Practical medical trials have confirmed the maximum effect of Levitra, whith a positive effect being observed in 99 of 100 patients kamagra uk Our internet store sells medicines produced in Indian pharmaceutical factories under licensed agreement.
Pii: s0140-6736(98)05012-0
Articles Effect of angiotensin-converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trial Lennart Hansson, Lars H Lindholm, Leo Niskanen, Jan Lanke, Thomas Hedner, Anders Niklason, Kimmo Luomanmäki,Björn Dahlöf, Ulf de Faire, Claes Mörlin, Bengt E Karlberg, P O Wester, Jan-Erik Björck, for the Captopril Prevention
with captopril than with conventional treatment (76 v s 9 5
events; relative risk 0·77 [0·57–1·04], p=0·092), the rate of
B a c k g r o u n d Angiotensin-converting-enzyme (ACE) inhibitors
fatal and non-fatal myocardial infarction was similar (162 v s
have been used for more than a decade to treat high blood
161), but fatal and non-fatal stroke was more common with
pressure, despite the lack of data from randomised
captopril (189 vs 148; 1·25 [1·01–1·55]. p=0·044).
intervention trials to show that such treatment affects
I n t e r p r e t a t i o n Captopril and conventional treatment did not
cardiovascular morbidity and mortality. The Captopril
differ in efficacy in preventing cardiovascular morbidity and
Prevention Project (CAPPP) is a randomised intervention
mortality. The difference in stroke risk is probably due to the
trial to compare the effects of ACE inhibition and
lower levels of blood pressure obtained initially in previously
conventional therapy on cardiovascular morbidity and
treated patients randomised to conventional therapy.
mortality in patients with hypertension. Lancet 1999; 353: 6 1 1 – 1 6 M e t h o d s CAPPP was a prospective, randomised, open trial
with blinded endpoint evaluation. 10 985 patients were
enrolled at 536 health centres in Sweden and Finland.
Patients aged 25–66 years with a measured diastolic blood
pressure of 100 mm Hg or more on two occasions were
Angiotensin-converting-enzyme (ACE) inhibitors areused widely in the treatment of high blood pressure.
randomly assigned captopril or conventional antihypertensive
Guidelines for the management of hypertension issued by
treatment (diuretics, -blockers). Analysis was by intention-
WHO and the International Society of Hypertension,
to-treat. The primary endpoint was a composite of fatal and
class ACE inhibitors as suitable for first-line treatment,
along with diuretics and -blockers. Guidelines issued by
the Joint National Committee in the USA used to state
F i n d i n g s Of 5492 patients assigned captopril and 5493
the same thing, but more recent versions of these
assigned conventional therapy, 14 and 13, respectively,
guidelines have not recommended ACE inhibitors as first-
were lost to follow-up. Primary endpoint events occurred in
line treatment. This change reflects the fact that no data
363 patients in the captopril group (11·1 per 1000 patient-
from prospective and randomised trials in hypertensive
years) and 335 in the conventional-treatment group
patients have shown that ACE inhibitor treatmentprotects against cardiovascular morbidity and mortality.
( 1 0 · 2 per 1000 patient-years; relative risk 1·05 [95% CI
There has been concern about the safety of newer
0·90–1·22], p=0·52). Cardiovascular mortality was lower
antihypertensive agents and whether they give the same
benefits as diuretics and -blockers; such concern has
Department of Public Health and Social Sciences, University of
focused on calcium antagonists but not ACE inhibitors. Uppsala, Uppsala, Sweden (Prof L Hansson MD); Department of
The Captopril Prevention Project (CAPPP) was designed
Public Health and Clinical Medicine (Prof L H Lindholm MD) and
as a prospective intervention trial to compare the
Department of Medicine (Prof P O Wester MD), Umeå University
potential benefits to cardiovascular morbidity and
Hospital, Umeå, Sweden; Department of Medicine, Kuopio
mortality of a regimen based on the ACE inhibitor
University Hospital, Kuopio, Finland (Prof L Niskanen MD); Department of Statistics, Lund University, Lund, Sweden
captopril with a conventional antihypertensive regimen of
(Prof J Lanke PhD); Department of Clinical Pharmacology,
diuretics or -blockers. For ethical reasons, a long-term
Sahlgrenska University Hospital, Gothenburg, Sweden
comparison with placebo was not done.
(Prof T Hedner MD); Bristol-Myers Squibb, Stockholm, Sweden
The scientific background and rationale of the CAPPP
(A Niklason MB, C Mörlin MD, J-E Björck MB); Department of
study have been reported elsewhere.5 Observations on
Medicine, Helsinki University Central Hospital, Helsinki, Finland
intermediary endpoints, which were available when the
(Prof K Luomanmäki MD)); GU Clinical Research Institute,
study was planned in the late 1980s, suggested that an
Gothenburg, Sweden (B Dahlöf MD); Department of Cardiovascular
antihypertensive regimen based on an ACE inhibitor
Research, Karolinska Hospital, Stockholm, Sweden
might offer benefits equal to or greater than those of
(Prof U de Faire MD); and Department of Medicine, University Hospital, Linköping, Sweden (Prof B E Karlberg MD)
conventional antihypertensive treatment with diuretics, -blockers, or both.6 ACE inhibitors help to reverse left-
Correspondence to: Prof Lennart Hansson, Division of Clinical
ventricular hypertrophy,7,8 itself a powerful indicator of
Hypertension Research, Department of Public Health and SocialSciences, University of Uppsala, Box 609, S-751 25 Uppsala,
patients with left-ventricular dysfunction,11,12
THE LANCET • Vol 353 • February 20, 1999
Figure 1: Trial profile
favourable metabolic effects,13 and help to maintainquality of life.14 More recently, benefits of ACE inhibitionhave been shown in patients with diabetic nephropathy15and in diabetic patients in general.16 ACE inhibitors also
Figure 2: Blood pressure during study
maintain renal function in patients with primary
Open Blinded Endpoint), which is similar to routine clinical
hypertension,17,18 which strengthens the hypothesis that a
practice. Men and women aged 25–66 years who had treated or
therapeutic regimen based on ACE inhibitors in the
untreated primary hypertension were included in the trial if their
treatment of primary hypertension could reduce the risk
diastolic blood pressure was 100 mm Hg or higher on two
of cardiovascular morbidity and mortality.
separate occasions. Exclusion criteria were secondaryhypertension, serum creatinine concentration of more than
150 mol/L, and disorders that required treatment with
-blockers. Eligible patients were randomly assigned captopril
treatment or conventional antihypertensive treatment with
The CAPPP trial, at 536 health centres in Sweden and Finland,
diuretics, -blockers, or both. The initial dose of captopril was
used the design of the PROBE study19 (Prospective Randomised
50 mg daily given in one or two doses. In the group receivingconventional treatment, atenolol and metoprolol were the most
Characteristic Captopril Conventional
commonly used -blockers, and hydrochlorothiazide and
treatment treatment
bendrofluazide the most common diuretics. The initial dose of
(n=5492) (n=5493)
atenolol and metoprolol was 50–100 mg once daily. Demographic M/F Characteristic Previously untreated (n=5245) Diabetes (n=572) Clinical Demographic Clinical Medical history Medical history
Data are number of patients or *mean (SD).
