Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients priligy uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Untitled
ALLERGIES IN THE WORKPLACE ALLSA RESEARCH AWARDS REPORT APPROACHES TO DIAGNOSING ANISAKIS
The management of anisakiasis involves physically
removing the larvae, if possible, or treating the patientwith antihelminthics, anti-inflammatories and anal-
Natalie Nieuwenhuizen,1 BSc(Med) Hons, PhD
gesics.3,4 The Anisakis larvae cannot survive or repro-duce in humans, but if the larvae are not removed, the
Mohamed Jeebhay,2 MBChB, DOH, MPhil (Epi),
disease can become chronic as inflammatory cells sur-
round the larval remains and lead to symptoms which
Andreas L Lopata,1,3 MSc, PhD (Med Science)
can mimic dyspepsia, Crohn’s syndrome, appendicitis,
1Division of Immunology, Institute of Infectious
irritable bowel syndrome, diverticulitis, non-specific
Diseases and Molecular Medicine, Faculty of Health
eosinophilic enteritis, or even gastric cancer.2
Science, University of Cape Town, South Africa
Abdominal pain, nausea, vomiting and/or diarrhoea
2Centre for Occupational and Environmental Health
within 48 hours of consuming fresh seafood should
Research, School of Public Health and Family
indicate the possibility of Anisakis infection. As many
Medicine, University of Cape Town, South Africa
cases of anisakiasis have occurred after consumptionof freshly caught fish that appeared well-cooked but
3Allergy Research Group, School of Applied Science,
was not sufficiently heated through to kill larvae, inges-
Royal Melbourne Institute of Technology, Bundoora
tion of raw seafood should not be the only factor mer-
iting further investigation. In order to kill larvae, fishshould be frozen at –20°C for at least 24 hours orcooked so that all parts of the fish reach at least 60°Cfor 10-20 minutes.2 Smoking fish or marinating it in
lemon juice or vinegar does not kill Anisakis. Anisakis is a parasitic nematode which infects fishand can cause gastrointestinal disease if accidental-
ANISAKIS ALLERGY
ly ingested. Infection can be accompanied by severe
Of particular relevance to the physician is that Anisakis
allergic reactions such as urticaria, angio-oedema
can also cause severe allergic reactions because of its
and anaphylaxis. Furthermore, workers involved in
ability to elicit strong Th2 responses.5,6 Many patients
fish processing can develop occupational allergy to
experience gastroallergic anisakiasis, in which infection
Anisakis, including asthma, rhinoconjunctivitis andprotein contact dermatitis. Diagnosis of allergy toAnisakis relies on skin-prick tests and the detectionof specific IgE by ImmunoCAP. Since Anisakisinfests fish, fish allergy should be investigated insymptomatic patients. Anisakis proteins alsodemonstrate considerable immunological cross-reactivity to proteins of related nematodes and otherinvertebrates such as house-dust mites and cock-roaches; this needs to be borne in mind when thediagnosis is made. This review outlines theapproaches that have been used to increase thespecificity of Anisakis diagnosis, including the use ofimmunoblotting and the identification of Anisakisallergens. ANISAKIS INFECTION Anisakis species are marine roundworms which use sea mammals such as dolphins and whales as primary hosts. The stage 3 larval form (L3) of Anisakis (Fig. 1) infects fish and other seafood such as squid, and con- sequently humans may become accidental hosts for Anisakis if they consume raw or undercooked fish.1 Infection is known as anisakiasis and is often associat- ed with gastrointestinal symptoms such as abdominal pain, diarrhoea, nausea and vomiting. Patients’ reac- tions range from being asymptomatic to requiring emergency room care. Since 1960 when anisakiasis was first described, thousands of cases have been reported from Japan and hundreds from Europe, the USA. and other parts of the world.2
Correspondence: Dr N Niewenhuizen, Division of Immunology,Institute of Infectious Diseases and Molecular Medicine, University of
Fig. 1. Anisakis larvae removed from Thyrsites atun
Cape Town, Observatory 7935. E-mail [email protected]
Current Allergy & Clinical Immunology, August 2009 Vol 22, No. 3
is accompanied by allergic reactions such as urticaria,
Only one case of food allergy to Anisakis has been doc-
angio-oedema, bronchospasm and/or anaphylaxis.7,8
umented in South Africa28 despite the recent popularity
This allergic response can occur without gastrointesti-
of sushi, perhaps because the disease is largely
nal symptoms, leading to misdiagnosis of the reaction
unknown to physicians and may go undiagnosed.
