Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients cialis uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Bodyfocushealthgroup.com.au
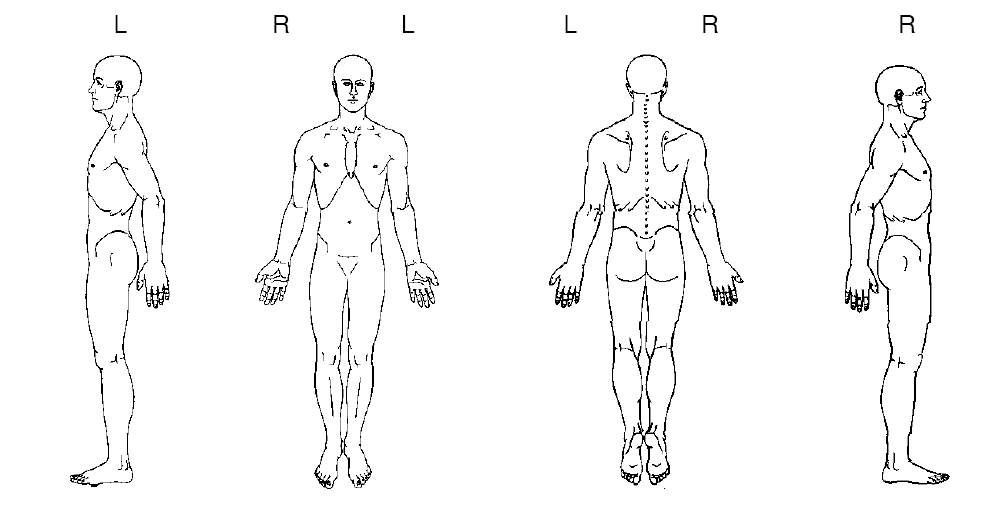
CONFIDENTIAL PATIENT CASE HISTORY As a multidisciplinary practice providing comprehensive care, we focus on your ability to be healthy. Our goals are: firstly, to address the issues that brought you to this practice; secondly, to treat the cause of your condition (not just treat the symptoms or place a temporary patch over your condition); and thirdly, to offer you the opportunity of improved health potential and wellness services in the future. Answering the following questions will give us a profile of your health, and ensure that we optimise your outcome and deliver treatment excellence. What is your major complaint? _________________________________________________________________ Draw on the sketch below the area(s) where you feel your problem to be.
When did your symptoms start? _________________________________________________________________ Was it a gradual or sudden onset? _________________________________________________________________ Have you had this or a similar problem in the past? _________________________________________________________________ If you are experiencing pain, please tick the words that best describe your pain:
Confidential Patient Case History Form Version 1.0,
Do you get?
needles Since the problem started it is:
About the same Getting better Getting worse
What makes your pain worse? Your pain interferes with: What type of work do you do? __________________________________________________________ Any Bladder or Bowel changes since this episode started? __________________________________________________________ Do you experience any nausea, dizziness, difficulty swallowing, changes in vision, or fainting spells, fever, skin rashes associated with your symptoms? __________________________________________________________ Other health professionals seen for this problem (please list): Medical Doctor____________________________________________________________ Specialist Doctor/Surgeon_____________________________________________________ Physiotherapist/Chiropractor __________________________________________________________________ Other __________________________________________________________________ List any medications you are taking __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ Have you ever taken oral cortisone or prednisone (including asthma medications such as pulmicort, symbicort, flixotide & seretide)? Y/N Are you pregnant? Y/N
Confidential Patient Case History Form Version 1.0,
Do you have or have you ever had?: (please tick)
High blood pressure
Patient’s Signature: _______________ Print Name: ______________________ Practitioner's Signature: _________________ Date: _____________________
Confidential Patient Case History Form Version 1.0,
Liste mit Basismedikamenten und Materialien Die folgende Liste enthält Medikamente welche häufig benutzt werden und bei denen wir sehr froh wären, wenn sie uns bei Möglichkeit solche beisteuern könnten. Erkältungs- und Bronchitis-/Asthmamedikamente: • Ambroxol, Sirup • Albuterol, Ampullen zum vernebeln/inhalieren • Ibuprofen (Brufen, Irfen, Optifen 200mg. Sirup und Tabletten �
In any given area the water quality is determined by local conditions. Pure rain water starts to absorb pol utants even as it fal s through the atmosphere. As it permeates through the soil and lies as ground water, its chemical composition is affected by the nature of the earth’s strata in the locality and the level of contaminants these contain. The various treatments that are used to produc

 CONFIDENTIAL PATIENT CASE HISTORY
CONFIDENTIAL PATIENT CASE HISTORY 
 Do you have or have you ever had?: (please tick)
Do you have or have you ever had?: (please tick)