Data are number of patients or *mean (SD).
Table 2: Baseline characteristics of previously untreated
Table 1: Baseline characteristics patients and of patients with diabetes at baseline
THE LANCET • Vol 353 • February 20, 1999
Event (n) Captopril group Conventional group
Table 3: Patients with events during follow-up by treatment group
WHO criteria, and required at least two abnormal fastingglucose values or, if not unequivocal, confirmation by an oralglucose-tolerance test. The CAPPP study was approved by ethics
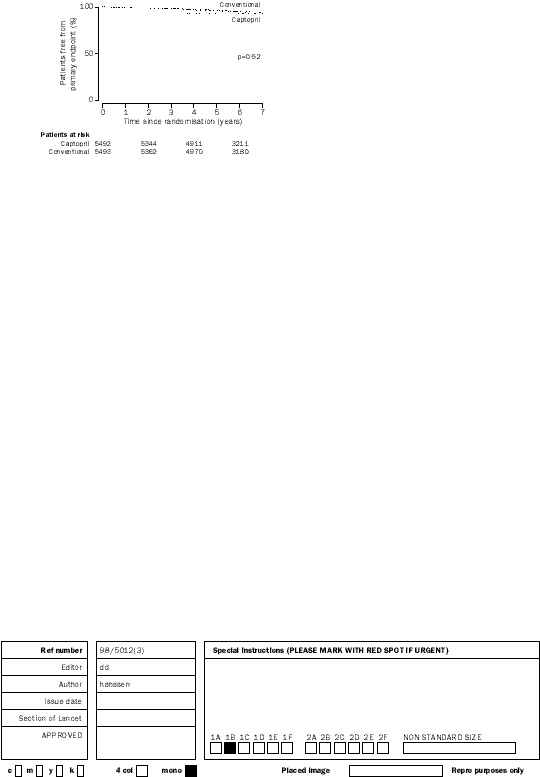
Figure 3: Patients remaining free from primary endpoint
Hydrochlorothiazide was given as 25 mg once daily, andbendrofluazide as 2·5 mg once daily. The randomisation
sequence was generated by computer and conveyed to the
Analysis was by intention to treat. The CAPPP study was
investigators by means of sealed numbered envelopes, one for each
designed to have an 80% power of detecting a 20% reduction in
patient, with instructions to use the envelopes in numerical order.
the rate of primary endpoints in a two-sided test at 5%
Blood pressure was measured with the patient supine by
significance. 640 primary events were required in the two groups
means of conventional mercury sphygmomanometers. The cuffs
combined. For each patient, only the first occurrence of primary
contained a rubber bladder with dimensions of 12ϫ35 cm.
endpoint was included in the analysis. Cox regression analysis
Larger cuffs were used if necessary. We calculated the mean of
used time since randomisation as a non-parametrically modelled
two measurements of blood pressure made to the nearest 2 mm
time variable. The model was adjusted for age at randomisation,
Hg. The goal of treatment was a supine diastolic blood pressure
sex, diabetes, and systolic blood pressure at randomisation. The
of 90 mm Hg or less. To reach this goal, the treatment dose
study group included both previously untreated patients and
could be increased to 100 mg once or twice daily in the captopril
patients receiving antihypertensive treatment before
group, and if necessary a diuretic was added. In the group that
randomisation, and we did not include a washout period.
received conventional treatment, an optimum dose of -blocker
We therefore had to account for baseline differences in the
or diuretic was used. The investigators were free to choose
model. We included baseline systolic blood pressure, a factor
suitable conventional treatment, and the diuretic and the
‘previously untreated’, and the product of these factors in the
-blocker could be combined. A calcium antagonist could be
model. In the on-treatment analysis a patient was classified as on
added to the treatment regimen in both treatment groups.
treatment for as long as he or she took the intended medication
The primary endpoint was the combination of fatal and non-
and no other medication. All calculations used Stata software
fatal myocardial infarction and stroke, and other cardiovascular
deaths. Primary events and most secondary events were assessedby an independent endpoint committee from which the
treatment allocation was concealed. Secondary endpoints were
11 018 patients were enrolled in the study, but 33 were
new or deteriorated ischaemic heart disease and congestive heart
excluded because of their age. Of the remaining 10 985
failure, atrial fibrillation, diabetes mellitus, transient ischaemic
patients, 5492 were randomly assigned captopril
attacks, and death from all causes. A diagnosis of acute
treatment and 5493 were randomly assigned conventional
myocardial infarction required that at least two of the following
treatment (figure 1). Follow-up lasted for a mean of 6·1
criteria were met: central chest pain for more than 15 min;transient increase in serum concentrations of enzymes indicating
years: a total of 67 239 patient-years were recorded. Only
myocardial damage; and electrocardiographic changes typical of
27 (0·25%) patients were lost to follow-up.
myocardial infarction. A diagnosis of fatal myocardial infarction
Baseline characteristics (table 1) and effects on blood
required the same criteria as a non-fatal acute myocardial infarct,
pressure have been described elsewhere.20 Blood pressure
or a statement of that diagnosis in hospital or necropsy reports.