to Anisakis as fish allergy or idiopathic urticaria/anaphy-
Recently, several case reports described adverse reac-
laxis.5 Symptoms can begin anywhere between a few
tions to Anisakis in individuals handling fish or fishmeal,
hours to more than a day after ingestion of the para-
with symptoms ranging from conjunctivitis to allergic
site, and patients may therefore not connect the inges-
asthma.16,17,19 In an epidemiological study of two large
tion of the fish to the symptoms. Although some
fish-processing factories in St Helena Bay on the west
patients tolerate dead larvae in frozen or cooked fish,
coast of South Africa we found a prevalence of 8%
others have symptoms after eating well-cooked or
sensitisation to Anisakis among the fish-processing
canned fish, indicating that both live and dead larvae
workers,6,29 but only 1-3% had Anisakis-related allergic
and their proteins can cause allergic reactions.9-12 A his-
symptoms. The study also found that indviduals with
tory of fish consumption prior to allergic symptoms and
Anisakis sensitisation were twice as likely (OR = 2.24,
the absence of sensitisation to fish indicates the need
CI: 1.01-4.97) to have high seafood intake as measured
to test for Anisakis allergy.
by elevated level of serum omega-3 fatty acids (eicos-
Currently, the diagnosis of Anisakis allergy relies on a
apentaenoic acid). We therefore decided to look at pat-
clear history of potential exposure to Anisakis and
terns of IgE-binding proteins recognised by our
symptoms of gastroallergic anisakiasis along with
sensitised workers to compare them with patterns
Anisakis specific IgE and positive Anisakis skin-prick
found in previous studies where patients had symp-
tests (SPTs).5,7 However, because many allergens of
Anisakis are heat stable, exposure to Anisakis proteins
Immunoblotting using serum from 15 workers who
in fish on an ongoing basis can also cause symptoms
were ImmunoCAP or SPT positive to Anisakis (Table I)
such as chronic urticaria, protein contact dermatitis,
showed diverse patterns of IgE binding to Anisakis pro-
asthma and rhinoconjunctivitis.13-19 In this case the clin-
teins (Fig. 2), as has been observed in previous stud-
ical history may be less clear since patients may be
ies.30 Somatic Anisakis antigens were used for
exposed to many agents in their environment at the
immunoblotting, as the workers were likely to be
same time. The use of specific IgE alone to diagnose
exposed to Anisakis through handling of fish, inhalation
Anisakis allergy is confounded by the fact that even
of vapours and consumption of cooked fish. Workers
asymptomatic individuals can have Anisakis specific
who were positive to Anisakis on ImmunoCAP were
IgE because of cross-reactivity with other helminths
often also positive to Ascaris lumbricoides, a human
(e.g. Ascaris) or invertebrates such as dust mites, cock-
roundworm, which is closely related to Anisakis.31 A
roaches and shrimp.20-22 Studies in Spain have found
subgroup analysis of sera (n = 129) demonstrated a
that a large number of asymptomatic individuals have
very high correlation (r = 0.72, p <0.001) between IgE
Anisakis specific IgE, some related to subclinical sensi-
reactivity to Anisakis and Ascaris (unpublished data).
tisation and others due to false-positive results as a
Immunoblotting against Anisakis extract may be less
useful for diagnosis if the patient has a past Ascaris
The muscle protein tropomyosin is an important source
infection because of cross-reactivity between Anisakis
of cross-reactivity with other invertebrates. Recently
and Ascaris.32 We therefore looked at patterns of IgE
we showed by allergen microarray analysis that all
binding in workers who had a higher level of specific
patients with specific IgE antibodies to Anisakis
IgE to Anisakis than to Ascaris, similar levels of specif-
tropomyosin (Ani s 3) also recognised tropomyosin of
ic IgE to both worms, or a higher level of specific IgE to
shrimp, dust mite, cockroach and snail (unpublished
Ascaris than to Anisakis. Sera from three workers who
data). Whether Anisakis tropomyosin is a clinically rele-
were SPT positive but ImmunoCAP negative to
vant allergen is however controversial. Asturias et al .20
have suggested that tropomyosin is not an important
Most of the workers recognised a variety of medium-
allergen as asymptomatic patients were sensitised to it
molecular-weight proteins ranging from about 33 to 75
whereas symptomatic patients were not. Other
kDa, including the workers who were primarily sensi-
researchers suggest that Anisakis tropomyosin could
tised to Ascaris. Some also recognised low-molecular-
play a role in eliciting food allergy after ingestion of
