Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients viagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Ipps logo
Initial History and Physical Examination Date:___________________________
This assessment form is intended to assist the clinician with the initial patient assessment and is not meant to be a diagnostic tool.
Contact Information Name:___________________________________ Birth Date:_________________
Phone: Work: ____________________________
Referring Provider’s Name and Address: __________________________________________________________________
Information About Your Pain Please describe your pain problem (use a separate sheet of paper if needed) :_______________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ What do you think is causing your pain?____________________________________________________________________ Is there an event that you associate with the onset of your pain? Yes No If so, what?_________________________ How long have you had this pain? ____ years ____ months For each of the symptoms listed below, please “bubble in” your level of pain over the last month using a 10-point scale:
0 - no pain 10 – the worst pain imaginable
intercourse Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Pelvic pain lasting hours or days after intercourse
urination Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Backache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Migraine
headache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Provider Comments ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact
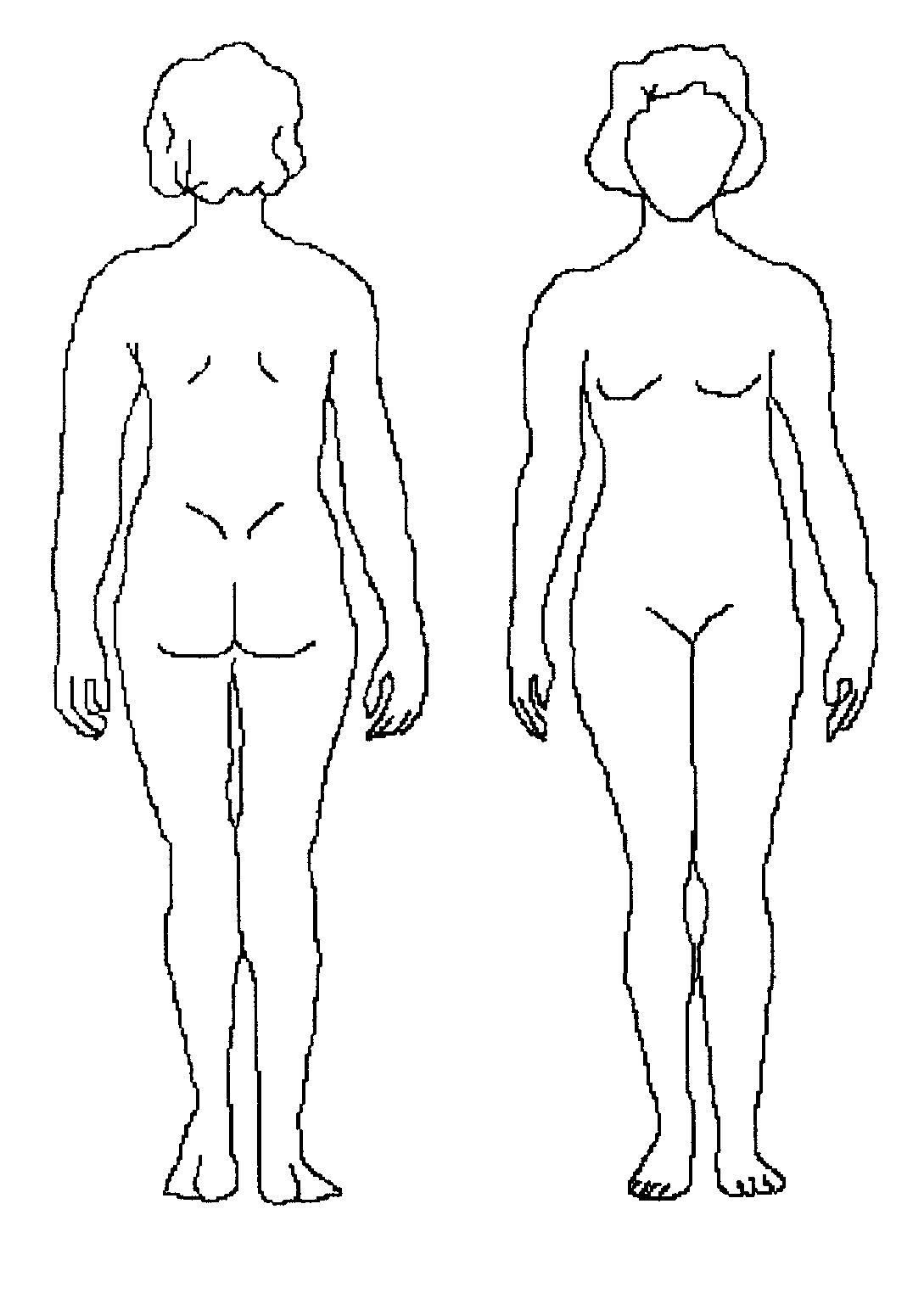
What types of treatments / providers have you tried in the past for your pain? Please check all that apply. Pain Maps Please shade areas of pain and write a number from 1 to 10 at the site(s) of pain. (10 = most severe pain imaginable)