at baseline was higher in the captopril group than in the
Diagnosis of stroke required typical symptoms or signs of
group that received conventional therapy, both among
remaining neurological deficit, with sudden onset and
previously untreated patients (166·6/103·6 vs 163·3/101·2
persistence for more than 24 h. Diagnosis of transient ischaemic
mm Hg, p<0·0001 in both cases) and among those
attacks required symptoms and signs of neurological deficit with
already on antihypertensive treatment (157·4/96·2 vs
sudden onset but with a duration of less than 24 h. Diagnosis of
156·2/95·4 mm Hg; p=0·025 and p=0·001, respectively,
fatal stroke required the same criteria as a non-fatal stroke, or astatement of that diagnosis in hospital records or necropsy
figure 2). Diabetes mellitus at baseline was more
reports. Diagnosis of diabetes was made according to
common in the captopril group than in the group
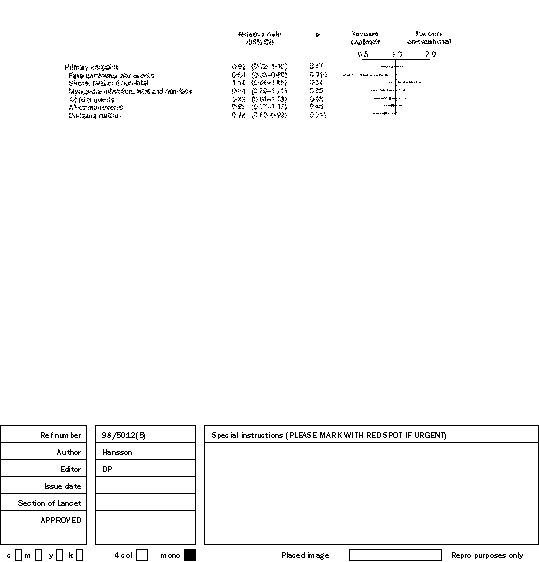
treatment (table 2). The primary endpoint(fatal
myocardial infarction, strokeand other cardiovasculardeaths) did not differbetween the two treatmentgroups (relative risk 1·05;
p=0·52, figures 3, 4). Numbers of the individual
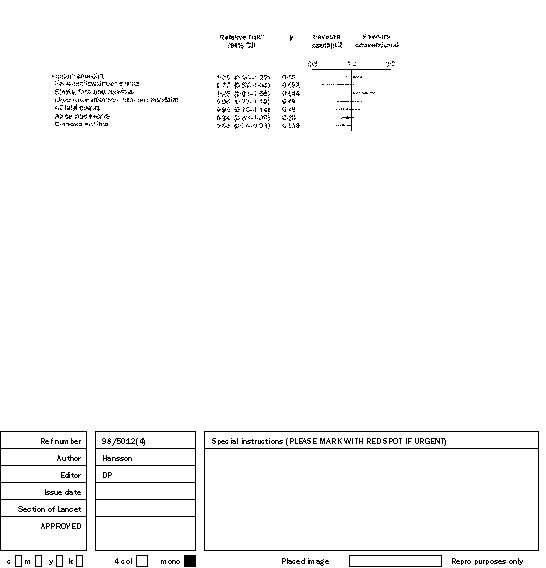
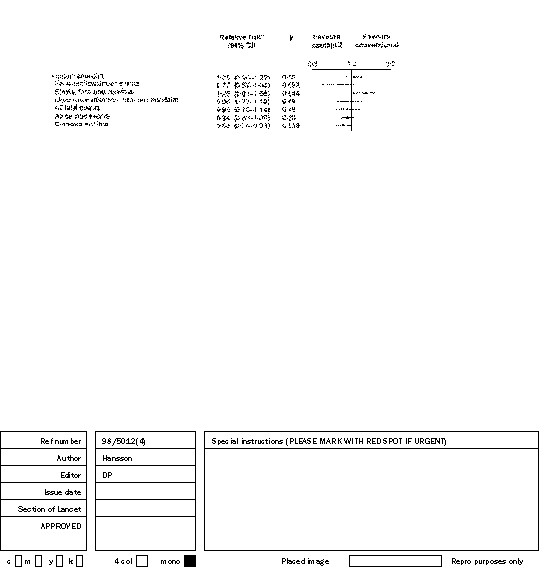
Figure 4: Relative risk of captopril vs conventional therapy *Adjusted for age, sex, diabetes, systolic blood pressure, and previous treatment.
THE LANCET • Vol 353 • February 20, 1999
We corrected our data for imbalance in blood pressure at
Relative risk (95% CI)*
baseline, sex, and the prevalence of diabetes in the
analyses. Centralised randomisation by fax21 would have
been preferable, but this procedure was not standard
Myocardial infarction, fatal and non-fatal
10 years ago, when this study was planned.
The proportion of patients lost to follow-up (0·25%) is
not as low as that of the STOP-Hypertension trial (0),22
*Adjusted for age, sex, diabetes, systolic blood pressure, and previous treatment.
but much lower than that of the MRC study in older
Table 4: On-treatment analysis: relative risk of captopril vs
patients (25%).23 The small number of patients lost to
conventional therapy
follow-up could not have affected the results of our study,since the loss was evenly distributed between the two
Cardiovascular mortality, defined as fatal stroke and
treatment groups (14 vs 13). Complete information on
myocardial infarction, sudden death, and other
primary events was available for the remaining patients.
cardiovascular death, was slightly lower in the captopril
The two treatment regimens had virtually the same
group than in the conventional group (0·77; p=0·092).
effect on blood pressure, although blood pressure
Fatal and non-fatal strokes were more common in the
measurements were slightly but significantly higher in the
captopril group (1·25; p=0·044). The rates of fatal and
captopril group throughout the study (figure 2). Almost
non-fatal myocardial infarction were similar in the two
all of the previously treated patients had been taking
diuretics, -blockers, or both, and were accustomed to
Analyses of secondary outcomes (figure 4) showed that
that kind of therapy, whereas captopril was in most
total mortality did not differ between the two treatment
instances a new therapy. Target blood pressure (diastolic
groups (0·93; p=0·49), and the incidence of diabetes was
blood pressure 90 mm Hg) was more rapidly achieved in
lower in the captopril group than in the conventional
the conventionally treated group than in the captopril
group (0·86; p=0·039). The rates of all cardiac events—fatal
group during the first 6–12 months of the study
and non-fatal myocardial infarction, other cardiovascular
(figure 2), although this effect was not noted for
deaths and sudden deaths, ischaemic heart disease,
previously untreated patients. Our study would have been
congestive heart failure, atrial fibrillation—did not differ
improved if we had included only previously untreated
between the two treatment groups (0·94; p=0·30).
patients, but recruitment of a large enough sample would
On-treatment analysis was also done. No new
differences between groups were shown, although the
Almost equal numbers of patients began captopril
results that were significant by intention-to-treat were
treatment once daily (48%) and twice daily (52%), but
more significant in the on-treatment analyses (table 4).
patients were switched between these two regimens
There was no difference between groups in blood
during the trial. Moreover, patients were not randomly
pressure related to cardiovascular mortality or morbidity,
assigned once-daily or twice-daily treatment. These
or in comparisons between once-daily and twice-daily
factors preclude meaningful analysis of outcomes in
Separate subgroup analyses were done for patients with
The treatment regimens did not differ in terms of
diabetes at baseline and for previously untreated patients
prevention of the primary endpoint, but the risk of stroke
(figure 5, 6). In both of these groups, captopril was as
was lower with conventional than with captopril therapy.
