Levitra has a minimal amount of contraindications which has increased its popularity kamagra uk You can buy quality certified medications from us at an affordable price.
Ahpma.co.uk
Incontinence Consumer article Too young to be incontinent? Think again!
You may be surprised to learn that, in the UK alone, an estimated 6 million adults cannot control their bladders as well they would likeconsidered a problem of later life, it affects many younger women, too. Researchers in New Zealand found that more than a third of new mothers were still experiencing some degree of urinary leakage three months after delivering their babiesmore surprisingly, a recent survey of 3536 US women aged 30 to 90 years found that urinary incontinence affected 45% - that’s almost one in two, of whom 28% were aged 30 – 39 years. Among these younger women, 8% describing their urinary leakage as severe. Figures are likely to be similar in the UK, as a postal survey of adults aged from 40 years found that 34% reported clinically significant urinary problem Stress incontinence
The commonest cause of female urinary leakage is stress incontinence. Despite its name, this is a physical rather than a psychological problem. It is due to weakness of the pelvic floor muscles which are slung, like a hammock, at the base of your pelvis to support your bladder, womb and lower bowel. Having weak pelvic floor muscles means that the neck of your bladder is no longer supported as well as usual, and starts to sag. This lack of support places strain on the natural valve mechanisms (sphincters) keeping your bladder closed, so that a sudden increase in pressure within the abdomen, as occurs during lifting, coughing, laughing, sneezing or running, for example, results in urinary leakage. Some cases are mild, with only slight damping, but a few women are devastated by a total loss of bladder control, which can occur on a daily basis. The pelvic floor muscles are especially prone to stretching during late pregnancy and child birth, so stress incontinence is especially common in women who have had difficult or multiple labours. It is also linked with general unfitness and overweight. While stress incontinence can cause problems at any stage of female adult life, symptoms tend to worsen after the menopause, when lack of oestrogen causes female tissues to thin and become less supportive. Another common cause of female urinary incontinence is an overactive bladder. The mechanism which controls bladder emptying in the central nervous system involves a simple ‘on-off’ switch that is under voluntary control. Normally, the bladder only contracts to force out urine when you choose to let it do so. Some cases of overactive bladder are thought to occur when muscle fibres in the bladder wall become over sensitive to stretch and start to contract prematurely, as urine accumulates and the bladder fills. This produces intense feelings of having to empty the bladder (urgency) and a need to pass urine more frequently than normal (frequency). As a result, around one in two people with an overactive bladder experience urge incontinence. In other cases, there may also be over sensitivity of nerve pathways so the “on” switch is activated when it should be “off”
Some women may have both an overactive bladder, and stress incontinence (eg when coughing or sneezing) so that a mixed pattern of urinary leakage occurs. Fact box: Urge incontinence is the most common type of incontinence in older people as it affects both men and women. Among women, however, it is the second most common form of incontinence, overall, after stress incontinence. Quality of life
Not surprisingly, urinary leakage can have a major effect on your quality of life. It may determine the way you plan your whole day, have a negative effect on your personal relationships and sex life, and even affect day-to-day tasks such as planning a trip to the shops. Attending special occasions such as weddings, travelling abroad with work, or going on holiday can also cause so many logistical problems that these activities may be avoided. As a result, urinary leakage can cause significant social, psychological, occupational, domestic, physical and sexual problems – especially when it is covered-up due to embarrassment, or a mistaken belief that you have to learn to live with it because nothing can be done to help. Urinary leakage doesn’t have to be a problem, however, as many solutions are now available as long as you can pluck up the courage to seek help. Treatments
Until recently, the main treatment options for stress incontinence have been pelvic floor exercises and surgery to support the bladder neck. The first drug treatment to receive a license in the UK to reduce urinary leakage from stress incontinence is now available, however. Yentreve (duloxetine) is thought to work by increasing the strength of muscle fibres controlling urine outflow from the bladder. Clinical trials have shown it can reduce urinary frequency by 60%. In one studywomen aged 33 to 75 years, who had severe incontinence (14 episodes per week, or more), one in five women who had received treatment were no longer interested in undergoing surgery to correct the problem. Similarly, Vesicare (solifenacin succinate) recently became available to help control bladder over-activity through a selective effect on special nerve receptors in the bladder wall. Research shows that 50% of people with urge incontinence can achieve continence again within 12 weeks of treatment. These advances mean that most women with urinary incontinence can have their condition improved and, in many cases, solved, by one of the measures mentioned above. Incontinence pads
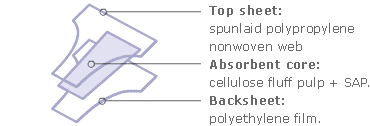
Incontinence pads are still the safest way to cope with leaks and to provide reassurance when undergoing medical treatment. Some absorbent pads are available on the NHS via your GP or local continence service. Depending on local budgets, however, you may need to buy pads yourself, especially if you want to use a brand not supplied by the health service. A wide range of absorbent pads for light incontinence is available in high street pharmacies and even in supermarkets. If you prefer, mail order services are also provided by manufacturers. Modern pads are available in a surprisingly large range of shapes and sizes in both disposable and reusable designs. They are an invaluable addition to your medical treatment, helping you lead a normal rather than a restricted life – even if leakage occurs regularly. Pads designed to cope with light incontinence are made to a different specification than sanitary pads, and have a higher absorbency which is typically ten times greater. The absorbent core is usually made from cellulose fluff pulp together with powdered superabsorbent polymers (SAP) that can quickly absorb many times their own weight of urine. The lining is typically a non-woven web of polypropylene that maintains a dry feel, so the pad can still be worn comfortably, even after it has absorbed a leak, although they should be changed before they become saturated. Some pads are available with a wetness strip to indicate when they need changing. Most pads also have a waterproof backsheet made of polyethylene film.