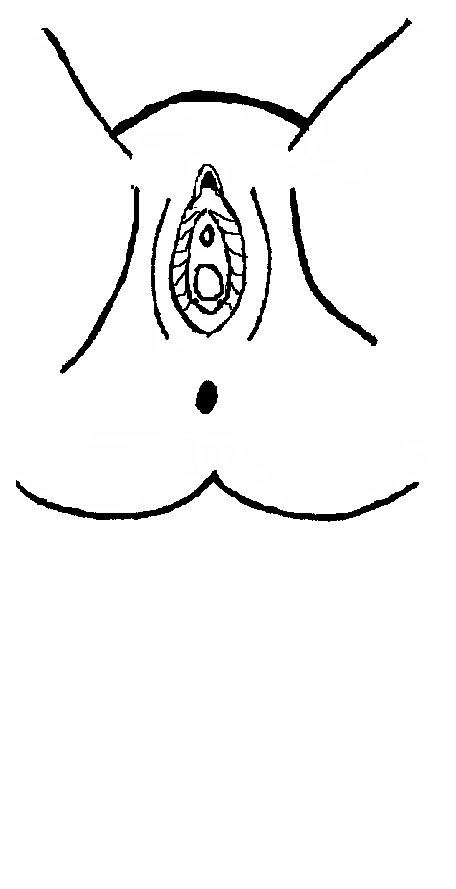
Vulvar / Perineal Pain (pain outside and around the vagina and anus) If you have vulvar pain, shade the painful areas and write a number from 1 to 10 at the painful sites. (10 = most severe pain imaginable) Is your pain relieved by sitting on a commode seat?
April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact What physicians or health care providers have evaluated or treated you for chronic pelvic pain? Physician / Provider Specialty City, State, Phone Demographic Information Are you (check all that apply):
Who do you live with? _____________________________________________________________________________ Education:
What type of work are you trained for? ________________________________________________________________ What type of work are you doing? ____________________________________________________________________
Surgical History Please list all surgical procedures you have had related to this pain: Year
Please list all other surgical procedures: Provider Comments _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact Medications Please list pain medication you have taken for your pain condition in the past 6 months, and the providers who prescribed them (use a separate page if needed): Medication / dose
Please list all other medications you are presently taking, the condition, and the provider who prescribed them (use a separate page if needed): Medication / dose Obstetrical History How many pregnancies have you had? ________ Resulting in (#): ____ Full 9 months ____ Premature ____ Miscarriage / Abortion ____ Living children Where there any complications during pregnancy, labor, delivery, or post partum?