effective in preventing cardiovascular events as in the
This finding could be the result of non-adjustment for
high blood pressure measurements at baseline and
throughout the study in the captopril group, or a more
Our conventional randomisation procedure, using sealed
frequent history of stroke and transient ischaemic attacks
envelopes, resulted in an imbalance between groups at
in that group than in the group assigned conventional
baseline in terms of the blood pressure measurements.
treatment. A difference of 2 mm Hg could account for a
15% difference in risk ofstroke and transientischaemic attack.24
diabetic patients bloodpressure measurements atbaseline were identical inthe two treatment groupsand the incidence of stroke
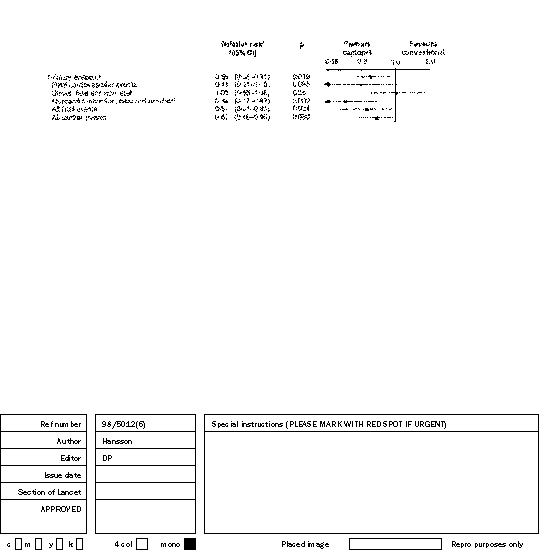
Figure 5: Relative risk in previously untreated patients (n=5245)
*Adjusted for age, sex, diabetes, and systolic blood pressure.
fatal strokes did notdiffer significantly in the
conventional): if therereally was an increased riskof stroke in the captoprilgroup, there should havebeen a proportionalincrease in both fatal and
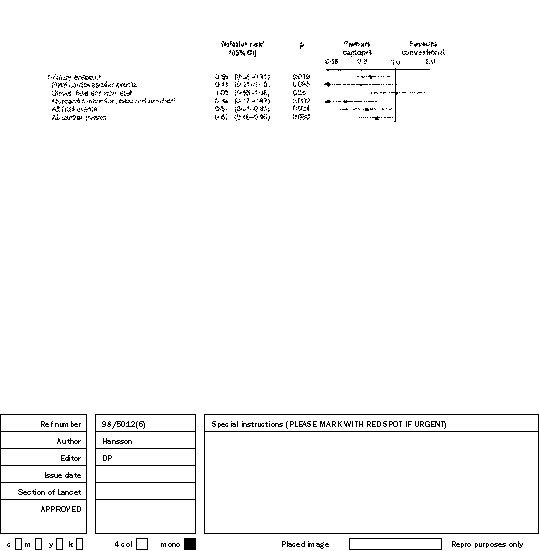
Figure 6: Relative risk in patients with diabetes mellitus at baseline (n=572)
*Adjusted for age, sex, systolic blood pressure, and previous treatment.
THE LANCET • Vol 353 • February 20, 1999
term follow-up data from the Glasgow Blood Pressure
between regimens might not be apparent. By contrast,
Clinic showed that the reduction in fatal stroke
among those previously untreated, both regimens would
associated with ACE inhibitors was at least as good as
be new to the patients and the difference in compliance
that associated with non-ACE inhibitors.25
discussion of this issue can be expected when the results
of the STOP-Hypertension-2 study become available,26 in
The overall results of the CAPPP study suggest than an
which hypertensive patients were randomly assigned one
antihypertensive regimen based on ACE inhibitors is as
of the three therapeutic options: conventional treatment
effective as conventional treatment with diuretics,
(diuretics, -blockers), calcium antagonists, or ACE
-blockers, or both in prevention of cardiovascular
inhibitors, with cardiovascular mortality as the primary
morbidity and mortality, possibly less effective in the
prevention of stroke, and most probably more effective in
There were fewer major cardiovascular events in the
the prevention of diabetes. This finding is of particular
captopril group, in line with our expectation of the effect
importance because recent studies have emphasised that
of captopril on intermediate endpoints.5,15–18 Significantly
both therapies have the same total treatment cost.33–35
fewer patients developed diabetes in the captopril group
than in the conventional group. This effect may be
Steering committee—L Hansson, J-E Björck, B Dahlöf, U de Faire,
attributed to the positive effect of captopril on insulin
T Hedner, B E Karlberg, J Lanke, L H Lindholm, K Luomanmäki,
sensitivity during long-term antihypertensive treatment,13
C Mörlin, L Niskanen, P O Wester. Endpoint committee—G Härtel, P Siltanen, K Swedberg, A Terent.
although studies of other ACE inhibitors have not
Endpoint secretary—A Holmner. Safety committee—L Erhardt, M Kupari, T Thulin, P-O Bendahl
diabetes in the captopril group should have positive
(statistician). Data management—B Slaug.
implications for long-term cardiovascular prognosis.
Patients with diabetes at baseline had a significantly
Sweden—P-O Andersson, J Asplund, A Dahlqvist, B Fagerberg, G Frithz,
lower rate of the primary endpoint and of fatal
B-G Hansson, A Hägg, S A Jonsen, T Kahan, B Carlberg, B EKristensson, J Kuylenstierna, H Larsson, B Lindström, I Mattiasson,
cardiovascular events in the captopril group than in the
B-H Möller, O R Nilsson, H Stakeberg, A Svensson, K Tolagen,
conventional group. There was a 66% lower rate of fatal
and non-fatal myocardial infarctions in the captopril
Finland—A Lehtonen, M Lilja, M Nikkilä, J Partanen.
group than in the conventional group. The frequency of
InvestigatorsSweden—H Aagaard, G Abrahamsson, T Ahlberg, H Åhlander, N Ahlén,
all cardiac events and total mortality was also significantly
G Ahlepil, E Ahlzén, L-G Ahnell, K Aljaderi, G Almqvist, M Alvin,
lower in the captopril group than in the conventional
B Andersson, G Andersson, H Andersson, I Andersson, M André,
group. These findings are similar to those of the subgroup
A Anglemo, S Anker, C Appelgren, K Arnman, G Asplund, B Atmer,C Aurelius, G Bartfay, E Basilier, L Berg, M Berg, M Bergfeldt,
analysis of the ABCD (Appropriate Blood Pressure
A Berglund, B Bergman, B-M Bergman, B Bergstad, R Bergström,
Control in Diabetes) study,16 and they strengthen the
J-E Billner, L Björkman, I Björkvald, S Blanking, U Blomqvist,
impression that an antihypertensive regimen based on
L Bodegård, S Bojesen, I Boman, O Borgholst, M Boström, G Bredmose-Hansen, M Brian, J Brun, B Bystritski, S Byström,
ACE inhibitors is particularly appropriate for the
E Bög-Hansen, S-M Carlsson, M Cech, B Christensen, O Christensen,
treatment of diabetic patients with hypertension.