Incontinence pads are designed to absorb urine rapidly, and distribute it throughout the absorbent core. This locks moisture away from your skin and traps it to minimise any potential for odour. Pads are comfortable and discrete during wear, hygienic and help to deal with leaks without anyone else knowing what has happened. For light use, slim and unobtrusive pads can be slipped inside ordinary underwear and kept in place with an in-built adhesive strip or, if you prefer, can be worn inside stretch pants or special pants with a built-in pouch. If using pants with a waterproof backing or pouch, you should use pads without a waterproof backsheet. All-in-one nappy-style pads are also available, but are usually reserved for heavier urinary and/or faecal incontinence. Pads can be mixed and matched according to your needs – perhaps use a smaller pad that can be changed frequently during the day, and a more absorbent pad for single use throughout the night. For heavier users products shaped more like undergarments are also available.
Disposable pads should be bagged and binned when changed. If you choose washable, reusable products, you will need to consider how to transport and store these until they can be laundered. Acceptance The development of new medical treatments is helping people think differently about urinary incontinence. Just as the development of Viagra helped to bring erectile dysfunction into the limelight, the launch of new drug treatments for both stress and urge incontinence is helping to overcoming embarrassment about this common problem. More and more retail outlets are now selling adult absorbent hygiene products, and it is as easy to slip a pack of incontinence pads into your shopping trolley as it is to buy sanitary products and disposable baby nappies – all of which have undoubtedly contributed to social progress in terms of quality of life, dignity, comfort, convenience, reduction in household chores and skin health benefits. Don’t suffer in silence. Accept that you have a common problem and seek the help that is widely available – without embarrassment. Resources
Further information is available from: The Continence Foundation 307 Hatton Square 16 Baldwin Gardens London, EC1N 7RG Helpline: 0845 345 0165 (Monday to Friday, 9:30 am to 1:00 pm)
i http://www.continence-foundation.org.uk/symptoms-and-treatments/index.php
ii Wilson PD et al. 1996 Obstetric practice and the prevalence of urinary incontinence three months after delivery. Br J Obstet Gynaecol. 103(2):154-61.
iii Melville JL et al. 2005. Urinary Incontinence in US Women: A Population-Based Study. Arch Intern Med. 165(5):537-42.
iv Perry S et al. 2000. An epidemiological study to establish the prevalence of urinary symptoms and felt need in the community: the Leicestershire MRC Incontinence Study. Leicestershire MRC Incontinence Study Team. J Public Health Med. 22(3):427-34.
v de Groat WC A neurologic basis for the overactive bladder. Urology 1997; 50(6A Suppl) 36-52; discussion 53-6
vi Cardozo L et al. 2004. Pharmacological treatment of women awaiting surgery for stress urinary incontinence. Obstet Gynecol. 104(3):511-9.
vii Cardozo L 2004. Randomized, double-blind placebo controlled trial of the once daily antimuscarinic agent solifenacin succinate in patients with overactive bladder. J Urol. 172(5 Pt 1):1919-24.