weight proteins, reportedly an indication of real
cooked seafood, because it closely resembles the
exposure to Anisakis rather than cross-reactivity to
heat-stable shrimp tropomyosin, an important allergen
other invertebrates.26 The IgE-binding pattern was
more variable in the workers who had higher specificIgE to Anisakis than to Ascaris. One of these workers
THE ROLE OF IMMUNOBLOTTING IN THE
had IgE against only two proteins of approximately 52
DIAGNOSIS OF ANISAKIS ALLERGY
and 75 kDa (with fainter binding at 37 kDa) and anoth-er recognised only a single band at about 42 kDa. A
Since cross-reactivity can cause false-positives in SPTs
third was strongly sensitised to a cluster of proteins
and specific IgE tests, some authors have used IgE
immunoblotting to differentiate anisakiasis/Anisakis
Some of the IgE-binding proteins identified in our study
allergy from asymptomatic Anisakis sensitisation.24,26,27
have not yet been characterised or identified as aller-
One study found that patients with confirmed Anisakis
gens. Previous studies have also detected IgE-binding
allergy had IgE directed at several proteins of medium
proteins different to the known allergens by
molecular weight as well as low-molecular-weight pro-
immunoblot analysis.23,30,33,34 Furthermore, up to the
teins, while patients with no allergy or doubtful symp-
present allergen characterisation has used sera from
toms were more likely to recognise either a single
patients with gastroallergic anisakiasis, and it is possi-
medium-molecular-weight protein of approximately 40
ble that different proteins may be involved in occupa-
kDa (possibly Anisakis tropomyosin) or a few medium-
tional sensitisation through inhalation or skin contact.
molecular-weight proteins.26 Another study also found
Allergen recognition is thought to vary significantly
that asymptomatic blood donors with specific IgE to
from patient to patient in Anisakis allergy, and patients
Anisakis frequently detected a single protein of 42 kDa
may also recognise cross-reactive proteins from other
whereas truly sensitised patients recognised multiple
invertebrates.23,30,33,34 Originally, authors used immuno-
Current Allergy & Clinical Immunology, August 2009 Vol 22, No. 3
Table I. Descriptive data of Anisakis-sensitised workers whose sera were investigated by immunoblotting Symptoms Non-specific Anisakis Anisakis Ascaris Sensitisation Other sensitisations broncho-hyper ImmunoCAP ImmunoCAP to Anisakis (microarray, responsiveness tropomyosin ImmunoCAP* (Ani s 3) on microarray*
Current Allergy & Clinical Immunology
Pen i 1, Pen m 1, Per a 7, Der p 10, Hel as 1
ImmunoCAP: latex, lobster, anchovy, pilchard
Microarray: Api m 1, Cup a 1,Lol p 1, Ole e 1
SPT: HDM, cockroach, ryegrass, raw lobster, Aspergillus
Pen i 1, Per a 7, Pen m 1,Phl p 1, Der p 10, Hel as 1
* A value greater than 0.35 kU/l was considered positive. SPT – skin-prick test, HDM – house-dust mite. Fig. 2. IgE immunoblotting against Anisakis antigens using sera from 15 Anisakis-sensitised fish-processing work-ers. Workers 1-4 had higher specific IgE to Anisakis than to Ascaris, workers 5-10 had specific IgE to both Anisakisand Ascaris, workers 11-12 had higher levels of specific IgE to Ascaris than to Anisakis and workers 13-15 wereSPT positive to Anisakis but negative on ImmunoCAP tests.
blotting with deglycosylated Anisakis proteins or excre-
The major allergens of Anisakis (recognised by more
tory-secretory (ES) proteins to increase the specificity
than 50% of patients) are considered to be Ani s 1 and
of Anisakis diagnosis.24,33 However, to avoid misdiagno-
Ani s 7,38 although in one study Ani s 5 was recognised
sis due to cross-reactivity, it is ideally better to use puri-
by 49% of patients (41/84). The 24 kDa Ani s 1 is recog-
fied or recombinant allergens that are specific for
nised by 67-87% of patients with gastroallergic anisaki-
Anisakis-allergic patients.34 The identification of specif-
ic Anisakis allergens which could be used in tests such
individuals.23,39 This allergen is secreted by the worm
as ImmunoCAP, SPT, allergen microarray or immuno-
and shows homology to serine protease inhibitors. A
blotting will in the long term increase the specificity of
21 kDa isoform of Ani s 1 also exists.39 Ani s 1 is heat
stable and can act as a food allergen, causing reactionsafter ingestion of cooked fish. The other major allergen,
ANISAKIS ALLERGENS
Ani s 7, is also an ES product of 139 kDa and is a novelglycoprotein.40 It was recognised by 100% of patients
Currently nine allergens of Anisakis simplex have been
with Anisakis allergy.40 However, Ani s 7 has cross-
identified, most of which exist in recombinant form.