A Dahl, G Dahlberg, G Dahlén, C Dahlin, A Dahlman, M Dalemar,
On the other hand, the UK Prospective Diabetes Study
L Duca, T Dyrborn, R Dziamski, Å Edlund, C Edström, M Edward,
(UKPDS 39)30 showed no advantage for captopril over
A Egilsson, T Ehn, M Ehnebom, M Ekberg, K Ekenbratt, S Ekesrydh,T Ekman, H Ekström, A Elfstrand, T Elfstrand, M Elm, K-G Enander,
atenolol in lowering of the risk of macrovascular and
M Enander, J Engborg, C Engstrand, G Engström, U-B Ericsson,
microvascular diabetic complications. This finding
V Eriksen, S Eriksson, U Eriksson, C Eskilson, C Fabian, L Falk,
suggests that lowering of blood pressure per se may be
G Filipsson, B-C Flensner, C Floom, I Fogelberg-Abrah, R Forrest, P-G Franke, B Franzén, C Frederiksen, S Fredlund, G Frenkner,
more important than the choice of antihypertensive
J Frithiof, K Fröstrom, B Furunes, B Gebre-Georgies, A Gidlöf,
agent, although captopril was better tolerated than
D Gilstring, A Gonn, U Grandell, P Grangaard, R Grenholm,
atenolol by most patients.31 The effective lowering of
V D Gräslund, L Grönquist, C-L Gustafsson, P Gustafsson, P Hansson,P Hajslund-Hansen, H Hallberg, C Hallendal, L Hallin, G Hansen,
blood pressure in the UKPDS 39 trial was highly
B Hansson, B Hansson, T Havland, M Hedlund, I-L Hegestrand,
beneficial in diabetic patients, which confirms
S Hellerstedt, P Hellke, P Hellman, M Hellqvist, T Hermansson,
observations in the HOT study21 in which the excess risk
C Hersvall, K Hertell, O Herterich, M Hessel, C Heyman, H Hirsch,
associated with diabetes was negligible in patients in
L Hjelmaeus, I Hjärne, S Hofvendahl, B Hofverberg, S Hollenberg,U Hollertz, R Hollsten, G Holmberg, F Holmer, A Holmgren, A-L Hult,
whom diastolic blood pressure was lowered to 80 mm Hg
A Hult, A Hägerfors, C Höglund, T Höglund, J Höjer, B-G Idh,
S Ingelög, H Isaksson, M Ivermark, G Jansson, R Jansson, J Jarl,
Captopril was more effective in lowering the risk of
B-O Johansson, B Johansson, E Johansson, G Johansson, H Johansson, L-Å Johansson, N-E Johansson, Y Johansson, Å Johansson, B Johnson,
cardiovascular events, particularly fatal events, in the
L Jonsson, K Juul, C Jägerström, C Jägrén, H J Jörgensen, C Karkow,
previously untreated group than in the study population
E Karlsson, T Kjellström, G Klemetz, L Klockhoff, R Klötz, P Koritz,
as a whole. One factor that may help to explain the
H Kristoferson, P Kronmann, B Kuylenstierna, H Landström, I Lantz, A-K Larsson, G Larsson, K Larrson, M Larsson, R Larsson, R Larsson,
variation in findings between previously treated and
Å Larsson, L Leander, K Leetmaa, B Lenngren, M Lind, I Lindahl,
previously untreated patients is a difference in
R Lindbergh, H O Lindbergsson, U Lindblad, B Lindborg, P Linde,
compliance between captopril and the conventional
L Lindén, T Lindén, B Linder, B Linder, H Lindfors, I Lindgren,A Lindh, B-Å Lindhe, A-C Lindman, E Ljungberg, L Ljungdahl,
regimen. We did not investigate this factor, but Monane
P Lorenzon, V Lukic, U Lundahl, N Lundström, C Lydén, J Löfgren,
and colleagues32 showed that therapy with an ACE
T Löfgren, L Lönneborg, B Lönner, F Lönqvist, B Magnusson,
inhibitor had 1·9 times better compliance than therapy
P-O Magnusson, K Malmlöf, B Malmros, K Marcus, K Marits,
with diuretics in a large group of hypertensive patients.
S-E Mattisson, R Melefors, K Mokhtar, J Munch, J Månsson,C Mårtensson, L Måwe, A-M Möller, C-M Mölstad, H Nerell,
The UKPDS 39 trial also showed better compliance with
E Nermo-Lindqvist, P Nicol, E Nielsen, B Nilsson, C Nilsson, H Nilsson,
captopril than with atenolol (78% compliance with
I R Nilsson, I Nilsson, L Nilsson, S Nilsson, Ö Nilsson, D Norberg,
captopril, 65% atenolol, p<0·0001).30 In our study,
E Norberg, A Nordenström, U Nordström, I Norén, A-B Nyberg,B Nyman-Ericsson, J Näsström, B Odeberg, M Ögland, C Öhlund,
among previously treated patients well used to taking
U-K Öhlund, T Öhrn, I Örstig, B Östberg, L Östling, R Östlund,
antihypertensive treatment, a difference in compliance
B Olerud, L Olofsson, H Olsson, P M Ollson, P Ollson, S Palm, E Pavek,
THE LANCET • Vol 353 • February 20, 1999
B Pell, E Persson, E Persson, O Persson, R Persson, M Peterson, G Petri,
Levy D. Left ventricular hypertrophy: epidemiological insights from
B Pettersson, L Pettersson, J Polacek, B Polhem, M Przedpelska, J
the Framingham Heart Study. Drug 1988; 35 (suppl 5): 1–5.
Pärnerud, M Rados, J Ramnemark, O Robertsson, T Roffey, M Roman,
10 Levy D. Garrison RJ, Sagae DD, Kannel WB, Castelli WP. Prognostic
G Rose, A-S Rosenqvist, U Rosenqvist, Y Roth, I-B Roupe, M-L Ryber,
implications of echocardiographically determined left ventricular mass
U Ryber, M Rydvall, B Ryss, T Rådestad, M Samuelsson, A Sandanam,
in the Framingham Heart Study. N Engl J Med 1990; 322: 1561–66.