For the use of a Registered Medical Practitioner or a Hospital or a Laboratory Only (Tirofiban Hydrochloride I.V. Injection) Composition: Each 10 ml contains: Tirofiban Hydrochloride equivalent to Tirofiban …5 mg Sodium Chloride I.P. … 0.9% w/v Water for Injection … q.s. Description: Tirofiban hydrochloride is non-peptide antagonist of the platelet glycoprotein (GP) llb/llla rece
id14147500 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com Lenovo ThinkPad R61e 7650 - C 540 / 1.86 GHz - RAM 1 GB - HDD 80 GB - DVD-Writer - GMA X3100 - Gigabit Ethernet - WLAN : 802.11a/b/g - Vista Business - 15.4" Widescreen TFT 1280 x 800 ( WXGA ) - TopSeller ThinkPad R61e is the coolest and
 Incontinence pads are still the safest way to cope with leaks and to provide reassurance when undergoing medical treatment. Some absorbent pads are available on the NHS via your GP or local continence service. Depending on local budgets, however, you may need to buy pads yourself, especially if you want to use a brand not supplied by the health service. A wide range of absorbent pads for light incontinence is available in high street pharmacies and even in supermarkets. If you prefer, mail order services are also provided by manufacturers. Modern pads are available in a surprisingly large range of shapes and sizes in both disposable and reusable designs. They are an invaluable addition to your medical treatment, helping you lead a normal rather than a restricted life – even if leakage occurs regularly. Pads designed to cope with light incontinence are made to a different specification than sanitary pads, and have a higher absorbency which is typically ten times greater. The absorbent core is usually made from cellulose fluff pulp together with powdered superabsorbent polymers (SAP) that can quickly absorb many times their own weight of urine. The lining is typically a non-woven web of polypropylene that maintains a dry feel, so the pad can still be worn comfortably, even after it has absorbed a leak, although they should be changed before they become saturated. Some pads are available with a wetness strip to indicate when they need changing. Most pads also have a waterproof backsheet made of polyethylene film.
Incontinence pads are designed to absorb urine rapidly, and distribute it throughout the absorbent core. This locks moisture away from your skin and traps it to minimise any potential for odour. Pads are comfortable and discrete during wear, hygienic and help to deal with leaks without anyone else knowing what has happened. For light use, slim and unobtrusive pads can be slipped inside ordinary underwear and kept in place with an in-built adhesive strip or, if you prefer, can be worn inside stretch pants or special pants with a built-in pouch. If using pants with a waterproof backing or pouch, you should use pads without a waterproof backsheet. All-in-one nappy-style pads are also available, but are usually reserved for heavier urinary and/or faecal incontinence. Pads can be mixed and matched according to your needs – perhaps use a smaller pad that can be changed frequently during the day, and a more absorbent pad for single use throughout the night. For heavier users products shaped more like undergarments are also available.
Disposable pads should be bagged and binned when changed. If you choose washable,
Incontinence pads are still the safest way to cope with leaks and to provide reassurance when undergoing medical treatment. Some absorbent pads are available on the NHS via your GP or local continence service. Depending on local budgets, however, you may need to buy pads yourself, especially if you want to use a brand not supplied by the health service. A wide range of absorbent pads for light incontinence is available in high street pharmacies and even in supermarkets. If you prefer, mail order services are also provided by manufacturers. Modern pads are available in a surprisingly large range of shapes and sizes in both disposable and reusable designs. They are an invaluable addition to your medical treatment, helping you lead a normal rather than a restricted life – even if leakage occurs regularly. Pads designed to cope with light incontinence are made to a different specification than sanitary pads, and have a higher absorbency which is typically ten times greater. The absorbent core is usually made from cellulose fluff pulp together with powdered superabsorbent polymers (SAP) that can quickly absorb many times their own weight of urine. The lining is typically a non-woven web of polypropylene that maintains a dry feel, so the pad can still be worn comfortably, even after it has absorbed a leak, although they should be changed before they become saturated. Some pads are available with a wetness strip to indicate when they need changing. Most pads also have a waterproof backsheet made of polyethylene film.
Incontinence pads are designed to absorb urine rapidly, and distribute it throughout the absorbent core. This locks moisture away from your skin and traps it to minimise any potential for odour. Pads are comfortable and discrete during wear, hygienic and help to deal with leaks without anyone else knowing what has happened. For light use, slim and unobtrusive pads can be slipped inside ordinary underwear and kept in place with an in-built adhesive strip or, if you prefer, can be worn inside stretch pants or special pants with a built-in pouch. If using pants with a waterproof backing or pouch, you should use pads without a waterproof backsheet. All-in-one nappy-style pads are also available, but are usually reserved for heavier urinary and/or faecal incontinence. Pads can be mixed and matched according to your needs – perhaps use a smaller pad that can be changed frequently during the day, and a more absorbent pad for single use throughout the night. For heavier users products shaped more like undergarments are also available.
Disposable pads should be bagged and binned when changed. If you choose washable,