reactive O-glycans and is better for diagnostic tests
Patients may be exposed primarily to somatic antigens
from dead larvae in food, ES antigens when there is
Another important allergen is Ani s 4, a heat-stable
expulsion or surgical removal of the intact larvae, or
nematode cystatin that is recognised by only 27-30%
both, in cases where the larva penetrates the tissue, is
of patients but appears to be particularly important in
killed by the host, and subsequently degenerates
eliciting anaphylaxis.9 Heat-stable allergens such as Ani
inside the host.35 Many allergens of Anisakis are heat
s 4 are important even if they are classified as minor
and/or pepsin resistant9,36,37 and most of them are
allergens as a result of their frequency of recognition,
because these allergens are associated with allergic
Current Allergy & Clinical Immunology, August 2009 Vol 22, No. 3
Table II. Anisakis allergens Allergen Molecular weight Description Location Recognition in Recombinant Anisakis-sensitised patients protein exists References
specific IgE0% (0/10) patients with true Anisakis allergy
Current Allergy & Clinical Immunology
SPX/RAL protein Homologous with proteins in the SXP/RAL-2 family,including Ani s 5
reactions to cooked or canned fish.42 Therefore, fre-
TG, Brombacher F. Exposure to the fish parasite Anisakis causesallergic airway hyperreactivity and dermatitis. J Allergy Clin
quency of recognition is not always equal to clinical rel-
Immunol 2006; 117: 1098-1105.
evance. Other minor allergens include Ani s 5 (15 kDa),
7. Daschner A, Alonso Giqm A, Cabanas R, Suarez-de-Parga JM, MC
Ani s 8 (15 kDa) and Ani s 9 (14 kDa), which share
Liqm-S. Gastroallergic anisakiasis: borderline between food allergy
homology and are all members of the SPX/RAL-2 fami-
and parasitic disease – clinical and allergologic evaluation of 20
ly, which is specific to nematodes. They are all heat-sta-
patients with confirmed acute parasitism by Anisakis simplex.
ble ES products, although Ani s 9 is reportedly more
J Allergy Clin Immunol 2000; 105: 176-181.
abundant in crude extract, and their biological function
8. Audicana MT, Fernandez de Corres L, Munoz D, Fernandez E,
Navarro JA, del Pozo MD. Recurrent anaphylaxis caused by
is unknown.36,42,43 Another minor allergen, Ani s 6 (7
Anisakis simplex parasitizing fish. J Allergy Clin Immunol 1995; 96:
kDa), is homologous with serine protease inhibitors,
including the honeybee allergen Api m 6.34
9. Moneo I, Caballero ML, Gonzalez-Munoz M, Rodriguez-Mahillo AI,
The remaining two allergens, Ani s 2 (41 kDa) and Ani
Rodriguez-Perez R, Silva A. Isolation of a heat-resistant allergen from the fish parasite Anisakis simplex. Parasitol Res 2005; 96:
s 3 (100 kDa) are the muscle proteins paramyosin and
tropomyosin, respectively, and are thought to be pri-
10. Audicana L, Audicana MT, Fernandez de Corres L, Kennedy MW.
marily responsible for cross-reactivity between
Cooking and freezing may not protect against allergenic reactions
Anisakis and other invertebrates.20,25,44 They do not
to ingested Anisakis simplex antigens in humans. Vet Rec 1997;
appear to be important in eliciting allergic reactions to
140: 235. Anisakis,20,38 but further studies are needed. A 21 kDa
11. Fernandez de Corres L, Audicana M, et al. Anisakis simplex induces
protein with homology to nematode troponin has also
not only anisakiasis: report on 28 cases of allergy caused by this nematode. J Investig Allergol Clin Immunol 1996; 6: 315-319.
been identified as an allergen but has never beennamed.45
12. Del Pozo MD, Audicana M, Diez JM, et al. Anisakis simplex, a rel-
evant etiologic factor in acute urticaria. Allergy 1997; 52: 576-579.