G Sandberg, P Sandru, A Segerstedt, G von Seth, Z Simeonova,
11 Pfeffer MA, Braunwald E. Moyé LA, et al, for the SAVE investigators.
B Sjöberg, L Sjöberg, A-K Sjöblom, V Sjögedal, P Sjörup, Å Sjöstrand,
Effect of captopril on mortality and morbidity in patients with left
A Skovgaard-Hansen, A-C Snygg, L Spång, A Stadelmann, A Stattin,
ventricular dysfunction after myocardial infarction. N Engl J Med
U Stattin, L Stavenow, P Steneryd, E Stockenvall, M Strand, S Strid,
1992; 327: 669–77.
O Strömstedt, T Sturesson, A-S Ståhl, I Ståhlberg, J Stålhammar,
12 Sharpe N, Murphy J, Smith H, Hannan S. Treatment of patients with
D Sundberg, E Sundequist-Stockh, B Sundin, T Svanberg,
symptomless left ventricular dysfunction after myocardial infarction.
M Svennebring, V Svensson, T Sülau, K Söderberg, R Sörnäs, C Tevell,
U Thelander, H Theobald, A Thorfinn, S Thorslund, S Thorslund,
13 Pollare T, Lithell H, Berne C. A comparison of the effect of
B Tilling, A Tisell, S Tracz, J Tunberg, G Tygesen, E Tönnesen,
hydrochlorothiazide and captopril on glucose and lipid metabolism in
T Ulvatne, M Ungerstedt, S Uppman, K Vetterskog, M Vlastos,
patients with hypertension. N Engl J Med 1989; 321: 868–73.
S Wadström, G Wahlberg, E Wahlund, T Walan, S Walander, K Wallén,B Wallentin, L Warselius, G Wedenmark, E Weiner, P Wendel,
14 Croogh, Levine S, Testa MA, et al. The effects of antihypertensive
therapy on the quality of life. N Engl J Med 1984; 314: 1657–64.
C Wersäll, B Westerdahl, B Westerlind, C Wetterhall, S Wide, K Wide-Andersson, T Wideluis, B Widén, U Wiklund, B Wilnier,
15 Lewis EJ, Hunsicker LG, Bain RP, Rohde RD, for the Collaborative
Study Group. The effect of angiotensin-converting-enzyme inhibition
Finland—J Aho, S Andersson, M Antila, T Anttila, M Aro, H Arola,
on diabetic nephropathy. N Engl J Med 1993; 329: 1456–62.
S Bergkulla, H Björkstam, P Ekberg, O Ervasti, M Ervelä, K Haapa,
16 Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford N, Schrrier
A Hakala, P Hakkarainen, A Haukijärvi, R Heikinheimo, K Heikkinen,
RW. The effect of nisoldipine as compared with enalapril on
I Heilala, K Heino, H Helenius-Reunanen, K Herttuainen, P Himanen,
cardiovascular outcomes in patients with non-insulin dependent
K Hirvonen, H-L Holmström, S Honkanen, T Honkanen, S Hovi,
diabetes and hypertension. N Engl J Med 1998; 338: 645–52.
M Hyvönen, M Hyvönen, K Hyytiäinen, J Hämäläinen, K Hämäläinen,
17 Himmelman A, Hansson L, Hansson B-G, et al. ACE inhibitors
T Hämäläinen, R Icén, H Ihalainen, P Ijäs, H Isotalus, R Jakka,
preserves renal function better than beta-blockers in the treatment of
P Jokinen, M Jussila, S Jyväsjärvi, T Kaitila, J Kallio, K Kallio, I Kantola,
essential hypertension. Blood Press 1995; 4: 85–90.
M Karhu, K Karjalainen, L Karjalainen, E Karonen, V Karskela,
18 Himmelman A, Hansson L, Hansson B-G, et al. Long-term renal
O Kauppinen, S Kekki, P Kemppainen, P Keränen, S Kilpeläinen,
preservation in essential hypertension: ACE inhibition superior to
J Kiuttu, P Kohonen-Jalonen, S Koistinen, J Komulainen, N Koponen,
beta-blockade. Am J Hypertens 1996; 9: 850–53.
M Kortesoja, H Kortesuo, S Koskela, K Koskimies, K Koskinen,
19 Hansson L, Hedner T, Dahlöf B. Prospective Randomized Open
S Kovalainen, H Kovanen, P Kuosmanen, E Kupiainen, J Kurola,
Blinded Endpoint (PROBE) Study; a novel design for intervention
E Kurttila, M Kuusela, M Kykkänen, T Kärki, U Laisi, H Lajunen,
trials. Blood Press 1992; 1: 113–19.
R Lampén, K Lehtonen, L Lehtovuori, T Leiviskä, P Lerssi,
20 Hansson L, Hedner T, Lindholm, L, et al, for the CAPPP Study
P Liimatainen, M Lilja, A Linna, A Linna, J Luikku, H Luokkamäki,
Group. The Captopril Prevention Projection (CAPPP) in hypertension:
E Luostarinen, Y Martikainen, K Marttila, E Mattila, J Mattila,
baseline data and current status. Blood Press 1997; 6: 365–67.
K Mattila, M Mattila, P Mattila, R Mauno, J Metso, T Metsälä,
21 Hansson L, Zanchetti A, Carruthers SG, et al, for the HOT Study
M Miettinen, M Mäkelä, T Mäkinen, K Mönkkönen, J-P Möttönen,
Group. Effects of intensive blood-pressure lowering and low-dose
P Nikander, L Niskanen, S Norola, J Nurmi, M Nurmiaho, T Nykänen,
aspirin in patients with hypertension: principal results of the
P Ojala-Tamminen, A Ojanen, M Ollinen, R Paajanen, H Palva, S Pentti,
Hypertension Optimal Treatment (HOT) randomised trial. Lancet
I Pietikäinen, T Piippo, A Piiroinen, L Pitkämäki, A Pohjamo,
1998; 351: 1755–62.
E Pohjasniemi, A Poropudas, S Pynnönen, H Rantanen, J Rantonen,
22 Dahlöf B, Lindholm LH, Hansson L, Scherstën B, Ekbom T, Wester
H Rasi, J Raustia, J Rekola, M Rissanen, T Rokka, P Romppanen,
P-O. Morbidity and mortality in the Swedish Trial in Old Patients
P Ruusulehto, R Rytkönen, P Räisänen, K Rönkä, M Rönty, K Saarinen,P Saarinen, T Saaristo, J-P Salonen, K Saloranta, P Saloranta,
with Hypertension (STOP-Hypertension). Lancet 1991; 338: 1281–85.
L Saukkoriipi, R Saurio, A Savolainen, J Sillanpää, N Snell, J Starck,
23 The MRC Working Party. Medical Research Council trial of
A Strandberg, S Sulosaari, B Sundström, M Sääksi, J Teirilä,
treatment of hypertension in older adults: principal results. BMJ 1992;
J Tervaharju, R Timoska, E Toivanen, P Tonteri, T Tuomaala,
304: 405.
