive resection), revealed that only in the last
decade was there a marked change towards less extensive
procedures. Thus, prior to 1990 biopsy was performed in
30 patients compared with 43 who underwent an extensiveresection. After 1990, 13 patients underwent biopsy
IFRT, involved field radiotherapy; EFRT, extended field radio-
compared with only 5 who had a more extensive resection.
The British Journal of Radiology, May 2005
K J Harrington, V J Michalaki, L Vini et al
Table 5. Survival according to stage of disease and extent ofirradiated volume
IFRT, involved field radiotherapy; EFRT, extended field radio-
Analysis of the data from this large series of patients
with TNHL treated over a prolonged period of time in asingle centre provides valuable insights in to the manage-ment of this uncommon disease. RT has traditionallyplayed a major role in treatment of TNHL and thefindings of this study have direct bearing on its use. Multivariate analysis has highlighted the extent ofradiation field as an independent prognostic factor. RFS
Figure 1. Kaplan-Meier curve showing overall survival of
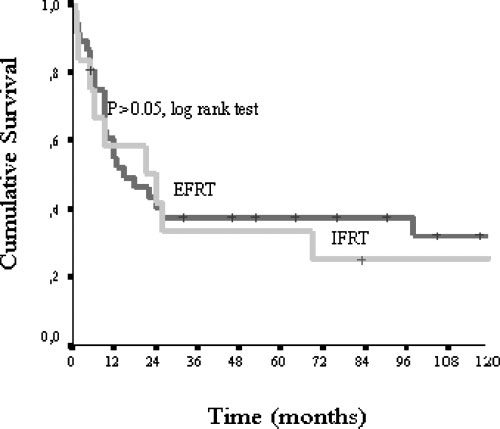
and OS rates were significantly better for patients treated
Stage I patients stratified by radiation field (extended field
with EFRT compared with IFRT; this difference was not
radiotherapy vs involved field radiotherapy).
seen in Stage II disease. This effect seemed to be mediatedat the level of the thyroid bed and adjacent lymph nodes in
or more, radiation dose was not significant in multivariate
the neck and mediastinum because 52% of patients treated
analysis of survival (hazard ratio 0.64, 95% confidence
with IFRT experienced locoregional failure compared with
interval (CI): 0.33–1.24, p50.18). However, the confidence
only 27% of patients treated with EFRT. There was no
intervals are wide and it is not possible to rule out an
difference between the two groups in terms of systemic
effect. Radiation dose was significant in multivariate
relapse. Therefore, the poor results of IFRT in all disease
analysis for local control (hazard ratio 0.42, 95% CI:
stages mean that this approach should be abandoned in
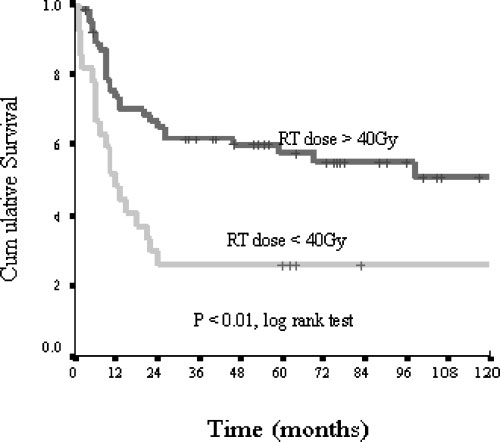
0.18–0.94, p50.04). At 5 years, only 7 of 27 (26%) patients
favour of more extensive radiation fields that encompass
treated at the lower dose level were alive, compared with
the mediastinal nodes. For patients with Stage I disease,
35 of 62 (56%) treated to 40 Gy or more (p,0.01, log rank
definitive EFRT yielded excellent rates of local control and
test). However, the first group included six patients who
survival and represented the treatment of choice. However,
received doses of less than 30 Gy; none achieved local
more recently, combination chemotherapy followed by RT
control and their maximal survival was 6 months. The
has become the standard of care for this disease and given
effect of radiation dose on outcome is presented in
the data from this study, EFRT should be considered as
Figure 2. Kaplan-Meier curve showing overall survival of
Figure 3. Kaplan-Meier curve showing overall survival of
Stage II patients stratified by radiation field (extended field
patients according to the radiation dose received (,40 Gy vs
radiotherapy vs involved field radiotherapy).