Purified Anisakis allergens have proven useful in diag-
13. Montoro A, Perteguer MJ, Chivato T, Laguna R, Cuellar C.
nosis, especially in combination. In one study, 95% of
Recidivous acute urticaria caused by Anisakis simplex. Allergy
64 Anisakis-allergic patients tested positive for Ani s 1
1997; 52: 985-991.
and/or Ani s 4 by immunoblotting47 and in a follow-up
14. Daschner A, Vega de la Osada F, Pascual CY. Allergy and parasites
study, only 12% of patients (10/84) did not recognise
reevaluated: wide-scale induction of chronic urticaria by the ubiqui-tous fish-nematode Anisakis simplex in an endemic region. Allergol
one or both of these allergens.36 Including Ani s 5 to
Immunopathol (Madr ) 2005; 33: 31-37.
the panel of allergens tested raised the sensitivity to
15. Kasuya S, Hamano H, Izumi S. Mackerel-induced urticaria and
94%, with 79/84 patients recognising one or more of
Anisakis. Lancet 1990; 335: 665.
16. Armentia A, Lombardero M, Callejo A, et al. Occupational asthma
Table II lists the nine Anisakis allergens.
by Anisakis simplex. J Allergy Clin Immunol 1998; 102: 831-834.
17. Scala E, Giani M, Pirrotta L, et al. Occupational generalised urticaria
APPROACH TO THE DIAGNOSIS AND
and allergic airborne asthma due to Anisakis simplex. Eur J Dermatol 2001; 11: 249-250. MANAGEMENT OF ANISAKIS ALLERGY
18. Carretero Anibarro P, Blanco Carmona J, Garcia Gonzalez F, et al.
The ideal diagnostic test for Anisakis allergy should
Protein contact dermatitis caused by Anisakis simplex. Contact Dermatitis 1997; 37: 247.
include all clinically relevant Anisakis allergens.
19. Anibarro B, Seoane FJ. Occupational conjunctivitis caused by sen-
Currently, CAP-RAST and SPTs use whole Anisakis
sitization to Anisakis simplex. J Allergy Clin Immunol 1998; 102:
extracts, while the latest allergen microarrays only con-
tain Ani s 1 and Ani s 3. Once a patient has confirmed
20. Asturias JA, Eraso E, Moneo I, Martinez A. Is tropomyosin an aller-
Anisakis allergy, after excluding fish allergy and taking
gen in Anisakis? Allergy 2000; 55: 898-899.
into consideration cross-reactivity to other helminths
21. Kennedy MW, Tierney J, Ye P, et al. The secreted and somatic anti-
(e.g. Ascaris) or invertebrates such as dust mites, cock-
gens of the third stage larva of Anisakis simplex, and antigenic rela-
roaches and shrimp, identifying which allergens are
tionship with Ascaris suum, Ascaris lumbricoides, and Toxocara canis. Mol Biochem Parasitol 1988; 31: 35-46.
recognised by the patient will assist in making dietary
22. Pascual CY, Crespo JF, San Martin S, et al. Cross-reactivity
recommendations.9 Many patients with Anisakis allergy
between IgE-binding proteins from Anisakis, German cockroach,
are able to tolerate a diet of frozen or well-cooked
and chironomids. Allergy 1997; 52: 514-520.
fish,48 but a small percentage of patients are particular-
23. Moneo I, Caballero ML, Gomez F, Ortega E, Alonso MJ. Isolation
ly sensitised to heat-stable allergens such as Ani s 4
and characterization of a major allergen from the fish parasite
and react badly to cooked or canned fish.2,9,33 These
Anisakis simplex. J Allergy Clin Immunol 2000; 106: 177-182.
patients should avoid marine fish altogether.
24. Moneo I, Audicana MT, Alday E, Curiel G, del Pozo MD, Garcia M.
Periodate treatment of Anisakis simplex allergens. Allergy 1997; 52: 565-569. Declaration of conflict of interest
25. Guarneri F, Guarneri C, Benvenga S. Cross-reactivity of Anisakis
The authors declare no conflicts of interest. simplex: possible role of Ani s 2 and Ani s 3. Int J Dermatol 2007; 46: 146-50. Acknowledgements
26. Garcia M, Moneo I, Audicana MT, et al. The use of IgE immunoblot-
ting as a diagnostic tool in Anisakis simplex allergy. J Allergy Clin
This work was sponsored by the Medical Research Council (MRC) and
Immunol 1997; 99: 497-501.
National Research Foundation of South Africa and an Allergy Society of
27. Del Pozo MD, Moneo I, de Corres LF, et al. Laboratory determina-
South Africa (ALLSA) research award.
tions in Anisakis simplex allergy. J Allergy Clin Immunol 1996; 97: 977-984. REFERENCES
28. Du Plessis K, Lopata AL, Steinman H. Adverse reactions to fish. Current Allergy & Clinical Immunology 2004; 17: 4-8.
Sakanari JA, McKerrow JH. Anisakiasis. Clin Microbiol Rev 1989; 2: 278-284.