Medication for bleeding Other _________________
Family History Has anyone in your family had:
Endometriosis Cancer, Type(s) _____________________________________
Medical History Please list any medical problems / diagnoses _________________________________________________________________ _____________________________________________________________________________________________________ _____________________________________________________________________________________________________ Allergies (including latex allergy) _________________________________________________________________________ Who is your primary care provider? _______________________________________________________________________ Have you ever been hospitalized for anything besides childbirth? Yes No If yes, please explain____________ _________________________________________________________________________________________________ Have you had major accidents such as falls or a back injury? Yes No Have you ever been treated for depression? Yes No Treatments: Medication Hospitalization Psychotherapy Birth control method:
Nothing Pill Vasectomy Vaginal ring Depo provera
Condom IUD Hysterectomy Diaphragm Tubal Sterilization
April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact
How old were you when your menses started? _________
Are you still having menstrual periods? Yes No
Answer the following only if you are still having menstrual periods.
How many days between your periods? ____________
How many days of menstrual flow? _______________
Date of first day of last menstrual period ___________
Do you have any pain with your periods? Yes
Does pain start the day flow starts? Yes
Do you pass clots in menstrual flow? Yes
Have you ever had an eating disorder such as anorexia or bulimia?
Are you experiencing rectal bleeding or blood in your stool?
Do you have increased pain with bowel movements?
The following questions help to diagnose irritable bowel syndrome, a gastrointestinal condition, which may be a cause Do you have pain or discomfort that is associated with the following:
Change in appearance of stool or bowel movement?
Does your pain improve after completing a bowel movement? Yes
Health Habits How often do you exercise?
Rarely 1-2 times weekly 3-5 times weekly Daily
What is your caffeine intake (number cups per day, include coffee, tea, soft drinks, etc)? 0 1-3 4-6 >6 How many cigarettes do you smoke per day? ___________
Have you ever received treatment for substance abuse? Yes No What is your use of recreational drugs? Never used Used in the past, but not now Presently using No answer
Heroin Amphetamines Marijuana Barbiturates Cocaine Other _______________________
How would you describe your diet? (check all that apply) Well balanced Vegan Vegetarian Fried food
Special diet ________________________ Other __________________________
April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact
Loss of urine when coughing, sneezing, or laughing? Yes
Still feeling full after urination? Yes
Having to void again within minutes of voiding?
The following questions help to diagnose painful bladder syndrome, which may cause pelvic pain Please circle the answer that best describes your bladder function and symptoms.
1. How many times do you go to the bathroom DURING THE DAY (to void or empty your bladder)?
2. How many times do you go to the bathroom
AT NIGHT (to void or empty your bladder)?
3. If you get up at night to void or empty your bladder
5. If you are sexually active, do you now or have you ever
had pain or symptoms during or after sexual intercourse?
6. If you have pain with intercourse, does it make you
7. Do you have pain associated with your bladder or in
your pelvis (lower abdomen, labia, vagina, urethra, perineum)?
2000 C. Lowell Parsons, MD Reprinted with permission. KCl ____ Not Indicated ____ Positive ____ Negative April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact Coping Mechanisms Who are the people you talk to concerning your pain, or during stressful times?
Mental Health provider I take care of myself
How does your partner deal with your pain?
Other _________________________________
Of all the problems or stresses or your life, how does your pain compare in importance?
Sexual and Physical Abuse History Have you ever been the victim of emotional abuse? This can include being humiliated or insulted Yes No No answer
Check an answer for both as a child and as an adult.
1a. Has anyone ever exposed the sex organs of their body to you when you did not want it? Yes No Yes No 1b. Has anyone ever threatened to have sex with you when you did not want it?
1c. Has anyone ever touched the sex organs of your body when you did not want this? Yes No Yes No 1d. Has anyone ever made you touch the sex organs of their body when you did not want this? Yes No Yes No 1e. Has anyone forced you to have sex when you did not want this?
1f. Have you had any other unwanted sexual experiences not mentioned above?
If yes, please specify _________________________________________________________________________________ 2. When you were a child (13 or younger), did an older person do the following?