The British Journal of Radiology, May 2005
Similarly, analysis of outcomes at radiation doses below
5. Ansell SM, Grant CS, Habermann TM. Primary thyroid
40 Gy versus 40 Gy or more provides clear indications for
lymphoma. Semin Oncol 1999;26:316–23.
clinical practice. A threshold dose of 40 Gy or more was
6. Bisbee AC, Thoeny RH. Malignant lymphoma of the thyroid
shown to be associated with a significantly improved local
following irradiation. Cancer 1975;35:1296–9.
7. Burke JS, Butler JJ, Fuller LM. Malignant lymphomas of the
control outcome. This is in keeping with previous data [23]
thyroid: a clinical pathologic study of 35 patients including
and we suggest a standard dose of 40 Gy in 20 fractions
ultra structural observations. Cancer 1977;39:1587–602.
8. Derringer GA, Thompson LD, Frommelt RA, Bijwaard KE,
The data on extent of surgical resection indicate a
Heffess CS, Abbondanzo SL. Malignant lymphoma of the
significantly improved outcome in patients who underwent
thyroid gland: a clinicopathologic study of 108 cases. Am J
a debulking procedure (defined as anything more than a
biopsy) prior to RT and concur with those reported in
9. Ha CS, Shadle KM, Medeiros LJ, et al. Localized non-
previous studies [33, 34]. Patients who had total macro-
Hodgkin lymphoma involving the thyroid gland. Cancer
scopic removal of tumour had the highest rate of local
control and long term survival (p,0.001). No significant
10. Holmes HB Jr, Kreutner A, O’Brien PH. Hashimoto’s
differences were seen between lobectomy, subtotal or total
thyroiditis and its relationship to other thyroid diseases. Surg Gynecol Obstet 1977;144:887–90.
thyroidectomy, although seven of nine long-term survivors
11. Pledge S, Bessell EM, Leach IH, et al. Non-Hodgkin’s
(58–129 months) underwent total thyroidectomy. Despite
lymphoma of the thyroid: retrospective review of all patients
these findings, it is unlikely that the trend towards
diagnosed in Nottinghamshire from 1973 to 1992. Clin Oncol
performing open biopsy to make a tissue diagnosis will
be reversed. The increasing role of combination chemo-
12. Skarsgard ED, Connors JM, Robins RE. A current analysis
therapy and consolidating RT is likely to strengthen the
move towards more conservative surgical intervention [32,
13. Baskal N, Erdogan G, Kamel AN, Dagci SS, Akyar S, Ekinci
The precise role of combination chemotherapy in
C. Localized non-Hodgkin’s lymphoma of the adrenal and
TNHL remains to be defined, although in recent years it
thyroid glands. Endocrinol Jpn 1992;39:269–76.
has become part of the standard management of this
14. Butler JS Jr, Brady LW, Amendola BE. Lymphoma of the
thyroid. Report of five cases and review. Am J Clin Oncol
disease. This study demonstrates the generally poor results
obtained with RT alone, even with EFRT, in patients with
15. Heimann R. Primary malignant lymphomas of the thyroid. A
anything more than Stage I disease and provide strong
brief review. Acta Otorhinolaryngol Belg 1987;41:727–35.
support for the use of chemotherapy as part of the primary
16. Ifrah N, Rohmer V, Saint-Andre JP, Jardel H, Boasson M,
treatment. The ability of chemotherapy to ‘‘debulk’’ the
Bigorgne JC. Primary lymphoma of the thyroid gland.
tumour prior to starting RT (in an analogous fashion to
Diagnostic and therapeutic discussion. Apropos of 4 cases.
surgical debulking) represents a further attraction. Indeed,
Ann Med Interne (Paris) 1988;139:344–8.