29. Jeebhay MF, Robins TG, Miller ME, et al. Occupational allergy and
asthma among salt water fish processing workers. Am J Ind Med
Audicana MT, Ansotegui IJ, de Corres LF, Kennedy MW. Anisakis sim-
2008; 51: 899-910.
plex: dangerous – dead and alive? Trends Parasitol 2002; 18: 20-25.
30. Arlian LG, Morgan MS, Quirce S, Maranon F, Fernandez-Caldas E.
Moore DA, Girdwood RW, Chiodini PL. Treatment of anisakiasis
Characterization of allergens of Anisakis simplex. Allergy 2003; 58:
with albendazole. Lancet 2002; 360: 54.
Pacios E, Arias-Diaz J, Zuloaga J, Gonzalez-Armengol J, Villarroel P,
31. Blaxter ML, de Ley P, Garey JR, et al. A molecular evolutionary
Balibrea JL. Albendazole for the treatment of anisakiasis ileus. Clin
framework for the phylum Nematoda. Nature 1998; 392: 71-75. Infect Dis 2005; 41: 1825-1826.
32. Sakanari JA, Loinaz HM, Deardorff TL, Raybourne RB, McKerrow
Baeza ML, Zubeldia JM, Rubio M. Anisakis simplex allergy. ACI
JH, Frierson JG. Intestinal anisakiasis. A case diagnosed by mor-
International 2001; 13: 242-249.
phologic and immunologic methods. Am J Clin Pathol 1988; 90:
Nieuwenhuizen N, Lopata AL, Jeebhay MF, Herbert DR, Robins
Current Allergy & Clinical Immunology, August 2009 Vol 22, No. 3
33. Baeza ML, Rodriguez A, Matheu V, et al. Characterization of allergens
41. Iglesias R, Leiro J, Santamarina MT, Sanmartin ML, Ubeira FM.
secreted by Anisakis simplex parasite: clinical relevance in compari-
Monoclonal antibodies against diagnostic Anisakis simplex anti-
son with somatic allergens. Clin Exp Allergy 2004; 34: 296-302.
gens. Parasitol Res 1997; 83: 755-761.
34. Kobayashi Y, Ishizaki S, Shimakura K, Nagashima Y, Shiomi K.
42. Rodriguez-Perez R, Moneo I, Rodriguez-Mahillo A, Caballero ML.
Molecular cloning and expression of two new allergens from
Cloning and expression of Ani s 9, a new Anisakis simplex allergen. Anisakis simplex. Parasitol Res 2007; 100: 1233-1241. Mol Biochem Parasitol 2008; 159: 92-97.
35. Audicana MT, Kennedy MW. Anisakis simplex: from obscure infec-
43. Kobayashi Y, Shimakura K, Ishizaki S, Nagashima Y, Shiomi K.
tious worm to inducer of immune hypersensitivity. Clin Microbiol
Purification and cDNA cloning of a new heat-stable allergen from
Rev 2008; 21: 360-379, table of contents. Anisakis simplex. Mol Biochem Parasitol 2007; 155: 138-145.
36. Caballero ML, Moneo I, Gomez-Aguado F, Corcuera MT, Casado I,
44. Perez-Perez J, Fernandez-Caldas E, Maranon F, et al. Molecular
Rodriguez-Perez R. Isolation of Ani s 5, an excretory-secretory and
cloning of paramyosin, a new allergen of Anisakis simplex. Int Arch
highly heat-resistant allergen useful for the diagnosis of AnisakisAllergy Immunol 2000; 123: 120-129.
larvae sensitization. Parasitol Res 2008; 103: 1231-1233.
45. Arrieta I, del Barrio M, Vidarte L, et al. Molecular cloning and char-
37. Caballero ML, Moneo I. Several allergens from Anisakis simplex
acterization of an IgE-reactive protein from Anisakis simplex: Ani
are highly resistant to heat and pepsin treatments. Parasitol Res
s 1. Mol Biochem Parasitol 2000; 107: 263-268.
2004; 93: 248-251.
46. Rodriguez-Mahillo AI, Gonzalez-Munoz M, Gomez-Aguado F, et al.
38. Anadon AM, Romaris F, Escalante M, et al. The Anisakis simplex
Cloning and characterisation of the Anisakis simplex allergen Ani s
Ani s 7 major allergen as an indicator of true Anisakis infections.