M-L Tuominen, P Tuominen, S Tuominen, T Tähtinen, P Valanto,
24 Cook NR, Cohen J, Hekbert PR, Taylor JO, Hennekens CH.
R Vanamo, A Vehviläinen, J Viinikanoja, I Viitaniemi-Malmi, J Vinberg,
Implications of small reductions in diastolic blood pressure for primary
T Vitranen, K Ylitolonen. U Ylläsjärvi.
prevention. Arch Intern Med 1995; 155: 701–09.
25 McInnes GT, Holes DJ, Murray LS, et al. Do ACE inhibitors reduce
mortality in hypertensive patients? Amsterdam: ISH, June 1998 (abstr).
This study was supported by a grant from Bristol-Myers Squibb.
26 Lindholm LH, Hansson L, Dahlöf B, et al. The Swedish Trial in Old
Patients with Hypertension-2 (STOP-Hypertension-2): progress
References
report. Blood Press 1996; 5: 300–04.
Zanchetti A, Chalmers J, Arakawa K, et al. The 1993 guidelines for
27 Alleman Y, Baumann S, Jost M, et al. Insulin sensitivity in
the management of mild hypertension: memorandum from a
normotensive subjects during angiotensin converting enzyme
WHO/ISH meeting. Blood Press 1993; 2: 86–100.
inhibition with fosinopril. Eur J Clin Pharmacol 1992; 42: 275–80.
The 1988 Joint National Committee. The 1988 report of the Joint
28 Santoro D, Natali A, Palombo C, et al. Effects of chronic angiotensin
National Committee on Detection, Evaluation and Treatment of High
converting enzyme inhibition on glucose tolerance and insulin
Blood Pressure. Arch Intern Med 1988; 148: 1023–28.
sensitivity in essential hypertension. Hypertension 1992; 20: 181–91.
The Joint National Committe on Detection, Evaluation, and Treatment
29 Haenni A, Andersson PE, Lind L, Berne C, Lithell H. Metabolic
of High Blood Pressure. The fifth report of the Joint National
effects during lisinopril/bendrofluazide treatment: results from a
Committee on Prevention, Detection, Evaluation, and Treatment of
randomised, double-blind study with parallel groups. Milan: Sixth
High Blood Pressure (JNC V ). Arch Intern Med 1993; 153: 154–83.
European Society of Hypertension meeting, 1993 (abstr).
The Joint National Committee on Detction, Evaluation, and
30 UK Prospective Diabetes Study Group. Efficacy of atenolol and
Treatment of High Blood Pressure. The sixth report of the Joint
captopril in reducing risk of macrovascular and microvascular
National Committee on Prevention, Detection, Evaluation, and
complications in type 2 diabetes: UKPDS 39. BMJ 1998; 317: 713–20.
Treatment of High Blood Pressure (JNC VI ). Arch Intern Med 1997;
31 Mogensen CE. Combined high blood pressure and glucose in type 2
157: 2413–46.
diabetes: double jeopardy. BMJ 1998; 317: 693–94.
The CAPPP Group. The Captopril Prevention Project: a prospective
32 Monane M, Bohn RL, Gurwitz JH, Glynn RJ, Levin R, Avorn J. The
interventional trial of angiotensin converting enzyme inhibition in the
effects on initial drug choice and comorbidity on antihypertensive drug
treatment of hypertension. J Hypertension 1990; 8: 985–90.
compliance. Am J Hypertens 1997; 10: 697–704.
Collins R, Peto R, MacMahon S, et al. Blood pressure, stroke, and
33 McCombs JS, Nichol M, Newman CM, Sclar DA. The costs of
coronary heart disease—part 2: short-term reductions in blood
interrupting antihypertensive drug therapy in a medicaid population.
pressure: overview of randomised drug trials in their epidemiological
Med Care 1994; 32: 214–26.
context. Lancet 1990; 335: 827–38.
34 Hilleman DE, Nohiuddin SM, Lucas Jr BD, Stading JA, Stoysich AM,
Dahlöf B, Pennert K, Hansson L. Reversal of left ventricular
Ryschon K. Cost-minimization analysis of initial antihypertensive
hypertrophy in hypertensive patients: a metaanalysis of 109 treatment
therapy in patients with mild-to-moderate essential diastolic
studies. Am J Hypertens 1992; 5: 95–110.
hypertension. Clin Ther 1994; 16: 88–102.
Schmieder RE, Marttus P, Klingbeil A. Reversal of left ventricular
35 Elliot WJ. Costs associated with changing antihypertensive drug
hypertrophy in essential hypertension: a meta-analysis of randomized
monotherapy: “preferred” vs “alternative” therapy. Am J Hypertens
double-blind studies. JAMA 1996; 275: 1507–13.
1995; 8: 80A (abstr F11).