despite the fact that low-grade MALT lymphomas have a
17. Kuma K, Matsuzuka F. Diagnosis and therapy of malignant
low distant recurrence rate [26, 28], a review of the
thyroid lymphoma. Nippon Naika Gakkai Zasshi 1997;86:
published literature suggests that the addition of chemo-
therapy to RT significantly reduces both distant and
18. Tennvall J, Cavallin-Stahl E, Akerman M. Primary localized
non-Hodgkin’s lymphoma of the thyroid: a retrospective
clinicopathological review. Eur J Surg Oncol 1987;13:297–
In conclusion, the following recommendations are made
for the management of TNHL. IFRT yields unacceptable
19. Tsutsui K, Shibamoto Y, Yamabe H, et al. A radio-
rates of disease free survival and OS and can not be
recommended. EFRT to a dose of 40 Gy is effective for
Hodgkin’s lymphoma: prognostic factors and re-evaluation
of treatment modality. Radiother Oncol 1991;21:83–90.
For Stage II–IV disease, EFRT is associated with poor
20. Friedberg MH, Coburn MC, Monchik JM. Role of surgery in
outcome; these patients should receive induction chemo-
stage IE non-Hodgkin’s lymphoma of the thyroid. Surgery
therapy followed by consolidation EFRT to a dose of
21. Rasbach DA, Mondschein MS, Harris NL, Kaufman DS,
Wang CA. Malignant lymphoma of the thyroid gland: aclinical and pathologic study of twenty cases. Surgery1985;98:1166–70.
22. Woolner LB, McConahey WM, Beahrs OH, Black BM.
Primary malignant lymphoma of the thyroid. Review of
1. Evans TR, Mansi JL, Bevan DH, Dalgleish AG, Harmer CL.
forty-six cases. Am J Surg 1966;111:502–23.
Primary non-Hodgkin’s lymphoma of the thyroid with bone
23. Tupchong L, Hughes F, Harmer CL. Primary lymphoma
marrow infiltration at presentation. Clin Oncol 1995;7:54–5.
of the thyroid: clinical features, prognostic factors, and
2. Heimann R, Vannineuse A, De Sloover C, Dor P. Malignant
results of treatment. Int J Radiat Oncol Biol Phys 1986;2:
lymphomas and undifferentiated small cell carcinoma of the
thyroid: a clinicopathological review in the light of the Kiel
24. Anscombe AM, Wright DH. Primary malignant lymphoma
of the thyroid—a tumour of mucosa-associated lymphoid
tissue: review of seventy-six cases. Histopathology 1985;9:81–
3. Souhami L, Simpson WJ, Carruthers JS. Malignant lym-
phoma of the thyroid gland. Int J Radiat Oncol Biol Phys
25. Fonseca E, Sambade C. Primary lymphomas of the thyroid
gland: a review with emphasis on diagnostic features. Arch
4. Vini L, Harmer C. Thyroid. Treatment of Cancer. In: Price P,
Sikora K, editors. Treatment of cancer (3rd edn). London:
26. Isaacson PG. Lymphoma of the thyroid gland. Curr Top
The British Journal of Radiology, May 2005
K J Harrington, V J Michalaki, L Vini et al
27. Kossev P, Livolsi V. Lymphoid lesions of the thyroid: review
35. Blair TJ, Evans RG, Buskirk SJ, Banks PM, Earle JD.
in light of the revised European-American lymphoma
Radiotherapeutic management of primary thyroid lymphoma.
classification and upcoming World Health Organization
Int J Radiat Oncol Biol Phys 1985;11:365–70.
classification. Thyroid 1999;9:1273–80.
36. Kanetake H, Toda M, Kawamoto Y. Prognostic factors in
28. Laing RW, Hoskin P, Hudson BV. The significance of MALT
primary lymphoma of the thyroid—a review of 74 cases.
histology in thyroid lymphoma: a review of patients from the
Nippon Jibiinkoka Gakkai Kaiho 1993;96:1105–11.