4 as a cysteine-protease inhibitor. Int J Parasitol 2007; 37: 907-917. Clin Exp Immunol 2009; 156: 471-478.
47. Moneo I, Caballero ML, Rodriguez-Perez R, Rodriguez-Mahillo AI,
39. Shimakura K, Miura H, Ikeda K, et al. Purification and molecular
Gonzalez-Munoz M. Sensitization to the fish parasite Anisakis sim-
cloning of a major allergen from Anisakis simplex. Mol Biochemplex: clinical and laboratory aspects. Parasitol Res 2007; 101: 1051- Parasitol 2004; 135: 69-75.
40. Rodriguez E, Anadon AM, Garcia-Bodas E, et al. Novel sequences
48. Garcia F, Blanco JG, Garces M, Juste S, Fuentes M, Herrero D.
and epitopes of diagnostic value derived from the Anisakis simplex
Freezing protects against allergy to Anisakis simplex. J Investig
Ani s 7 major allergen. Allergy 2008; 63: 219-225. Allergol Clin Immunol 2001; 11: 49-52. For further information contact: The Congress Office Sue McGuinness Communications & Event Management PO Box 782243, Sandton, 2146, Johannesburg South Africa Telephone: +27 (0)11 447 3876 Fax: +27 (0)11 442 8094 Email: [email protected] www.allergysa.co.za
Current Allergy & Clinical Immunology, August 2009 Vol 22, No. 3
Im Langacher 15 * CH - 8805 Richterswil Finde Dein Lebenstempo. Entschleunigen am Zürichsee. Mal eben schnell das Lebenstempo verändern, funktioniert nicht. Es braucht Zeit und Raum. In meiner Rolle als Coach und Gastgeberin stelle ich Zeit und Raum zur Verfügung: Mein Haus: Das Allegra Bio Bed & Breakfast. Diese Workshopwoche für selbständige Dienstleister macht Sinn,
International Journal of Pharmaceutics 309 (2006) 199–2071. Properties and in vitro/in vivo behavior of acyclovirYiguang Jin , Li Tong , Ping Ai , Miao Li , Xinpu Hou a Department of Pharmaceutical Chemistry, Beijing Institute of Radiation Medicine, Beijing 100850, PR China b Department of Physical Pharmacy, School of Pharmaceutical Sciences, Peking University, Beijing 100083, PR Chi
 ALLERGIES IN THE WORKPLACE
ALLERGIES IN THE WORKPLACE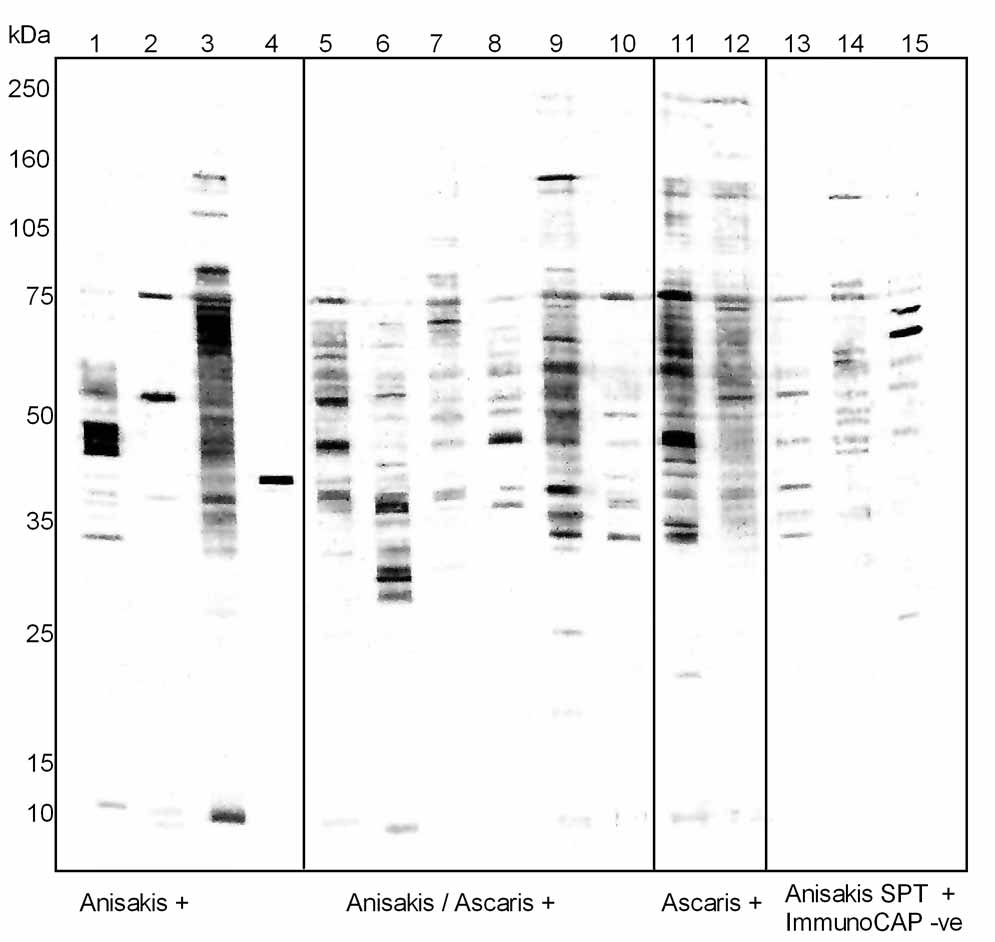 Fig. 2. IgE immunoblotting against Anisakis antigens using sera from 15 Anisakis-sensitised fish-processing work-ers. Workers 1-4 had higher specific IgE to Anisakis than to Ascaris, workers 5-10 had specific IgE to both Anisakisand Ascaris, workers 11-12 had higher levels of specific IgE to Ascaris than to Anisakis and workers 13-15 wereSPT positive to Anisakis but negative on ImmunoCAP tests.
blotting with deglycosylated Anisakis proteins or excre-
The major allergens of Anisakis (recognised by more
tory-secretory (ES) proteins to increase the specificity
than 50% of patients) are considered to be Ani s 1 and