THE LANCET • Vol 353 • February 20, 1999
MANUAL DE CONVIVENCIA COLEGIO PARROQUIAL RINCON DE SUBA BASE LEGAL El (Consejo Directivo) Rector del Colegio Parroquial Rincón de Suba en uso de sus facultades y las que le confiere la Constitución Política , la Ley 115 y el Decreto 1860/94, el Código del Menor, ley a. Que es un deber junto con los demás estamentos del gobierno escolar, padres de familia, tomar las medidas conduce
Olie van blijdschap Ki Tisa - אשת יכ : "When you take" Parasha: Ki Tisa - אשת יכ: "Als je neemt"Torah : Exodus 30:11-34:35 Haftarah : 1 Kings 18:1-39 Gospel : Matthew 9:35-11:1 Thought for the Week Gedachte voor de Week The Sages teach that in the month of Adar, joyDe Wijzen leren dat in de maand Adar, de vreugdeincreases. In Adar we celebrate
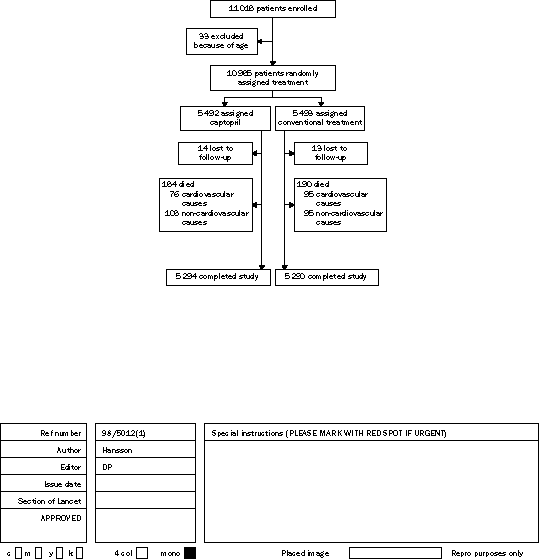
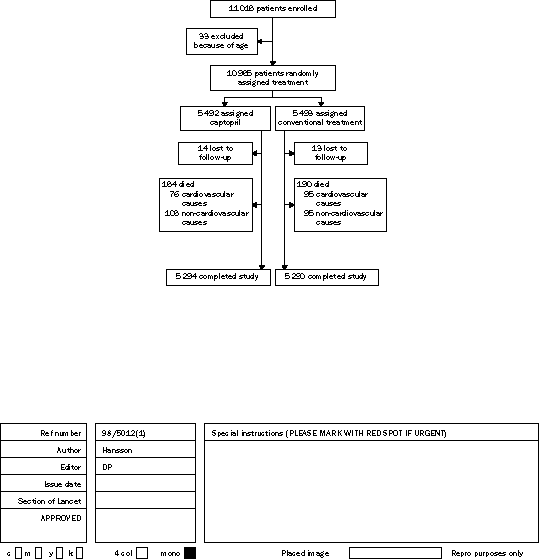
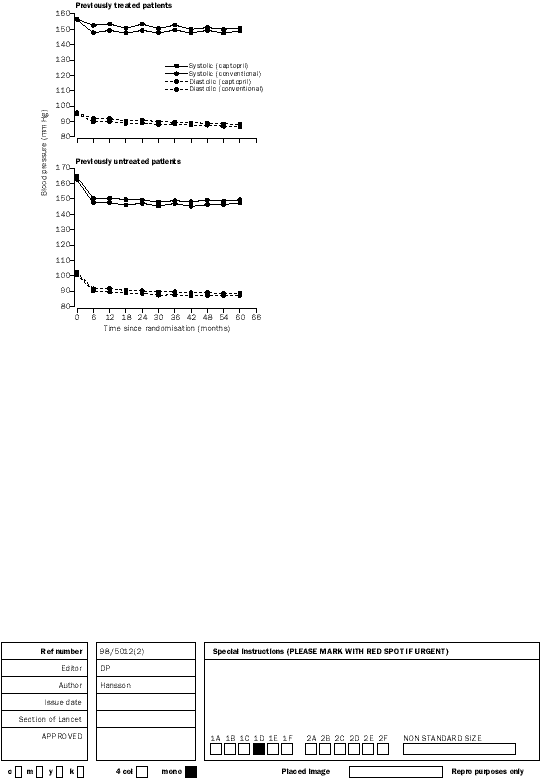
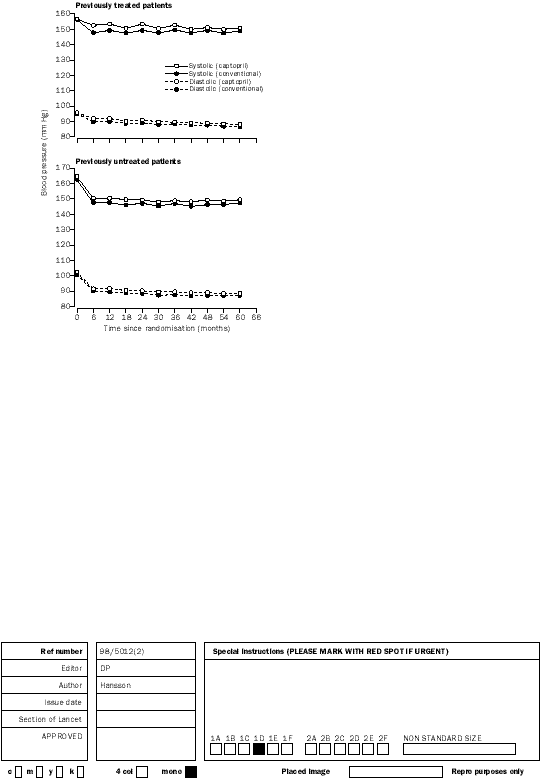 Figure 1: Trial profile
Figure 1: Trial profile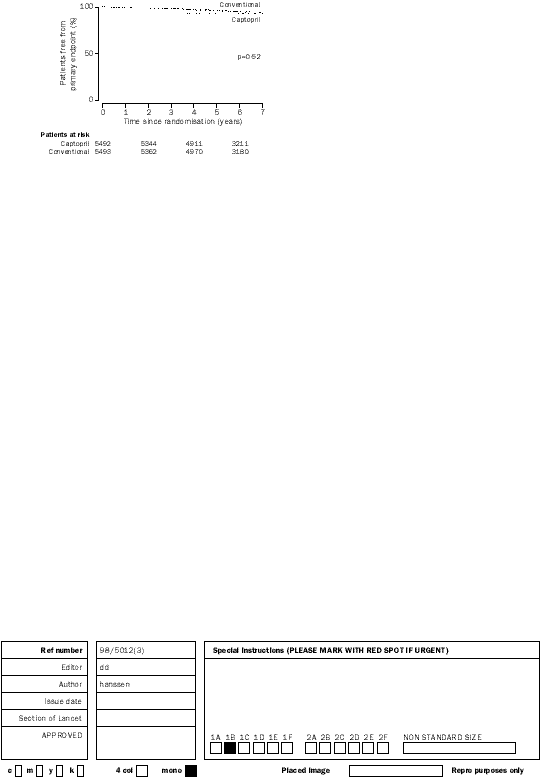
 Event (n)
Event (n)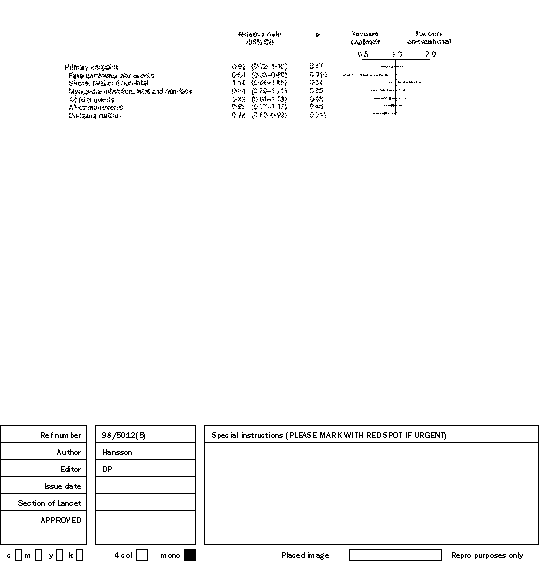
 We corrected our data for imbalance in blood pressure at
Relative risk (95% CI)*
We corrected our data for imbalance in blood pressure at
Relative risk (95% CI)*