3. Now that you are an adult (14 or older), has any other adult done the following?
Leserman, J, Drossman D, Li Z. The reliability and validity of a sexual and physical abuse history questionnaire in female patients with gastrointestinal disorders. Behavioral Medicine 1995;21:141-148. April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact Short-Form McGill The words below describe average pain. Place a check mark (√) in the column which represents the degree to which you feel that type of pain. Please limit yourself to a description of the pain in your pelvic area only. What does your pain feel like? Type None (0) Mild (1) Moderate (2) Severe (3)
__________ __________ __________ __________
Melzak R. The Short-form McGill Pain Questionnaire. Pain 1987;30:191-197. Pelvic Varicosity Pain Syndrome Questions Is your pelvic pain aggravated by prolonged physical activity?
Does your pelvic pain improve when you lie down?
Do you have pain that is deep in the vagina or pelvis during sex?
Do you have pelvic throbbing or aching after sex? Yes No Do you have pelvic pain that moves from side to side?
Do you have sudden episodes of severe pelvic pain that come and go?
April 2008, The International Pelvic Pain Society This document may be freely reproduced and distributed as long as this copyright notice remains intact
Your Complete Oral Type 2 Meds Reference Guide from Diabetes Health magazine Drug Class and How It Works Brand and Generic Name Manufacturer Usual Starting Dose Sulfonylureas: The fi rst three types of Amaryl (glimepiride) 1 to 2 mg once a day, taken with the fi rst mealoral diabetes medications listed here—the sulfonylureas, the meglitinides and the
Patient Procedure Guidelines Arm and Chest Port insertion and removal: (Ordering Physician) Send signed order specifying arm or chest port, history and physical, recent labs including platelet count, and list of meds to FAX 765-9955. Patient must be NPO for 6 hours prior to procedure in order to receive IV Conscious Sedation. Oral meds may be taken with water. Patient must bring driver an

 Initial History and Physical Examination
Date:___________________________
This assessment form is intended to assist the clinician with the initial patient assessment and is not meant to be a diagnostic tool.
Contact Information Name:___________________________________ Birth Date:_________________
Phone: Work: ____________________________
Referring Provider’s Name and Address: __________________________________________________________________
Information About Your Pain Please describe your pain problem (use a separate sheet of paper if needed) :_______________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ What do you think is causing your pain?____________________________________________________________________ Is there an event that you associate with the onset of your pain? Yes No If so, what?_________________________ How long have you had this pain? ____ years ____ months For each of the symptoms listed below, please “bubble in” your level of pain over the last month using a 10-point scale:
0 - no pain 10 – the worst pain imaginable
intercourse Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Pelvic pain lasting hours or days after intercourse
urination Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Backache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Migraine
headache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Provider Comments ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________
April 2008, The International Pelvic Pain Society
This document may be freely reproduced and distributed as long as this copyright notice remains intact
Initial History and Physical Examination
Date:___________________________
This assessment form is intended to assist the clinician with the initial patient assessment and is not meant to be a diagnostic tool.
Contact Information Name:___________________________________ Birth Date:_________________
Phone: Work: ____________________________
Referring Provider’s Name and Address: __________________________________________________________________
Information About Your Pain Please describe your pain problem (use a separate sheet of paper if needed) :_______________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ What do you think is causing your pain?____________________________________________________________________ Is there an event that you associate with the onset of your pain? Yes No If so, what?_________________________ How long have you had this pain? ____ years ____ months For each of the symptoms listed below, please “bubble in” your level of pain over the last month using a 10-point scale:
0 - no pain 10 – the worst pain imaginable
intercourse Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Pelvic pain lasting hours or days after intercourse
urination Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Backache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Migraine
headache Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο Ο
Provider Comments ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________ ____________________________________________________________________________________________________
April 2008, The International Pelvic Pain Society
This document may be freely reproduced and distributed as long as this copyright notice remains intact
 What types of treatments / providers have you tried in the past for your pain? Please check all that apply.
What types of treatments / providers have you tried in the past for your pain? Please check all that apply.