of Anisakis diagnosis.24,33 However, to avoid misdiagno-
Ani s 7,38 although in one study Ani s 5 was recognised
sis due to cross-reactivity, it is ideally better to use puri-
by 49% of patients (41/84). The 24 kDa Ani s 1 is recog-
fied or recombinant allergens that are specific for
nised by 67-87% of patients with gastroallergic anisaki-
Anisakis-allergic patients.34 The identification of specif-
ic Anisakis allergens which could be used in tests such
individuals.23,39 This allergen is secreted by the worm
as ImmunoCAP, SPT, allergen microarray or immuno-
and shows homology to serine protease inhibitors. A
blotting will in the long term increase the specificity of
21 kDa isoform of Ani s 1 also exists.39 Ani s 1 is heat
stable and can act as a food allergen, causing reactionsafter ingestion of cooked fish. The other major allergen,
ANISAKIS ALLERGENS
Fig. 2. IgE immunoblotting against Anisakis antigens using sera from 15 Anisakis-sensitised fish-processing work-ers. Workers 1-4 had higher specific IgE to Anisakis than to Ascaris, workers 5-10 had specific IgE to both Anisakisand Ascaris, workers 11-12 had higher levels of specific IgE to Ascaris than to Anisakis and workers 13-15 wereSPT positive to Anisakis but negative on ImmunoCAP tests.
blotting with deglycosylated Anisakis proteins or excre-
The major allergens of Anisakis (recognised by more
tory-secretory (ES) proteins to increase the specificity
than 50% of patients) are considered to be Ani s 1 and
of Anisakis diagnosis.24,33 However, to avoid misdiagno-
Ani s 7,38 although in one study Ani s 5 was recognised
sis due to cross-reactivity, it is ideally better to use puri-
by 49% of patients (41/84). The 24 kDa Ani s 1 is recog-
fied or recombinant allergens that are specific for
nised by 67-87% of patients with gastroallergic anisaki-
Anisakis-allergic patients.34 The identification of specif-
ic Anisakis allergens which could be used in tests such
individuals.23,39 This allergen is secreted by the worm
as ImmunoCAP, SPT, allergen microarray or immuno-
and shows homology to serine protease inhibitors. A
blotting will in the long term increase the specificity of
21 kDa isoform of Ani s 1 also exists.39 Ani s 1 is heat
stable and can act as a food allergen, causing reactionsafter ingestion of cooked fish. The other major allergen,
ANISAKIS ALLERGENS



 33. Baeza ML, Rodriguez A, Matheu V, et al. Characterization of allergens
41. Iglesias R, Leiro J, Santamarina MT, Sanmartin ML, Ubeira FM.
33. Baeza ML, Rodriguez A, Matheu V, et al. Characterization of allergens
41. Iglesias R, Leiro J, Santamarina MT, Sanmartin ML, Ubeira FM.