BNLI and Royal Marsden Hospital. Clin Oncol 1994;6:
37. Belal AA, Allam A, Kandil A, et al. Primary thyroid
lymphoma: a retrospective analysis of prognostic factors and
29. Logue JP, Hale RJ, Stewart AL, Duthie MB, Banerjee SS.
treatment outcome for localized intermediate and high grade
Primary malignant lymphoma of the thyroid: a clinicopatho-
lymphoma. Am J Clin Oncol 2001;24:299–305.
logical analysis. Int J Radiat Oncol Biol Phys 1992;22:
38. Doria R, Jekel JF, Cooper DL. Thyroid lymphoma. The case
for combined modality therapy. Cancer 1994;73:200–6.
30. Sasai K, Yamabe H, Haga H, et al. Non-Hodgkin’s
39. Gospodarowicz MK, Sutcliffe SB, Brown TC, Chua T, Bush
lymphoma of the thyroid. A clinical study of twenty-two
RS. Patterns of disease in localized extranodal lymphomas.
31. Singer JA. Primary lymphoma of the thyroid. Am Surg
40. Leedman PJ, Sheridan WP, Downey WF, Fox RM, Martin
FI. Combination chemotherapy as single modality therapy for
32. Wirtzfeld DA, Winston JS, Hicks WL, Loree TR. Clinical
presentation and treatment of non-Hodgkin’s lymphoma of
the thyroid gland. Ann Surg Oncol 2001;8:338–41.
41. Vigliotti A, Kong JS, Fuller LM, Velasquez WS. Thyroid
33. Pyke CM, Grant CS, Habermann TM, et al. Non-Hodgkin’s
lymphomas stages IE and IIE: comparative results for
lymphoma of the thyroid: is more than biopsy necessary?
radiotherapy only, combination chemotherapy only, and
multimodality treatment. Int J Radiat Oncol Biol Phys
34. Tsang RW, Gospodarowicz MK, Sutcliffe SB, Sturgeon JF,
Panzarella T, Patterson BJ. Non-Hodgkin’s lymphoma of thethyroid gland: prognostic factors and treatment outcome. ThePrincess Margaret Hospital Lymphoma Group. Int J RadiatOncol Biol Phys 1993;27:599–604.
The British Journal of Radiology, May 2005
Issue 2010/056 Title Cyclooxygenase-2 Selective Non-Steroidal Anti-Inflammatory Drugs (Etodolac, Meloxicam, Celecoxib, Rofecoxib, Etoricoxib, Valdecoxib and Lumiracoxib) for Osteoarthritis and Rheumatoid Arthritis: A Systematic Review and Economic Evaluation Agency NETSCC, HTA, NIHR Evaluation and Trials Coordinating Centre Alpha House, University of Southampton Science Pa
Testimony Concerning The FDA Approval of Psychamine Three years before the Washington hearings, PsychamineTM was used on an experimental basis in an urban area in the Northeast. Newsweek reported on the results. Susan A. has spent most of her adult life fighting After ten years of testing, psychamine is so far with people—her parents, her neighbors, her co-completely without side ef
 K J Harrington, V J Michalaki, L Vini et al
Table 5. Survival according to stage of disease and extent ofirradiated volume
IFRT, involved field radiotherapy; EFRT, extended field radio-
Analysis of the data from this large series of patients
with TNHL treated over a prolonged period of time in asingle centre provides valuable insights in to the manage-ment of this uncommon disease. RT has traditionallyplayed a major role in treatment of TNHL and thefindings of this study have direct bearing on its use.
K J Harrington, V J Michalaki, L Vini et al
Table 5. Survival according to stage of disease and extent ofirradiated volume
IFRT, involved field radiotherapy; EFRT, extended field radio-
Analysis of the data from this large series of patients
with TNHL treated over a prolonged period of time in asingle centre provides valuable insights in to the manage-ment of this uncommon disease. RT has traditionallyplayed a major role in treatment of TNHL and thefindings of this study have direct bearing on its use.